Adult-Onset Alexander Disease: A Case Report and Literature Review of Glu207 Alterations
Sai Krishna Vallamchetla, Omar Abdelkader, Ibrahim S Tuna, Gayane Barsamyan, Hans Shuhaiber

TL;DR
A 67-year-old woman with adult-onset Alexander disease had a rare GFAP gene mutation, showing how genetic testing and imaging can help diagnose this rare neurological disorder.
Contribution
This case expands the known genetic variants of adult-onset Alexander disease and highlights the importance of GFAP testing in adults with unexplained neurological symptoms.
Findings
A heterozygous GFAP c.620A>T (p.Glu207Val) variant was identified in a patient with adult-onset Alexander disease.
Characteristic MRI findings included spinal cord atrophy and periventricular FLAIR hyperintensity.
The mutation was present in a symptomatic sibling and maternal relatives, supporting autosomal dominant inheritance with variable expressivity.
Abstract
Alexander disease (AxD) is a rare leukodystrophy caused by heterozygous mutations in GFAP. We report the case of a 67-year-old woman with progressive dysarthria, dysphagia, ataxia, and oculomotor dysfunction. MRI revealed medullary and cervical spinal cord atrophy with a periventricular T2/fluid-attenuated inversion recovery (FLAIR) hyperintense rim, findings characteristic of adult-onset AxD. Genetic testing identified a heterozygous GFAP c.620A>T (p.Glu207Val) variant, absent from major population databases. Her symptomatic brother carried the same mutation, and additional maternal relatives exhibited suggestive neurological features, supporting autosomal dominant inheritance with variable expressivity. In silico tools predicted the variant to be pathogenic, and multiple mutations at the same residue have been associated with AxD. This case expands the genotypic spectrum of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
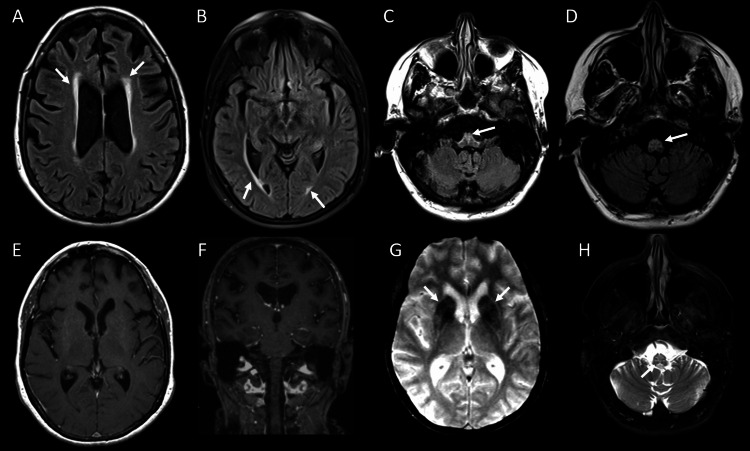 Figure 1
Figure 1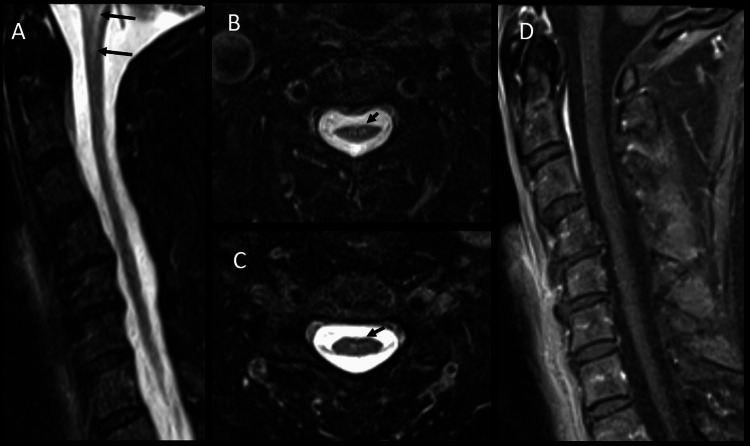 Figure 2
Figure 2| Case Reports/Studies | Type | Mutation | Exon/Intron | Protein change | Age at onset |
| van der Knaap et al., 2005 [ | missense | c.619G>A | Exon 4 | p.Glu207Lys | 10 years |
| van der Knaap et al., 2005 [ | missense | c.619G>C | Exon 4 | p.Glu207Gln | 10 years |
| Flint et al., 2012 [ | splice-site | c.619-3C>G | Intron 3 | p.Glu207_Lys260del | 76 years |
| Gass et al., 2017 [ | missense | c.620A > T | Exon 4 | p.Glu207Val | 52 years |
| Amano et al., 2021 [ | splice-site | c.619-1G>A | Intron 3 | p.Glu207del | 76 years |
| Current report | missense | c.620A > T | Exon 4 | p.Glu207Val | 65 years |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRNA regulation and disease · RNA and protein synthesis mechanisms · interferon and immune responses
Introduction
Alexander disease (AxD) is a rare, fatal neurodegenerative leukodystrophy caused by heterozygous gain-of-function mutations in the GFAP gene (chromosome 17q21) encoding glial fibrillary acidic protein (GFAP), an astrocyte-specific type III intermediate filament [1]. It is characterized pathologically by the abnormal accumulation of Rosenthal fibers in astrocytes, which are ubiquitinated protein aggregates composed of GFAP, heat shock protein 27 (HSP27), and alpha B-crystallin [2]. Due to variability in phenotypic expression and its strong correlation with age of onset, AxD was grouped into two major subtypes. Type I (early onset, often < 4 years) is characterized by macrocephaly, seizures, developmental delay, and failure to thrive. In contrast, Type II (older children and adults) is characterized by a slowly progressive course with bulbar, cerebellar, and oculomotor signs with autonomic dysfunction. These subtypes exhibit distinct neuroimaging patterns. Infantile forms typically show extensive frontal white matter abnormalities, basal ganglia involvement, and a periventricular rim, whereas the adult form often presents with mild-to-moderate cerebral involvement, atrophy of the medulla and cervical spinal cord, and signal abnormalities in the anterior portion of the medulla oblongata [3].
Diagnosis of AxD is suspected based on clinical presentation with supportive neuroimaging findings and is confirmed by identifying pathogenic GFAP mutations on genetic testing [4]. At least 182 distinct* GFAP *mutations had been identified in individuals with AxD, with the majority (97.4%) being missense mutations [1]. However, the phenotypic spectrum and underlying genetic landscape of leukodystrophies remain complex, with many mutations yet to be fully characterized [5]. Identifying novel mutations is crucial for improving diagnostic accuracy, understanding genotype-phenotype correlations, and guiding genetic counseling.
Here, we describe the case of a 67-year-old woman who presented with progressive bulbar dysfunction, spastic-ataxic gait, oculomotor abnormalities, and a suggestive family history, and was found to have a rare heterozygous missense mutation in the GFAP gene, specifically the c.620A>T (p.Glu207Val) variant. This case contributes to the evolving genotypic spectrum of adult-onset AxD and highlights the importance of considering GFAP testing in adults with unexplained bulbar-pyramidal syndromes.
Case presentation
A 67-year-old woman presented to our clinic with a two-year history of progressive dysarthria, dysphagia, worsening balance, and gait instability. She also reported intermittent episodes of dizziness, chronic constipation, and difficulty maintaining direct and conjugate gaze. Her medical history was notable for a cerebrovascular accident 24 years earlier, which resulted in bilateral peripheral visual field deficits and mild memory impairment. She had undergone total knee arthroplasty for severe osteoarthritis and was taking hydrochlorothiazide, atorvastatin, and omeprazole for hypertension, hypercholesterolemia, and gastroesophageal reflux disease, respectively.
Neurologic examination revealed generalized hyperreflexia and spasticity, predominantly in the lower limbs, along with cerebellar dysfunction evidenced by a positive Romberg sign, an ataxic, wide-based gait with impaired tandem walking, and bilateral finger-to-nose dysmetria. Oculomotor assessment revealed impaired smooth pursuit and saccades, with horizontal gaze worsening diplopia. Oral examination demonstrated rhythmic palatal myoclonus.
Routine laboratory investigations were unremarkable. However, contrast-enhanced MRI of the brain demonstrated a periventricular rim of fluid-attenuated inversion recovery (FLAIR) hyperintensity in the brain (Figure 1).
Contrast-enhanced MRI of the brainBrain MRI demonstrates mild to moderate generalized brain volume loss with ex-vacuo prominence of the ventricles and cerebral sulci. On the T2-FLAIR sequence, there is mild diffuse periventricular rim FLAIR hyperintensity (arrows on A and B) without deep white matter involvement. At the level of the medulla and upper cervical spine, there is moderate atrophy and increased T2/FLAIR signal (arrows on C, D, and H) without a mass configuration. Postcontrast imaging (E and F) demonstrates no abnormal enhancement in the basal ganglia, white matter, or brainstem. T2GRE (G) demonstrates hypointensity, suggesting prominent mineralization in the basal ganglia, particularly in the caudate nucleus and putamen (arrows on G) without atrophy.FLAIR: fluid-attenuated inversion recovery; GRE: gradient recalled echo*
Additionally, cervical spine MRI showed an abnormal signal and diffuse atrophy involving the cervicomedullary junction and upper cervical spinal cord, characterized by T2/FLAIR hyperintensity in the medulla and central upper cervical cord, along with medullary atrophy (Figure 2).
Cervical spine MRISagittal T2-STIR (A) and axial T2-STIR at the level of C3 (B) and C5 (C) demonstrate abnormal T2 signal involving the medulla and upper cervical spinal cord at the level of C1 (black arrows on A) and central cord (black arrows on B and C) with mild diffuse cord atrophy. There is no abnormal enhancement within the cord on post-contrast sag T1 fat-saturated imaging (D).STIR: short tau inversion recovery
These clinical and neuroimaging findings, along with a family history of AxD in her 59-year-old brother, prompted expanded genetic testing.
Invitae leukodystrophy panel identified a heterozygous variant in GFAP, c.620A>T (p.Glu207Val), located in exon 4. Her brother’s genetic report showed an identical mutation. Additional family history revealed significant neurological issues. While her parents and eight other siblings remained asymptomatic, two sisters (aged 68 and 63 years) exhibited suggestive features such as vocal cord tremors, unsteady gait, and autonomic dysregulation, though without genetic confirmation. Two maternal cousins had genetically confirmed AxD, strongly implicating maternal carriage.
Considering her symptoms, she was initiated on baclofen, tizanidine, and cyclobenzaprine for spasticity and gabapentin for neuropathic discomfort. At the six-month follow-up, she reported modest improvements in tremor control, neuropathic pain, and ambulation, and she continues genetic counseling.
Discussion
AxD is a rare neurodegenerative disorder characterized by mutations in the GFAP gene [1]. Its clinical presentation and genetic diversity, particularly in adult-onset forms, remain an active research area [5]. This case report expands the known genetic spectrum of adult-onset AxD by highlighting a heterozygous missense mutation in GFAP. While the identified GFAP c.620A>T (p.Glu207Val) variant is absent in major public databases such as ClinVar and gnomAD [6,7], an identical mutation at p.Glu207Val was previously reported in a 52-year-old male with adult-onset AxD [8]. In silico analyses (PolyPhen-2 and MutationTaster) predict this variant to be damaging and disease-causing [9,10]. The glutamate residue at position 207 appears to play a critical role in GFAP function, as alterations at this site have been implicated in disease causation. Multiple missense mutations, including p.Glu207Val (adult onset) [8], p.Glu207Gln (juvenile onset) [11,12], p.Glu207Lys (juvenile onset) [11,12], and splice-site mutations like p.Glu207del (adult onset) [13] and p.Glu207_Lys260del (adult onset) [14] have been associated with AxD (Table 1).
Unlike the infantile form characterized by rapid neurodevelopmental decline, seizures, and extensive cerebral white matter involvement, adult-onset AxD typically presents in the second to seventh decades with prominent bulbar dysfunction, spasticity, and ataxia, often progressing slowly over the years. Because these features overlap with other adult neurological syndromes, AxD is frequently unrecognized or misdiagnosed without genetic testing or characteristic neuroimaging findings [4,15]. Our patient’s presentation with progressive dysarthria, dysphagia, spastic‐ataxic gait, palatal myoclonus, and oculomotor impairment fits the classic bulbar‐predominant phenotype of AxD. Brain and cervical-spine MRI confirmed the disproportionate medullary and upper cervical cord atrophy with associated T2 signal changes, along with a fine rim of frontal periventricular T2/FLAIR hyperintensity. When coupled with her *GFAP *mutation, this clinicoradiologic fingerprint not only supports the diagnosis and distinguishes AxD from its mimics but also underscores the need for GFAP sequencing in adults presenting with unexplained bulbar signs and progressive spasticity.
Although no disease-modifying therapies exist at this point, symptomatic management of spasticity, neuropathic discomfort, and bulbar dysfunction can improve quality of life, and genetic counseling offers at-risk relatives the opportunity for surveillance and early intervention [4]. Emerging approaches that target GFAP expression or aggregation hold promise for future treatment [16].
Conclusions
The variant's absence in population databases, its prior association with AxD, its predicted deleterious impact, and its familial occurrence alongside a consistent clinical and radiological phenotype strongly suggest its pathogenicity. This case not only emphasizes the pathogenicity of this variant but also supports the autosomal dominant inheritance pattern of the disease. It also highlights the lack of strong genotype-phenotype correlation with variable expressivity, even with the same mutation in the index patient’s family. This phenotypic variability may be due to additional factors affecting disease expression.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A systematic review and meta-analysis of GFAP gene variants in Alexander disease Sci Rep Grossi A Rosamilia F Carestiato S Salsano E Ceccherini I Bachetti T 243411420243942004610.1038/s 41598-024-75383-4PMC 11487261 · doi ↗ · pubmed ↗
- 2The Alexander disease-causing glial fibrillary acidic protein mutant, R 416W, accumulates into Rosenthal fibers by a pathway that involves filament aggregation and the association of alpha B-crystallin and HSP 27Am J Hum Genet Der Perng M Su M Wen SF 1972137920061682651210.1086/504411 PMC 1559481 · doi ↗ · pubmed ↗
- 3GFAP mutations, age at onset, and clinical subtypes in Alexander disease Neurology Prust M Wang J Morizono H 128712947720112191777510.1212/WNL.0b 013e 3182309 f 72PMC 3179649 · doi ↗ · pubmed ↗
- 4Alexander disease Gene Reviews® [Internet] Srivastava S Waldman A Naidu S Seattle (WA)University of Washington, Seattle 2020 https://www.ncbi.nlm.nih.gov/books/NBK 1172/20301351 · pubmed ↗
- 5Clinical, genetic, and molecular characteristics in a central-southern Chinese cohort of genetic leukodystrophies Ann Clin Transl Neurol Li Y Xu J Xu Y Li C Wu Y Liu Z 155615681020233743439010.1002/acn 3.51845 PMC 10502626 · doi ↗ · pubmed ↗
- 6Clin Var: public archive of relationships among sequence variation and human phenotype Nucleic Acids Res Landrum MJ Lee JM Riley GR Jang W Rubinstein WS Church DM Maglott DR 0542201410.1093/nar/gkt 1113 PMC 396503224234437 · doi ↗ · pubmed ↗
- 7A genomic mutational constraint map using variation in 76,156 human genomes Nature Chen S Francioli LC Goodrich JK 9210062520243805766410.1038/s 41586-023-06045-0PMC 11629659 · doi ↗ · pubmed ↗
- 8Novel GFAP variant in adult-onset Alexander disease with progressive ataxia and palatal tremor Neurologist Gass JM Cheema A Jackson J Blackburn PR Van Gerpen J Atwal PS 2472482220172909532910.1097/NRL.0000000000000153 · doi ↗ · pubmed ↗