Importance of Investigating Occult Gallbladder Injury in Hepatic Trauma: A Case Report
Matheus de Oliveira Santos, Larissa S Coimbra, Aline Sardow, Rafael B Pelosi, Sandro Scarpelini

TL;DR
A case report shows how a hidden gallbladder injury can occur with liver trauma and highlights the need for close monitoring and timely surgery.
Contribution
This report adds to the limited literature on occult gallbladder injuries and emphasizes the importance of early surgical intervention.
Findings
Gallbladder contusions may not be easily detected on initial imaging.
Persistent symptoms despite stable imaging require a high index of suspicion for gallbladder injury.
Laparoscopic cholecystectomy confirmed gallbladder contusion and prevented complications.
Abstract
Gallbladder injury secondary to blunt abdominal trauma is a rare condition and may be missed during the initial evaluation. We present the case of a 65-year-old male patient with a history of chronic alcohol and tobacco use who was admitted two weeks after a physical assault, with facial trauma, abdominal pain, and hemodynamic stability. Initial imaging revealed a grade III hepatic injury and mild thickening of the gallbladder wall. The patient was initially managed conservatively. However, within 48 hours, he developed persistent right upper quadrant pain, low-grade fever, leukocytosis, and a positive Murphy’s sign. Abdominal ultrasound showed thickening of the gallbladder wall and intraluminal hyperechoic content, suggestive of clots. Laparoscopic cholecystectomy confirmed gallbladder contusion with an intramural hematoma and intraluminal clots, while the liver injury showed no active…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
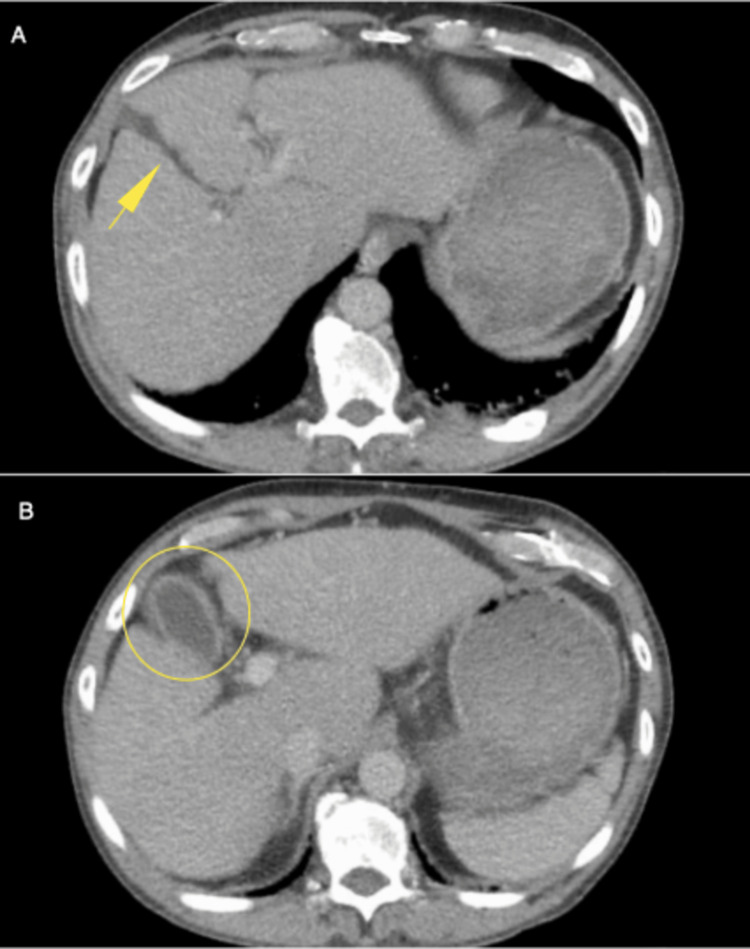 Figure 1
Figure 1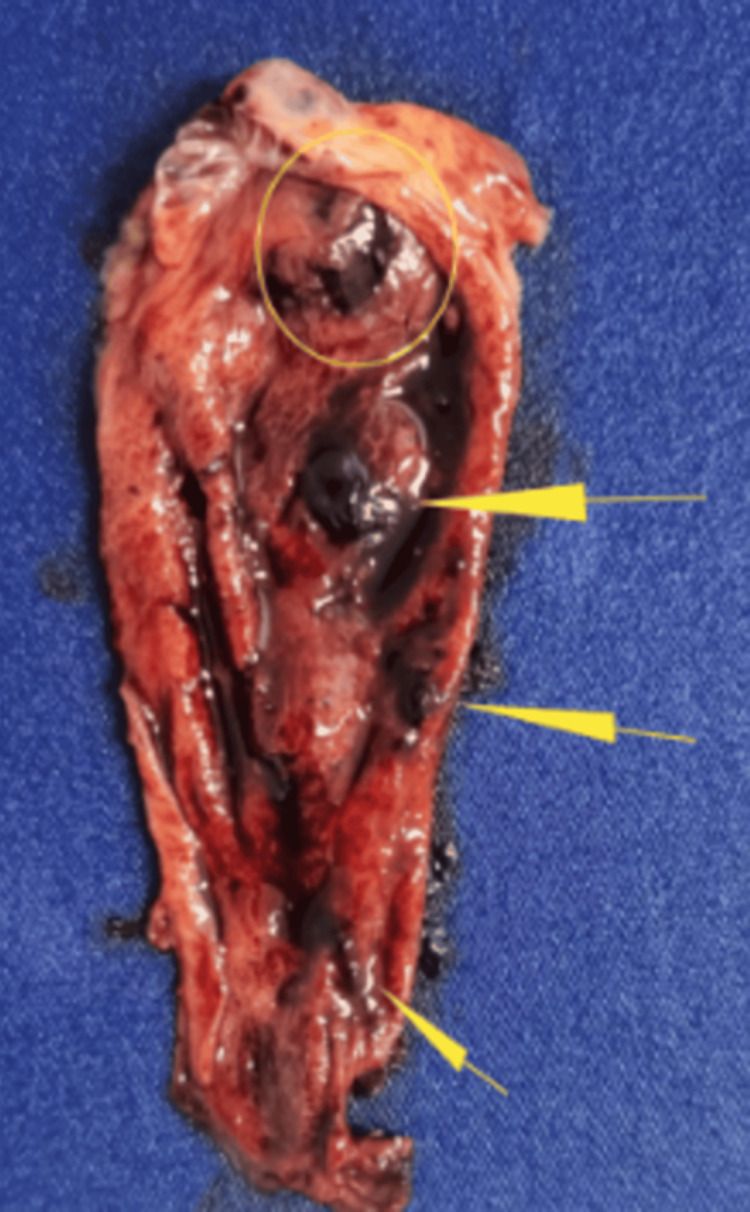 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal Trauma and Injuries · Congenital Anomalies and Fetal Surgery · Urological Disorders and Treatments
Introduction
Hepatic trauma is one of the most frequent abdominal injuries in polytrauma patients. In contrast, associated injuries of the gallbladder are rare, occurring in approximately 2% of blunt abdominal traumas and may go unrecognized during the initial assessment, leading to complications if not promptly identified and treated [1,2].
Traumatic gallbladder injuries often present with nonspecific clinical signs, making early diagnosis challenging. Symptoms may be initially subtle or masked by concomitant injuries [1]. Imaging modalities such as ultrasound and computed tomography (CT) are critical for evaluation but findings can be inconclusive in the early phase, especially when there is no significant hemoperitoneum or bile leak [3].
Clinical vigilance remains crucial in cases of blunt abdominal trauma where initial imaging does not fully explain persistent or evolving symptoms. Progressive right upper quadrant pain, fever, and leukocytosis should raise suspicion for occult gallbladder injury [2]. In such scenarios, early surgical intervention - typically through laparoscopic cholecystectomy - may be necessary to prevent complications such as bile peritonitis or secondary infection [4].
This case highlights the diagnostic challenges associated with occult gallbladder injuries following blunt abdominal trauma and emphasizes the importance of clinical vigilance and timely surgical intervention to prevent morbidity.
Case presentation
A 65-year-old male patient with no known comorbidities, and a history of chronic alcohol and tobacco use, was admitted to the Emergency Department two weeks after being assaulted. He presented with facial trauma, abdominal pain, and hemodynamic stability, without clear signs of peritonitis on initial physical examination.
Contrast-enhanced CT revealed facial fractures, a small focus of subarachnoid hemorrhage, a grade III hepatic injury in segment V, and discrete thickening of the gallbladder wall (Figures 1A-1B). The patient was initially managed conservatively with clinical monitoring and analgesic support.
A) Contrast-enhanced CT showing grade III hepatic injury in segment V (yellow arrow); B) Contrast-enhanced CT showing mild gallbladder wall thickening (transparent yellow circle).CT, computed tomography
Within the first 48 hours, the patient developed persistent right upper quadrant pain, low-grade fever, and a positive Murphy’s sign. Laboratory tests revealed leukocytosis and elevated inflammatory markers. Abdominal ultrasound showed a normally shaped gallbladder with a thickened wall (6 mm) and hyperechoic images inside suggestive of clots or stones.
He underwent laparoscopic cholecystectomy, which revealed an intramural hematoma and a large amount of clots inside the gallbladder (Figure 2). The liver injury was organizing, with no active bleeding. The patient recovered well postoperatively and was discharged the following day.
Surgical specimen image showing gallbladder with intramural hematoma (transparent yellow circle) and intraluminal clots (yellow arrows).
Discussion
Non-operative management is the gold standard for hemodynamically stable patients with liver trauma, strongly supported by the literature [5]. However, this case highlights the importance of continuous clinical surveillance, especially when symptoms persist.
Traumatic injuries of the gallbladder are rare due to the anatomical protection provided by the liver, ribs, and abdominal wall [6]. They represent less than 2% of blunt abdominal traumas [1], usually occurring in high-energy traumas or with associated injuries [7]. However, focal trauma directed at the right upper quadrant can compress the gallbladder against adjacent structures, leading to contusions, hemorrhage, or partial avulsion [8].
Injuries can be classified as contusion, laceration, or avulsion. This case fits the definition of a contusion with intramural hematoma and clots, which are often underdiagnosed in imaging studies [8]. Certain predisposing factors have been identified for gallbladder injury following blunt abdominal trauma: a thin-walled, normal gallbladder, a distended gallbladder, and alcohol ingestion [9].
Although CT and ultrasound are fundamental diagnostic tools, their sensitivity remains limited. Thus, in the setting of inconclusive imaging findings and clinical-radiological dissociation, surgical exploration becomes necessary to establish a definitive diagnosis [10]. The most common CT finding is pericholecystic fluid, although this is not specific for gallbladder injury and can be seen with other intra-abdominal injuries [11]. In our case, the persistence of pain, fever, and a positive Murphy’s sign indicated the need for intervention.
Surgical intervention allowed for a definitive diagnosis and treatment, preventing complications such as bile peritonitis or sepsis. Sharma reported that diagnosis was made intraoperatively in several cases of traumatic gallbladder injury [12], reinforcing the importance of clinical suspicion when symptoms persist.
This case adds to the scarce literature on occult gallbladder injuries after blunt trauma, highlighting the need for close clinical follow-up and a low threshold for surgical intervention.
Conclusions
This case highlights the diagnostic pitfalls associated with blunt traumatic gallbladder injuries, a rare and often underrecognized entity. The persistence of clinical signs, despite often non-specific symptoms and imaging findings, should prompt high clinical suspicion and early surgical exploration to prevent adverse outcomes. Our patient's favorable evolution after laparoscopic cholecystectomy underscores the importance of not relying solely on imaging but integrating clinical evolution into decision-making. By reporting this case, we add to the scarce body of literature on occult gallbladder injuries, providing further evidence that delayed or missed diagnosis can be avoided through attentive follow-up and timely intervention. Although this is a single case report, with inherent limitations in generalizability, it highlights the need for further case series or retrospective studies to better characterize these injuries. This report assists clinicians in recognizing similar patterns in future cases, improving the diagnostic accuracy and management of this challenging clinical scenario.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Blunt abdominal trauma resulting in gallbladder injury: a review with emphasis on pediatrics J Trauma Jaggard MK Johal NS Choudhry M 100510107020112161040410.1097/TA.0b 013e 3181 fcfa 17 · doi ↗ · pubmed ↗
- 2Isolated gallbladder injury in a case of blunt abdominal trauma J Radiol Case Rep Birn J Jung M Dearing M 25306201210.3941/jrcr.v 6i 4.941PMC 337069522690293 · doi ↗ · pubmed ↗
- 3Isolated gallbladder hematoma after a blunt abdominal trauma: case report Crit Ultrasound J Wang IT Tsai MT Huang CY Tsai KC Wu SH Lien WC Sun JT 072015
- 4Traumatic gallbladder rupture treated by laparoscopic cholecystectomy Case Rep Gastroenterol Egawa N Ueda J Hiraki M Ide T Inoue S Sakamoto Y Noshiro H 2122171020162746218810.1159/000437046 PMC 4924469 · doi ↗ · pubmed ↗
- 5Management of liver trauma in adults J Emerg Trauma Shock Ahmed N Vernick JJ 114119420112163357910.4103/0974-2700.76846 PMC 3097559 · doi ↗ · pubmed ↗
- 6Injuries of the gall-bladder Br J Surg Penn I 6366414919621448510010.1002/bjs.18004921816 · doi ↗ · pubmed ↗
- 7Trauma to the gallbladder is associated with concurrent injuries to the extra hepatic biliary system: a South African experience Injury Kong V Xu W Cheung C 981025320223436610610.1016/j.injury.2021.07.034 · doi ↗ · pubmed ↗
- 8Complete traumatic avulsion of the gallbladder Injury Losanoff JE Kjossev KT 3653681199910.1016/s 0020-1383(99)00072-810505132 · doi ↗ · pubmed ↗