Non-fungal pathogens detected by broad-range fungal polymerase chain reaction
Sonya Ahuja, Joshua A. Lieberman

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
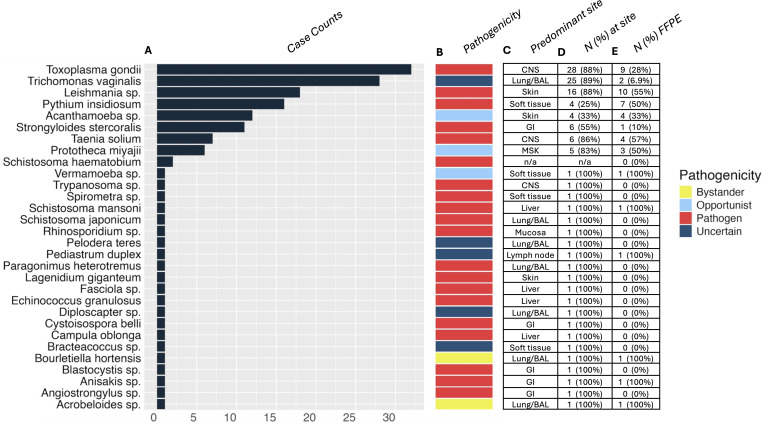 Fig 1
Fig 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPlant Pathogens and Fungal Diseases · Antifungal resistance and susceptibility · Fungal Infections and Studies
LETTER
Few laboratory tests target non-fungal eukaryotic pathogens, such as oomycetes, amoebae, and other parasites. At our molecular reference laboratory, we observed rare detections (<1%) of non-fungal eukaryotic pathogens by broad-range fungal PCR and Sanger sequencing (1–3) due to conserved primer binding sequences in the large ribosomal subunit gene (Fig. S1) (4). These were reported clinically but described as “incidental findings” whose presence could preclude the detection of fungal DNA (see Supplemental materials). To assess the diversity and taxonomic specificity of organisms detected by this method, we searched the laboratory information system for the term “incidental” within broad-range fungal PCR reports from January 2001 to August 2023. For organisms identified by this strategy, we searched fungal PCR reports for instances where “incidental” was omitted. Metadata and laboratory results were analyzed using R version 2023.06.2+561.
We identified 153 cases from 138 patients, with a median age of 49.6 years. Of the patients, 50 were female, 86 were male, and 2 were unspecified. Thirty unique non-fungal organisms distributed across 10 taxonomic orders were reported (Fig. S2). Of eight identified in multiple patients, seven were bona fide pathogens (Fig. 1). The three most common were Toxoplasma gondii (N = 32), Trichomonas vaginalis (N = 28), and Leishmania sp. (N = 18) (Fig. 1). T. gondii was primarily identified in central nervous system (CNS) samples (28/32), and Leishmania sp. was primarily in skin (16/18). Interestingly, T. vaginalis was primarily identified in BAL/lung specimens (25/28). Most organisms were detected in viscera (N = 68), with BAL/lung (N = 37) as the most frequently involved site. The 28S primer set was more frequently positive (114/167) than ITS (66/167), likely reflecting increased sequence diversity in ITS loci (Fig. S1) (4). Both primer sets were positive in 37 cases.
Characteristics of incidentally identified non-fungal eukaryotes. Case counts of non-fungal organisms detected are displayed as horizontal bars (A). Note that Campula oblonga was detected from a dolphin necropsy performed for research testing rather than from a human case. Organism pathogenicity is indicated by colored bars (B). The anatomic site where the incidental organism was most often detected is indicated (GI, gastrointestinal; BAL, bronchoalveolar lavage; and n/a, not applicable) (C), with the proportion of cases at the predominant site provided as the number and percentage of cases (D). The number and percentage of cases for each organism detected in formalin-fixed paraffin-embedded tissue were calculated using all samples tested rather than unique patients (E).
We identified a wide range of non-fungal incidental findings, from the common helminth Strongyloides stercoralis (N = 14) to uncommon pathogens like Pythium insidiosum (N = 20). Five organisms were of uncertain clinical significance, each identified in one case (Fig. 1). While some may have been contaminants, others, like Bracteacoccus—a green alga identified in subcutaneous tissue from a patient’s thumb—could represent true infections. Our observations suggest broad-range fungal assays may aid in the detection and identification of non-fungal eukaryotic pathogens when other diagnostic options are limited, including when present in formalin-fixed paraffin-embedded tissue (Fig. 1).
This study has several limitations. First, the assay was validated for fungi; thus, performance data for other organisms are lacking. Second, concurrent histologic/laboratory results were frequently unavailable, limiting clinicopathologic correlation and precluding an estimate of false negativity (see Supplemental materials). Third, the assay was frequently limited to genus rank identification due to inherent limitations in the targeted rRNA loci or lack of high-quality sequences in public databases (5). Consequently, less common parasites, such as Spirometra and Angiostrongylus, were reported at genus rank, whereas more common parasites like Strongyloides stercoralis and Schistosoma spp. were identified at species rank. Notably, 28S rRNA sequencing of Leishmania spp. was limited to genus identification; however, species identification informs clinical decisions (6), underscoring the importance of organism-specific assays (7). Despite these limitations, our results indicate that fungal PCR may prove a valuable adjunct in the detection of rare eukaryotic pathogens when suspected by visualization in histologic sections or from serologic testing and clinical presentation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lieberman JA, Bryan A, Mays JA, Stephens K, Kurosawa K, Mathias PC, Sen Gupta D, Bourassa L, Salipante SJ, Cookson BT. 2021. High clinical impact of broad-range fungal PCR in suspected fungal sinusitis. J Clin Microbiol 59:e 0095521. doi:10.1128/JCM.00955-2134406798 PMC 8525558 · doi ↗ · pubmed ↗
- 2Konnick EQ, Chow S-K, Reder NP, Sengupta DJ, Hoogestraat DR, Pottinger PS, Abbott AN, Monsaas PW, Kurosawa K, Stephens K, Salipante SJ, Yeung CCS. 2016. Incidental identification of Strongyloides stercoralis infection by broad-range 28S r DNA gene sequencing in a patient with a hematolymphoid malignancy. Diagn Microbiol Infect Dis 86:362–364. doi:10.1016/j.diagmicrobio.2016.08.02927645607 · doi ↗ · pubmed ↗
- 3Harrington AT, Creutzfeldt CJ, Sengupta DJ, Hoogestraat DR, Zunt JR, Cookson BT. 2009. Diagnosis of neurocysticercosis by detection of Taenia solium DNA using a global DNA screening platform. Clin Infect Dis 48:86–90. doi:10.1086/59412819025499 PMC 2678049 · doi ↗ · pubmed ↗
- 4Rakeman JL, Bui U, Lafe K, Chen Y-C, Honeycutt RJ, Cookson BT. 2005. Multilocus DNA sequence comparisons rapidly identify pathogenic molds. J Clin Microbiol 43:3324–3333. doi:10.1128/JCM.43.7.3324-3333.200516000456 PMC 1169180 · doi ↗ · pubmed ↗
- 5Mathison BA, Bradbury RS, Pritt BS. 2023. Medical parasitology taxonomy update, June 2020–June 2022. J Clin Microbiol 61. doi:10.1128/jcm.00286-22PMC 811114233028601 · doi ↗ · pubmed ↗
- 6Aronson N, Herwaldt BL, Libman M, Pearson R, Lopez-Velez R, Weina P, Carvalho E, Ephros M, Jeronimo S, Magill A. 2017. Diagnosis and treatment of leishmaniasis: clinical practice guidelines by the Infectious Diseases Society of America (IDSA) and the American Society of Tropical Medicine and Hygiene (ASTMH). Am J Trop Med Hyg 96:24–45. doi:10.4269/ajtmh.16-8425627927991 PMC 5239701 · doi ↗ · pubmed ↗
- 7Truong TT, Crawford K, Wang-Mc Guire I, Jensen K, Mushtaq A, Lieberman NAP, Buckner FS, Van Voorhis WC, Cookson BT, Salipante SJ, Lieberman JA. 2024. Descriptive and molecular epidemiology of leishmaniasis diagnosed from clinical samples in the United States, 2021-2022. Microbiol Spectr 12:e 0105524. doi:10.1128/spectrum.01055-2439248481 PMC 11448060 · doi ↗ · pubmed ↗