Inflammatory Fibroid Polyp or Vanek Tumor as an Uncommon Cause of Adult Intussusception: Diagnostic and Surgical Considerations
Anaida Xacur Trabulce, Begoña Llaca Morfin, Gessner Casas Fuentes, Atl Simon Arias Rivera, Andoni Vicente Eguia

TL;DR
Inflammatory fibroid polyps, a rare benign tumor, can cause intestinal blockage in adults and require surgical removal for effective treatment.
Contribution
The study adds a new case and reviews 22 published cases to improve understanding and clinical awareness of inflammatory fibroid polyps.
Findings
A 69-year-old man's case showed successful treatment of jejunojejunal intussusception via laparoscopic surgery.
Histopathology confirmed the diagnosis of inflammatory fibroid polyps.
Review of 22 cases emphasizes the need for prompt surgical treatment to prevent complications.
Abstract
Inflammatory fibroid polyps (IFPs) or Vanek tumors are rare benign neoplasms of the gastrointestinal tract, with an unknown pathogenesis, that, despite their harmless nature, can lead to small bowel intussusception - a rare cause of intestinal obstruction in adults. In this article, we present the case of a 69-year-old man who arrived at the emergency department with vague abdominal discomfort. Imaging revealed a jejunojejunal intussusception caused by a polypoid mass, which was successfully treated through laparoscopic-assisted bowel resection. Histopathology and immunohistochemistry confirmed the diagnosis of IFPs. A comprehensive literature review was conducted, identifying 22 previously published cases to better understand the clinical profile and management of this rare condition. It highlights the importance of raising awareness among clinicians about this unusual disease so that…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
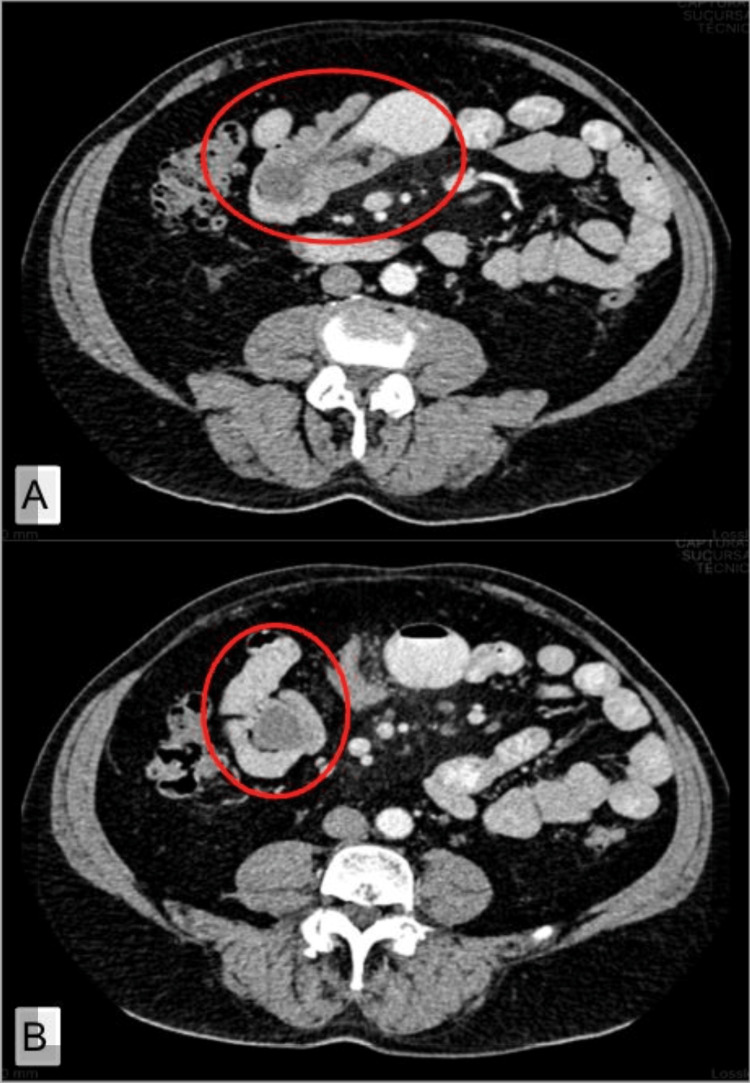 Figure 1
Figure 1 Figure 2
Figure 2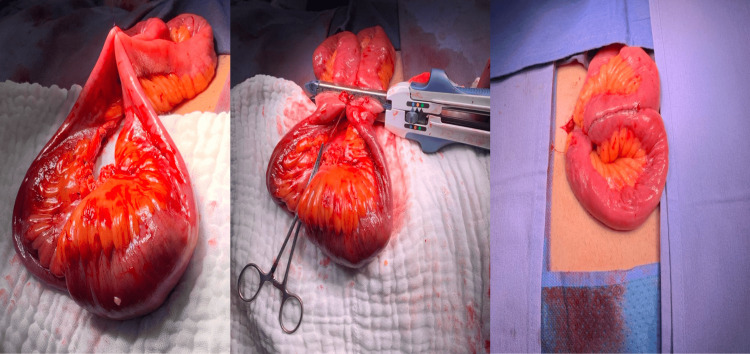 Figure 3
Figure 3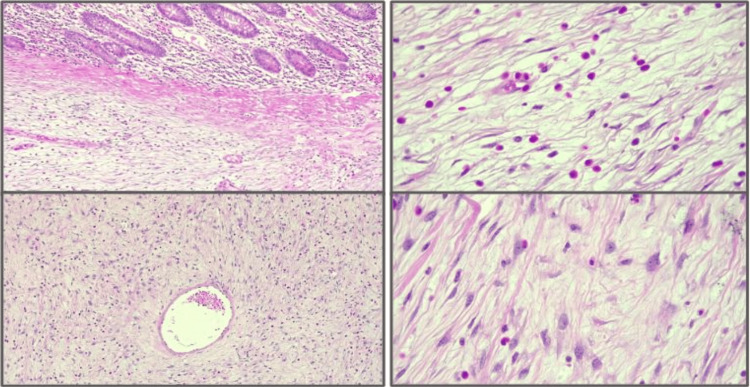 Figure 4
Figure 4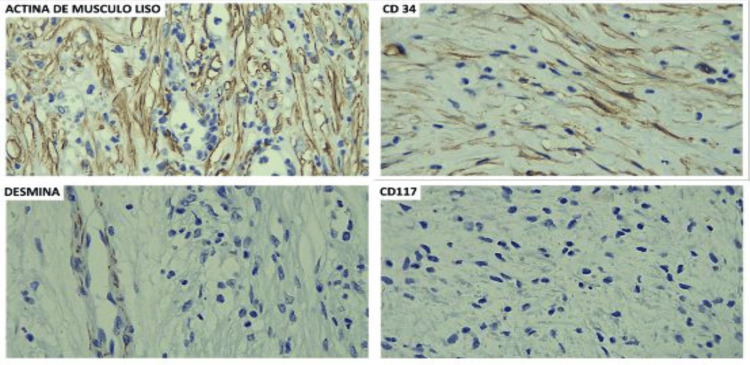 Figure 5
Figure 5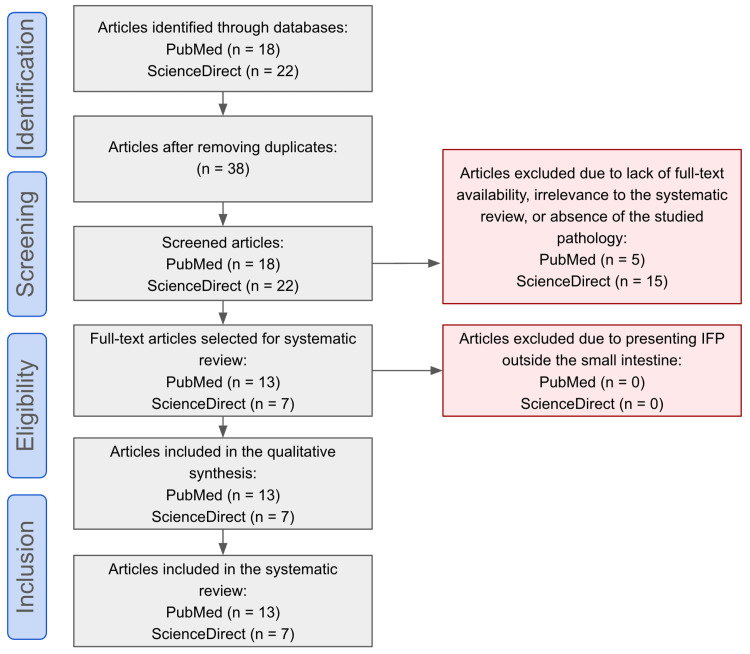 Figure 6
Figure 6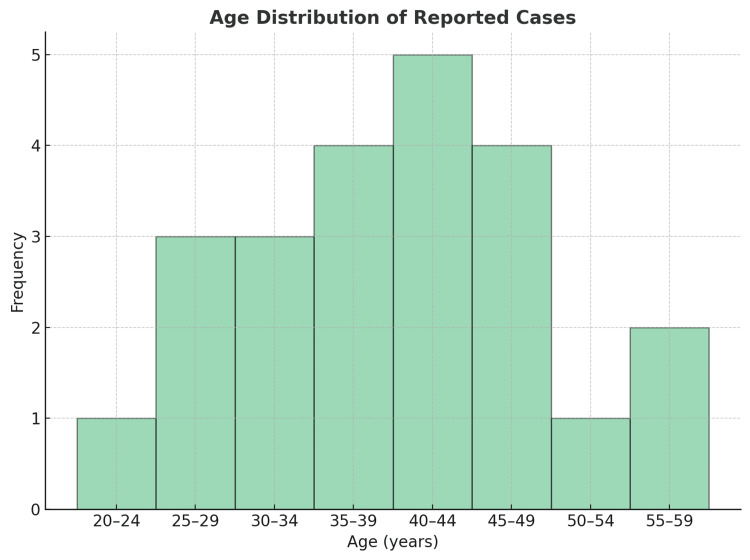 Figure 7
Figure 7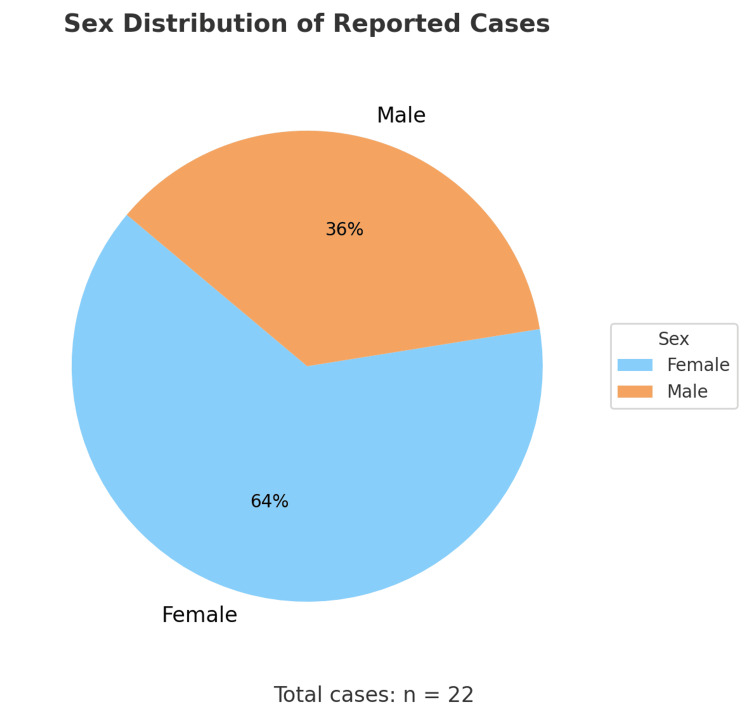 Figure 8
Figure 8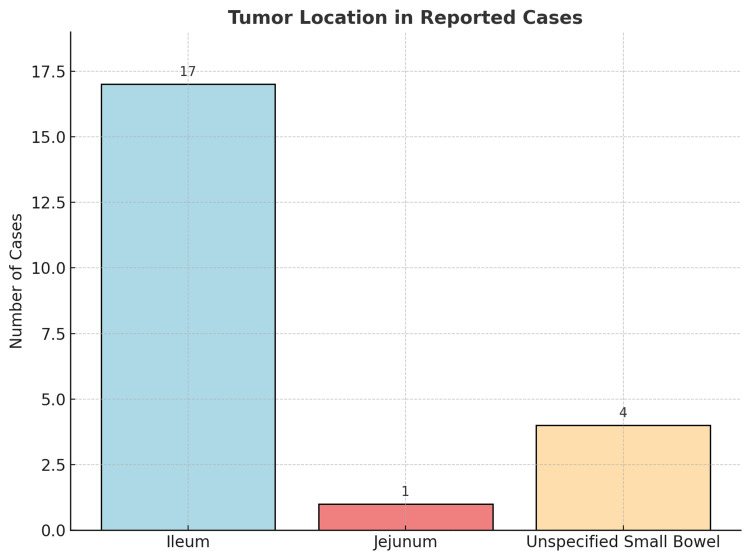 Figure 9
Figure 9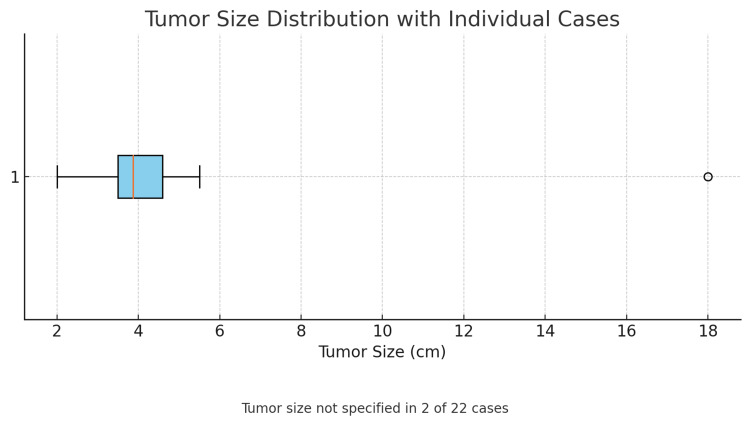 Figure 10
Figure 10| Reference | Age | Sex | Clinical Presentation | Palpable Mass | Radiological Tools | Immunohistochemistry | Surgical Approach | Location | Size |
| Chaima et al. [ | 35 years | Male | Abdominal pain for 2 weeks, intestinal obstruction for 3 days | No | Non-contrast abdominal CT: intestinal intussusception | CK7 (-), DOG1 (-) | Exploratory laparotomy + 30 cm bowel resection + side-to-side primary anastomosis | Ileum | 4 cm |
| Park et al. [ | 23 years | Male | Diffuse abdominal pain for 3 days progressing to epigastric pressure pain, constipation, nausea, and vomiting | No | Non-contrast abdominal CT: jejunojejunal intussusception | CD34 (+), CD117 (−), BCL-2 (−), DESMIN (−), SMA (−), S-100 (−), Ki-67 1–5% | Exploratory laparoscopy + intestinal resection + side-to-side linear stapled anastomosis | Jejunum | (1) 5 x 3 x 3 cm, (2) 2.5 x 2.3 x 1.2 cm |
| Johan et al. [ | 41 years | Male | Diffuse abdominal pain and distension for 1 month, followed by obstipation, nausea, fecaloid vomiting, weight loss and anorexia for 3 days | No | Contrast-enhanced abdominopelvic CT: ileo-ileal intussusception | CD34 (+), CD117 (-) | Exploratory laparotomy + bowel resection + primary anastomosis + mesenteric lymph node dissection | Ileum | 4 x 4 x 3.6 cm |
| Nonose et al. [ | 56 years | Female | Postprandial intermittent cramping abdominal pain for 45 days | No | Oral contrast-enhanced abdominopelvic CT: ileo-ileal intussusception | CD34 (+), CD117 (-), S100 (-), ACTIN (-), DESMIN (-) | Exploratory laparotomy + bowel resection + end-to-end primary anastomosis + peritoneal lavage | Ileum | 4.5 cm |
| Al Taei et al. [ | 47 years | Female | Cramping abdominal pain, nausea, and vomiting for 4 days | No | Contrast-enhanced abdominopelvic CT: ileo-ileal intussusception | Not available | Exploratory laparotomy + 16 cm bowel resection + side-to-side anastomosis | Ileum | 3.5 x 3 x 3 cm |
| Carvalho et al. [ | 41 years | Female | Cramping lower quadrant abdominal pain for 6 hours, nausea with one episode of vomiting and diarrhea | No | Abdominal ultrasound: positive for intestinal intussusception. Contrast-enhanced abdominopelvic CT confirmed bowel wall thickening of 35 mm | CD34 (+) | Exploratory laparoscopy + 24 cm bowel resection | Small intestine | 4.8 cm |
| Carvalho et al. [ | 51 years | Female | Cramping right upper quadrant abdominal pain for 2 months and nausea | No | Contrast-enhanced abdominopelvic CT: ileo-ileal intussusception | CD34 (+) | Exploratory laparotomy + 22 cm bowel resection | Ileum | 5.5 cm |
| Jan et al. [ | 60 years | Male | Generalized abdominal pain, predominantly in the left iliac fossa, moderate intensity, associated with nausea and anorexia | No | Simple abdominopelvic CT: ileo-ileal intussusception | CD34 (+) | Exploratory laparotomy + bowel resection + end-to-end primary anastomosis | Ileum | 4.6 x 3.6 cm |
| Maya et al. [ | 82 years | Female | Generalized abdominal pain and distension for 48 hours | No | Oral contrast-enhanced abdominopelvic CT: intestinal intussusception | CD34 (+), VIM (+), S100 (-), ACTIN (-), DESMIN (-) | Exploratory laparotomy + bowel resection + end-to-end primary anastomosis | Ileum | 5 cm |
| Neishaboori et al. [ | 40 years | Female | Progressive cramping abdominal pain, mostly postprandial, nausea and vomiting for 3 days | No | Abdominal ultrasound: positive for intestinal intussusception | CD34 (+) | Exploratory laparotomy + bowel resection + end-to-end primary anastomosis | Jejunum | 18 x 5 x 1 cm |
| Gadoura et al. [ | 32 years | Female | Epigastric abdominal pain, nausea, vomiting, and diarrhea for 2 weeks | No | Non-contrast abdominal CT: intestinal intussusception | Not available | Exploratory laparotomy + 80 cm bowel resection + end-to-end anastomosis + lymph node dissection | Ileum | 4 x 3 cm |
| Akbulut [ | 38 years | Female | Abdominal pain, nausea, and vomiting for 10 days | No | Abdominal ultrasound: positive for intussusception due to tumor mass | CD117 (-), SMA (-), DESMIN (-), S100 (-), CD34 (-) | Exploratory laparotomy + 20 cm bowel resection + end-to-end anastomosis | Ileum | 4 x 4 cm |
| Ivaniš et al. [ | 38 years | Not specified | Generalized abdominal pain localized to the right hemiabdomen, worse postprandially, with diarrhea and anorexia | No | Abdominal ultrasound: positive for intussusception due to tumor mass | Not available | Exploratory laparotomy + bowel resection | Small intestine | 3.5 cm |
| Forasté-Enríquez et al. [ | 58 years | Female | Cramping epigastric pain for 4 months associated with eating, weight loss (12 kg). Presented to ED with worsened pain, abdominal distention, diarrhea, nausea, vomiting | Yes | Contrast-enhanced abdominopelvic CT: ileo-ileal intussusception | CD34 (+), SMA (-), ALK1 (-), CD117 (-), Ki67 (-) | Exploratory laparotomy + 70 cm bowel resection + end-to-end primary anastomosis | Ileum | 6.3 x 2.9 cm |
| Khanduri et al. [ | 41 years | Male | Sudden abdominal pain, nausea, vomiting, and obstipation for 24 hours | Yes | Contrast-enhanced abdominopelvic CT: ileo-ileal intussusception | Not available | Exploratory laparoscopy + right hemicolectomy + ileocolic anastomosis + en bloc lymph node resection (14 nodes) | Ileum | 3 x 3 cm |
| Adams et al. [ | 61 years | Female | Diarrhea and hematochezia for 2 weeks, then right lower quadrant abdominal pain for 2 days | No | Contrast-enhanced abdominopelvic CT: ileo-ileal intussusception | CD117 (-), SMA (-), CD34 (-), DESMIN (-), S100 (-), DOG1 (-) | Exploratory laparoscopy + infraumbilical mini-laparotomy + 22 cm bowel resection + side-to-side stapled anastomosis | Ileum | 7.5 x 4.5 x 3.2 cm |
| Jacob et al. [ | 37 years | Female | Generalized cramping abdominal pain for 4 days, vomiting and diarrhea | No | Simple abdominopelvic CT: ileo-ileal intussusception | SMA (+), CD34 (-), CD117 (-), DOG1 (-), ALK (-), DESMIN & KERATIN (-) | Diagnostic laparoscopy converted to exploratory laparotomy + 30 cm bowel resection + side-to-side ileocolic stapled anastomosis | Ileum | 3 cm |
| Joyce et al. [ | 62 years | Male | Sudden cramping abdominal pain and abdominal distension for 12 hours | No | Simple abdominopelvic CT: jejuno-jejunal intussusception | CD117 (-), SMA (-), CD34 (-), VIM (+) | Exploratory laparotomy + 33 cm bowel resection + end-to-end anastomosis | Jejunum | 4.2 x 2.5 cm |
| Fabbri et al. [ | 62 years | Male | Cramping abdominal pain for 40 days | No | Contrast-enhanced abdominopelvic CT: intestinal intussusception | Not available | Exploratory laparotomy + 10 cm bowel resection + side-to-side primary anastomosis | Jejunum | 3.5 cm |
| Sakran et al. [ | 40 years | Male | Intermittent generalized abdominal pain and nausea | No | Oral contrast-enhanced abdominopelvic CT: intestinal intussusception | CD34 (+), VIM (+), S100 (-), DOG1 (-), ACTIN (-), DESMIN (-) | Exploratory laparoscopy + 10 cm bowel resection + side-to-side primary anastomosis + partial vertical gastrectomy with stapler | Ileum | Not specified |
| Paramythiotis et al. [ | 42 years | Female | Diffuse abdominal pain with vomiting and diarrhea for 7 days | No | Contrast-enhanced abdominopelvic CT: ileo-ileal intussusception | Not available | Exploratory laparotomy + right hemicolectomy | Ileum | Not specified |
| Xacur Trabulce et al. (Present study) | 69 years | Male | Intermittent cramping abdominal pain starting in lower quadrants and migrating to periumbilical area for 30 days | No | Oral/IV contrast-enhanced abdominopelvic CT: distal jejunal intussusception due to polypoid lesion | ACTIN (+), CD34 (+), CD117 (-), DOG1 (-), ALK (-), DESMIN (-), MDM-2 (-), proliferation index 1%. | Exploratory laparoscopy + 15 cm bowel resection + side-to-side enteroenteric anastomosis with linear stapler + laparoscopic cholecystectomy | Jejunum-Ileum | 3.4 x 4.1 cm |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Vascular Malformations and Hemangiomas · Gastrointestinal Tumor Research and Treatment
Introduction
Inflammatory fibroid polyps (IFPs) are uncommon, benign, non-epithelial tumors that mostly present as polypoid masses. They may develop anywhere in the gastrointestinal tract, but they are commonly found in the stomach (70%), specifically in the antrum, followed by the small bowel in the ileum [1-4]. These tumors arise in the submucosa and have an idiopathic nature [1,5]. The IFP was first described in 1949 by Czech pathologist Josef Vaněk (1915-1990) as a “submucosal gastric granuloma with eosinophilic infiltration” [5-9]. The exact pathogenesis of IFPs is unknown despite their specific histopathologic characteristics, described as a proliferation of spindle-shaped cells within a fibromyxoid stroma and prominent eosinophilic inflammatory infiltrate. A distinctive feature is a "whorled" or "onion-skin" appearance of stromal cells around blood vessels [2,5,10-12].
Vanek tumors contribute to less than 1% of all tumors of the gastrointestinal tract [1-4].
Most IFPs are incidentally detected during endoscopy, surgery, or imaging, because of their silent evolution. There are cases in which these tumors are located in the small bowel, and when they exceed 2-3 cm in size, they may cause obstructive symptoms. Intussusception is a rare condition in adults defined as the invagination of a proximal segment of the intestine into a distal segment. Intussusception accounts for only 1-5% of bowel obstructions, most commonly related to tumors, with benign lesions representing approximately 80% of all cases [6,13-15].
Preoperative contrast-enhanced CT imaging is essential, even though radiologic features of Vanek tumor are nonspecific, revealing only an intraluminal mass or intussusception, sometimes described as a sausage or sandwich sign and target or “bullseye” sign. The definitive diagnosis is based on histopathologic evaluation and immunohistochemistry, and for IFPs, the immunohistochemical markers are as follows: positive for CD34, negative for CD117 (c-kit), DOG1, S100, desmin, and alpha smooth muscle actin (SMA). This immunoprofile is helpful in differentiating IFPs from other neoplasms in the gastrointestinal tract, including gastrointestinal stromal tumors (GISTs), leiomyoma, and neural tumors [9,16,17].
The treatment of choice is surgical excision in symptomatic patients or when complications such as intussusception or obstruction occur. Both open and minimally invasive surgery, even in complex cases, have been described with no recurrence or malignant transformation after the resection because of the benign nature of these neoplasms [2,18,19].
Our case illustrates the typical presentation of a small intestine intussusception causing obstructive symptoms secondary to IFPs, requiring emergency surgical intervention.
A comprehensive literature review was conducted using PubMed and ScienceDirect, identifying only 20 published articles reporting IFPs of the small intestine as a cause of intussusception in adult patients, with the earliest case published in 2011.
Case presentation
A 69-year-old male was referred to the emergency department due to abdominal pain. During anamnesis, he reports acute colicky pain in the lower abdominal quadrants that migrates to the periumbilical region, intensity described with a punctuation on the pain scale of 4 out of 10. He denies any presence of nausea, vomiting, weight loss, fever, or diaphoresis. In the clinical examination, we find a globular abdomen due to panniculus, hypoactive peristalsis, tympanic percussion of the colic frame, and pain on the palpation of the mesogastrium, without signs of peritoneal irritation. A computed tomography of the abdomen and pelvis with IV contrast revealed a polypoid lesion located in the distal jejunum, which caused a small bowel intussusception, cholelithiasis, and uncomplicated diverticular disease (Figure 1).
Computed tomography of the abdomen and pelvis with IV contrastA polypoid lesion of the distal jejunum that causes small bowel intussusception, considered the first possibility of a gastrointestinal stromal tumor.A) Red circle - sausage or sandwich sign. B) Red circle - target or “bullseye” sign.
On account of the imaging and clinical features of the patient, an exploratory laparoscopy was performed. The following intraoperative findings were identified: intestinal intussusception located 250 cm distal to the Treitz angle, and within the intestinal lumen, a tumor measuring approximately 3.4 x 4.1 cm was found, without evidence of free fluid or intestinal perforation in the abdominal cavity (Figure 2). Because of the impossibility of intracorporeal reduction, it was necessary to expand the umbilical incision by 4 more centimeters to facilitate the exteriorization of the involved loop. A 14.5-cm small bowel resection was performed. Subsequently, a side-to-side entero-enteric anastomosis using a linear stapler was executed (Figure 3). The anastomosis was reduced back to the abdominal cavity, followed by a complementary laparoscopic cholecystectomy.
Intraoperative pathological examination findingsIntestinal intussusception located 250 cm from the Treitz angle, with a 4.1 × 3.4 cm tumor exhibiting extensive ulceration on the superficial portion. Marked edema and vascular congestion are present, along with areas of recent microhemorrhage in the intestinal wall.
Side-to-side entero-enteric anastomosis using a linear staplerThe staple line is clearly visualized, demonstrating precise alignment and a tension-free configuration between the adjacent small bowel loops.
The intestinal resection segment and gallbladder specimens were sent to pathology, and the histopathological analysis identified a polypoid tumor with morphological and immunophenotypic findings consistent with an inflammatory fibroid polyp (Vanek tumor) characterized by proliferative stromal cells (Figure 4). The 4.1 x 3.4 cm lesion exhibited extensive superficial ulceration, concomitant with marked edema, vascular congestion, and focal areas of recent microhemorrhage within the intestinal wall. A few days after the surgery, the immunohistochemical staining revealed the tumor to be positive for smooth muscle actin and CD34, and while negative for CD117, DOG-1, ALK, desmin, and MDM-2, the Ki-67 proliferation index was 1% (Figure 5). The postoperative recovery was uneventful, resulting in discharge after 72 hours.
HistopathologyFibromyxoid tissue with inflammatory infiltration, spindle-shaped or stellate cells, and inflammatory cells, typically eosinophils. Thin-walled blood vessels are arranged in an "onion-skin" pattern. The lesion was diagnosed as an inflammatory fibroid polyp. A staining method was used for histopathological evaluation, although the specific technique was not disclosed.
ImmunohistochemistrySmooth muscle actin (SMA) positive, CD34 positive, CD117 negative, DOG-1 negative, ALK negative, desmin negative, and MDM-2 negative. Proliferation index: 1%. Ki-67 staining was performed with a result of <1%; however, it is not shown.
Discussion
A search of the english literature was performed by the authors (AX, BL, GC y SA) on the open-access databases PubMed and ScienceDirect, using the following algorithm ((vanek tumor) AND (inflammatory fibroid polyp)) AND (small bowel intussusception) applying more specific filters to include papers published between the years 2011-2023, incorporating review articles, research articles and case reports, in the English language. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 (PRISMA) guidelines were followed, and the search included the keywords “Vanek tumor” and “inflammatory fibroid polyp”. Only cases involving small intestine localization with intestinal intussusception in adult patients were considered. The initial search included 40 articles, and 38 remained after removing duplicates. After that, 20 papers were excluded due to lack of full-text availability, irrelevance to the systematic review, or absence of the studied pathology. A total of 20 reports meeting the selection criteria were identified, covering the period from 2011 to 2023 (Figure 6).
PRISMA flow diagramArticle selection process using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)
After full text analysis, information extraction was directed to the identification of age, sex, clinical presentation, the presence or absence of palpable mass, radiological tools, immunohistochemistry, surgical approach, location, and size of Vanek tumors (Table 1). Notably, while Figure 1 accounts for 20 studies, Table 1 comprises 22 cases. This discrepancy arises from the inclusion of two cases reported by Carvalho et al. [5] and the addition of our own case as the 22nd.
An analysis of 22 clinical cases was performed, and it is clear that the typical presentation of IFPs predominates in adults during the fourth to fifth decade of life (Figure 7), with a higher incidence in females (Figure 8) [1-20]. Vanek tumors are most commonly located in the stomach, followed by the small intestine, and rarely in the colon (Figure 9) [10,14]. Most times, these neoplasms are asymptomatic, and their discovery is often incidental during endoscopy or abdominal surgery. Although some patients present to the emergency department with a clinical presentation of bowel obstruction, with colicky abdominal pain representing the cardinal symptom - with variable intensity proportional to the degree of obstruction and presence of bowel ischemia [2,3,5,6]. Patients can also experience constipation, abdominal distension, nausea, vomiting, and, less frequently, diarrhea, weight loss, or gastrointestinal bleeding [1-3,5,7,8]. Tumor size presentation among the 22 cases ranged between 1.9 and 18 cm; most tumors measured between 3 and 5 cm, as illustrated in the box plot (Figure 10). Tumor size was not specified in two cases. The plot excludes one extreme outlier (18 cm) for visual clarity. This finding supports that IFPs can vary in size, although they often remain asymptomatic until they cause mechanical complications [2,6,10].
Histogram - age distribution of the reported casesMost patients were in their fourth to fifth decade of life, predominantly between 40 and 45 years.Sources: Refs [1-20]
Pie chart - sex distribution of the reported cases 63.6% of the total cases occurred in females.Sources: Refs [1-20]
Bar chart - tumor location in the reported casesThe ileum was significantly the most frequent location.Sources: Refs [10,14]
Box plot - distribution of tumor size (cm)The tumor size ranged from 1.9 to 18 cm, with most lesions measuring between 3 and 5 cm. The mean tumor diameter was approximately 4.0 cm. Tumor size was not reported in two of the 22 cases.
Literature implies that approximately 50% of cases may present with a palpable abdominal mass on physical examination [10]; however, only two patients in the review exhibited this clinical finding. Due to the presence of intestinal ischemia, ulceration, or perforation, additional signs will develop, such as mucocutaneous pallor, tenderness, guarding, rebound tenderness or tachycardia, progressing to hemodynamic instability, septic shock, and even death [9,12,13].
As part of the diagnostic algorithm, abdominal radiography is useful to identify the presence of bowel obstruction and free abdominal air, suggesting that perforation with the “seagull sign” can be recognized in a thorax radiography. In the abdominal ultrasound, some specific findings of intussusception might be present, just like the classic “target” or “bullseye” sign, with a reported sensitivity of 98-100% and specificity of 88-89% [10,14,20]. Notwithstanding, contrast-enhanced abdominal computed tomography remains the preferred imaging modality for adult intussusception. Typical findings in the CT scan include the “target” or “bullseye” sign, “sausage”- or “sandwich”-shaped masses, and signs of complications such as bowel obstruction, free fluid, pneumoperitoneum, intestinal pneumatosis, or mural thickening >35 mm [5,7,13]. Our case, along with those reported by Carvalho et al. [5] and Forasté-Enríquez et al. [6], provides an example of a small bowel intussusception that required surgical intervention.
Definitive diagnosis relies on histopathological examination and immunohistochemistry. Microscopic findings include fibromyxoid tissue infiltrated by eosinophils, spindle or stellate mesenchymal cells, thin-walled blood vessels in concentric (“onion-skin”) arrangements, and sometimes multinucleated giant cells [1,4,11,16]. Most IFPs express CD34 and lack markers such as CD117 (c-KIT) and S100, assisting in their differentiation from GISTs, leiomyomas, and neural tumors [8,10,14].
Complete excision by open or minimally invasive surgery remains the standard treatment for symptomatic Vanek tumors, and although when the lesions are small and accessible, endoscopic removal can be considered. Choosing the appropriate approach depends on tumor location, evidence of perforation or ischemia, and the degree of suspicion for malignancy [9,15,17]. Once the tumor is fully removed, recurrence is virtually nonexistent, and there is no need for further treatment [10,18,19].
Conclusions
Vanek tumors located in the small intestine are uncommon, benign lesions that are generally asymptomatic but can occasionally cause intussusception, leading to bowel obstruction in adults. While they are more frequently found in the stomach, when the small bowel is involved, it can lead to various forms of invagination, including complicated or recurrent forms. This case highlights an uncommon presentation of an IFP causing ileo-ileal intussusception in an adult patient, emphasizing the importance of maintaining a high index of suspicion for rare benign causes of bowel obstruction. Although preoperative imaging, especially computed tomography, is crucial for suggesting intussusception, definitive diagnosis of IFP is made histopathologically. The cornerstone for treatment is surgical resection, which has been reported laparoscopically in several studies. Despite their benignity, the increasing number of reported cases further sharpens our understanding of their clinical behavior and management strategies. This requires ongoing documentation and study of these tumors to further enhance early recognition and optimize outcomes of affected patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Inflammatory fibroid polyp (Vanek's tumor) causing double compound ileo-ileal intussusception in an adult patient, a case report Int J Surg Case Rep Gadoura A Mohammed F Abdulkarim M Ibn Yasir A Shani D Salih N 106947932022 https://doi.org/10.1016/j.ijscr.2022.1069473531818310.1016/j.ijscr.2022.106947 PMC 8935495 · doi ↗ · pubmed ↗
- 2Intussusception in an adult revealing a Vanek's tumor: a case report Int J Surg Case Rep Chaima Y Amine S Ahmed BM Amine D Anis H Montasser Jameleddine K 1082651062023 https://doi.org/10.1016/j.ijscr.2023.1082653712089510.1016/j.ijscr.2023.108265 PMC 10173153 · doi ↗ · pubmed ↗
- 3Small bowel intussusception due to inflammatory fibroid polyp: a case report Radiol Case Rep Al Taei TH Al Mail SA 8018041320182998892910.1016/j.radcr.2018.05.008PMC 6034136 · doi ↗ · pubmed ↗
- 4Laparoscopic resection of two inflammatory fibroid polyps: an unusual cause of jejunojejunal intussusception Int J Surg Case Rep Park KB Jee YS Kim DW 2023692020 https://doi.org/10.1016/j.ijscr.2020.03.0293224801110.1016/j.ijscr.2020.03.029PMC 7132045 · doi ↗ · pubmed ↗
- 5Small bowel intussusception in 2 adults caused by inflammatory polyps Radiol Case Rep Carvalho A Leitão P Pinheiro J Sá Fernandes M Rodrigues M Preto AS Silva N 7107141220172948405510.1016/j.radcr.2017.08.010PMC 5823309 · doi ↗ · pubmed ↗
- 6[Intestinal obstruction in adults due to ileal intussusception secondary to inflammatory fibroid polyp: a case report]Rev Gastroenterol Mex Forasté-Enríquez CF Mata-Hernández R Hernández-Villaseñor A Alderete-Vázquez G Grube-Pagola P 2632658220172771762810.1016/j.rgmx.2016.03.006 · doi ↗ · pubmed ↗
- 7Vanek's tumor as an unusual cause of ileo-ileal intessuception - a unique case report Ann Med Surg Jan ZU Muslim M Ullah K Shoaib A Ahmed N Khan ZM Aurangzeb M 141732201810.1016/j.amsu.2018.06.006PMC 603989530002823 · doi ↗ · pubmed ↗
- 8Rare case of small bowel intussusception secondary to an inflammatory fibroid polyp (Vanek's tumour)ANZ J Surg Jacob S Lee T Yuen L 04912021 https://doi.org/10.1111/ans.1670910.1111/ans.1670933634595 · doi ↗ · pubmed ↗