Photo Quiz: Asteroid bodies in a skin biopsy of a farmer
Xiujiao Xia

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
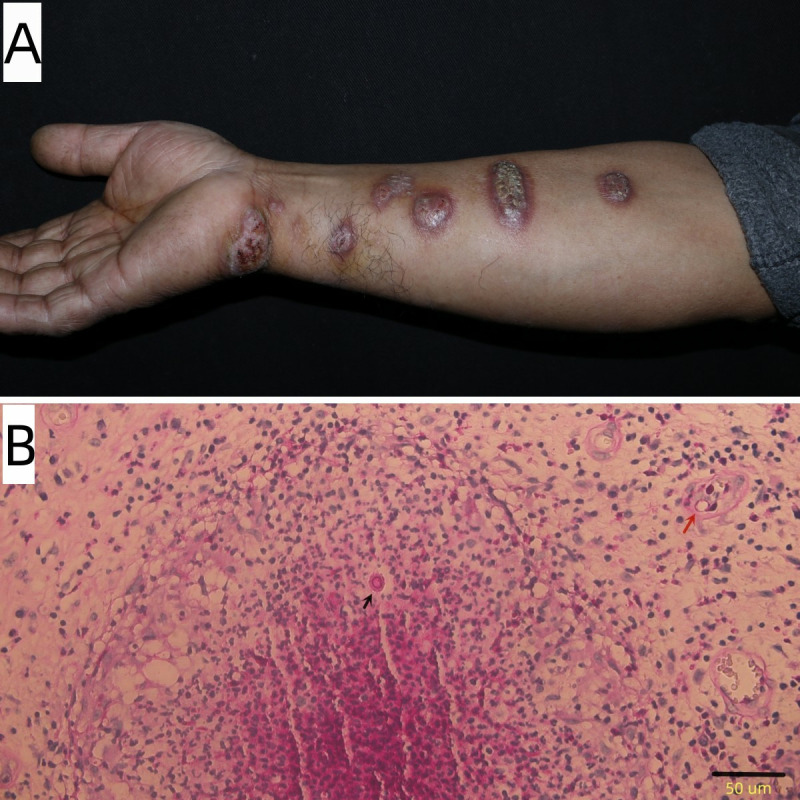 Fig 1
Fig 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Infectious Diseases and Mycology · Dermatological diseases and infestations
PHOTO QUIZ
A 56-year-old otherwise healthy male farmer presented to our dermatology clinic with a 3-month history of progressively increasing nodules on the right upper extremity. The patient indicated that nodular lesions developed approximately 2 weeks after a traumatic wrist injury during farming activities. Physical examination revealed several dull-red, crusted nodules distributed in a sporotrichoid and beaded pattern along the right upper extremity (Fig. 1). A biopsy of the lesions was performed for histopathological evaluation and fungal culture. Hematoxylin and eosin staining revealed diffuse inflammatory cell infiltration in the dermis, with multiple epithelioid cell granulomas containing central neutrophilic microabscesses. Periodic acid-Schiff (PAS) staining showed that yeast cells were present within the dermis; some yeast cells were encapsulated by a prominent layer of reddish material, with numerous neutrophils diffusely distributed in the surrounding area (Fig. 1B).
Linear distribution of nodules on the right upper extremity (A). Black arrow shows a round asteroid body, and red arrow shows a round yeast cell (B, PAS × 400).
What is your diagnosis?
ANSWER TO PHOTO QUIZ
The patient was diagnosed with lymphocutaneous sporotrichosis. Sporotrichosis is a subcutaneous mycosis caused by dimorphic fungi of the genus Sporothrix (order Ophiostomatales). Among the pathogenic species, Sporothrix brasiliensis, which is primarily transmitted through animal contact, exhibits high virulence and is predominantly endemic to South America, particularly Brazil. In contrast, Sporothrix globosa and Sporothrix schenckii follow classical saprophytic transmission pathways and demonstrate relatively lower virulence. S. globosa is primarily distributed across Asia, while S. schenckii has a global distribution (1). Definitive diagnosis of sporotrichosis requires culturing and subsequent characterization of Sporothrix species from patient-derived specimens. Fungal cultures were conducted in our mycology laboratory. Fungal cultures yielded colonies of S. globosa, which were confirmed by DNA sequencing (GenBank accession number PV203249). Based on these findings, a diagnosis of lymphocutaneous sporotrichosis was established. The lesions resolved completely following a 6-month course of systemic 10% potassium iodide (oral, 10 mL three times daily).
Histopathological examination of human samples may lack specificity and can only provide suggestive information for the diagnosis of sporotrichosis. Its histopathological features on skin biopsy are usually associated with granulomatous and pyogenic reactions and may be accompanied by epidermal hyperplasia (with or without ulceration), papillary spinous layer hypertrophy, hyperkeratosis, intraepidermal microabscesses, and the presence of fungal elements such as yeast cells and asteroid bodies (ABs) (2). ABs are histopathological structures characterized by a central eosinophilic core surrounded by radiating, homogeneous, refractile, eosinophilic, club-shaped projections. These structures represent a Splendore-Hoeppli reaction, which is a localized immunological host response to antigens from various infectious organisms, including fungi, bacteria, and parasites (3). In sporotrichosis, ABs are formed by the yeast cells and the surrounding antigen-antibody precipitation complex. According to the outline of the eosinophilic materials, the AB can be classified into five categories: stellate, club-shaped, ring-shaped, flower-shaped, and irregular (2).
AB is not a sporotrichosis pathognomonic structure, as it can occur in other infectious or granulomatous diseases (4), but in the case of central presence of yeast cells, combined with the clinical manifestations and medical history, it is a useful clue in the diagnosis of sporotrichosis (5). The sensitivity of histopathological tests for diagnosing cutaneous sporotrichosis remains limited due to the scarcity of fungal elements in the tissue samples (4). Fungal structures in tissues are observed in 18.00%–35.30% of cases, depending on the group of patients studied and the methodology employed (6). Sporothrix yeast cells exhibit a variety of morphologies, including round, oval, and cigar-shaped forms (7). The central spherical fungal structure within AB serves to decrease the volume-to-external surface ratio, thereby effectively minimizing the contact area (8). Itraconazole is widely regarded as the first-line treatment for sporotrichosis, owing to its well-documented efficacy, favorable safety profile, and convenient dosing regimen (9). Potassium iodide has been traditionally used in the treatment of sporotrichosis since the early 20th century. Nowadays, it is still used to treat cutaneous sporotrichosis due to its low cost (7).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rodrigues AM, Hagen F, de Camargo ZP. 2022. A spotlight on sporothrix and sporotrichosis. Mycopathologia 187:407–411. doi:10.1007/s 11046-022-00642-935776287 · doi ↗ · pubmed ↗
- 2Zhang Y-Q, Xu X-G, Zhang M, Jiang P, Zhou X-Y, Li Z-Z, Zhang M-F. 2011. Sporotrichosis: clinical and histopathological manifestations. Am J Dermatopathol 33:296–302. doi:10.1097/DAD.0b 013e 3181 f 5b 62221512340 · doi ↗ · pubmed ↗
- 3Barros M de L, de Almeida Paes R, Schubach AO. 2011. Sporothrix schenckii and sporotrichosis. Clin Microbiol Rev 24:633–654. doi:10.1128/CMR.00007-1121976602 PMC 3194828 · doi ↗ · pubmed ↗
- 4Morris-Jones R. 2002. Sporotrichosis. Clin Exp Dermatol 27:427–431. doi:10.1046/j.1365-2230.2002.01087.x 12372075 · doi ↗ · pubmed ↗
- 5Rodríguez G, Sarmiento L. 1998. The asteroid bodies of sporotrichosis. Am J Dermatopathol 20:246–249. doi:10.1097/00000372-199806000-000049650696 · doi ↗ · pubmed ↗
- 6Pereira MA, Freitas RJ, Nascimento SB, Pantaleão L, Vilar EG. 2020. Sporotrichosis: a clinicopathologic study of 89 consecutive cases, literature review, and new insights about their differential diagnosis. Am J Dermatopathol 42:751–755. doi:10.1097/DAD.000000000000161732149828 · doi ↗ · pubmed ↗
- 7Rodrigues AM, Gonçalves SS, de Carvalho JA, Borba-Santos LP, Rozental S, Camargo ZP de. 2022. Current progress on epidemiology, diagnosis, and treatment of sporotrichosis and their future trends. J Fungi (Basel) 8:776. doi:10.3390/jof 808077635893145 PMC 9331723 · doi ↗ · pubmed ↗
- 8Daniel Da Rosa W, Gezuele E, Calegari L, Goñi F. 2008. Asteroid body in sporotrichosis. Yeast viability and biological significance within the host immune response. Med Mycol 46:443–448. doi:10.1080/1369378080191489818608903 · doi ↗ · pubmed ↗