The Impact of Gastroesophageal Reflux Disease on Quality of Life Among Obese Individuals in the Eastern Province of Saudi Arabia
May A Alharbi, Lama S Alahmadi, Faris Altom, Fahad W Raedi, Taif A Alahmadi, Shahed Chamsi Basha, Waleed Alkanderi, Afrah Almutairi, Thamraa N Jalfan, Hebah A Alaamri

TL;DR
This study finds that GERD significantly reduces quality of life in obese individuals in Saudi Arabia's Eastern Province, despite no strong link to BMI.
Contribution
The study provides region-specific insights into GERD's impact on quality of life among obese individuals in Saudi Arabia.
Findings
GERD prevalence was 23.1% among participants in the Eastern Province of Saudi Arabia.
GERD was associated with significantly lower quality of life scores in physical, mental, and social domains.
Obese individuals reported higher symptom severity despite BMI not being a significant predictor of GERD.
Abstract
Background Gastroesophageal reflux disease (GERD) is a widespread digestive condition globally, with obesity being a significant risk factor. GERD symptoms, such as heartburn and acid reflux, are caused by abnormal relaxation of the lower esophageal sphincter (LES), allowing stomach acid to flow back into the esophagus. Chronic symptoms can negatively impact quality of life (QoL) and may lead to complications such as esophageal adenocarcinoma. Objectives To assess the prevalence of GERD in the Eastern Province of Saudi Arabia among obese and non-obese individuals and to examine its impact on QoL. Methodology This observational, descriptive cross-sectional study was conducted from October to December 2024. Adults aged 18 years and above from the Eastern Province were recruited using convenience sampling. A self-administered questionnaire was distributed online. A total of 342…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
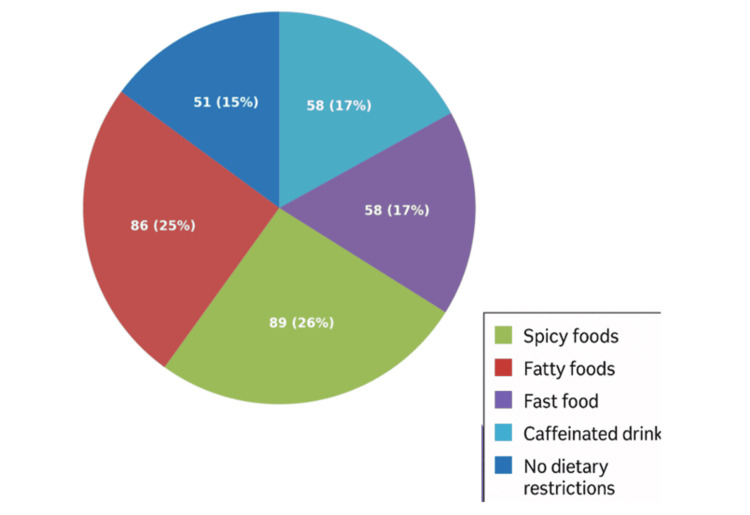 Figure 1
Figure 1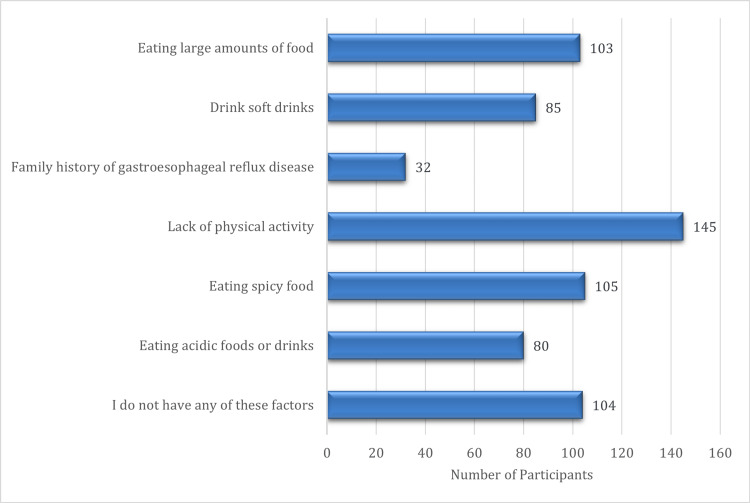 Figure 2
Figure 2| Category | Subcategory | n (%) |
| Gender | Female | 239 (69.9%) |
| Male | 103 (30.1%) | |
| Age Category | 18-29 | 179 (52.3%) |
| 30-44 | 101 (29.5%) | |
| 45-59 | 53 (15.5%) | |
| 60+ | 9 (2.6%) | |
| Nationality | Non-Saudi | 33 (9.6%) |
| Saudi | 309 (90.4%) | |
| BMI Category | Underweight (<18.5) | 23 (6.7%) |
| Average weight (18.5-24.9) | 134 (39.2%) | |
| Overweight (25-29.9) | 96 (28.1%) | |
| Obese (≥30) | 89 (26.0%) | |
| Marital Status | Single | 173 (50.6%) |
| Married | 158 (46.2%) | |
| Divorced | 10 (2.9%) | |
| Widow | 1 (0.3%) | |
| Educational Level | Elementary | 1 (0.3%) |
| Middle school | 5 (1.5%) | |
| High school | 68 (19.9%) | |
| University | 243 (71.1%) | |
| Postgraduate | 25 (7.3%) | |
| Occupation | Student | 115 (33.6%) |
| Government sector | 80 (23.4%) | |
| Private sector | 55 (16.1%) | |
| Unemployed | 79 (23.1%) | |
| Freelancer | 13 (3.8%) | |
| Income | Less than 5000 | 173 (50.6%) |
| 5000-10000 | 73 (21.3%) | |
| More than 10000 | 96 (28.1%) | |
| Smoking Status | Non-smoker | 265 (77.5%) |
| Current smoker | 27 (7.9%) | |
| Ex-smoker | 25 (7.3%) | |
| Passive smoker | 25 (7.3%) | |
| GERD Diagnosis | Yes | 79 (23.1%) |
| No | 263 (76.9%) |
| Symptom | Frequency | No GERD N (%) | Yes GERD N (%) |
| Epigastric pain or burning | Every two weeks | 23 (6.73%) | 16 (4.68%) |
| More than once a day | 12 (3.51%) | 21 (6.14%) | |
| More than once a week | 37 (10.82%) | 28 (8.19%) | |
| Once a month | 50 (14.62%) | 2 (0.58%) | |
| No symptoms | 141 (41.23%) | 12 (3.51%) | |
| Reflux of food into the throat | Every two weeks | 25 (7.31%) | 10 (2.92%) |
| More than once a day | 7 (2.05%) | 14 (4.09%) | |
| More than once a week | 29 (8.48%) | 26 (7.60%) | |
| Once a month | 52 (15.20%) | 11 (3.22%) | |
| No symptoms | 150 (43.86%) | 18 (5.26%) | |
| Heartburn | Every two weeks | 27 (7.89%) | 11 (3.22%) |
| More than once a day | 17 (4.97%) | 21 (6.14%) | |
| More than once a week | 44 (12.87%) | 32 (9.36%) | |
| Once a month | 50 (14.62%) | 3 (0.88%) | |
| No symptoms | 125 (36.55%) | 12 (3.51%) | |
| Chest pain | Every two weeks | 18 (5.26%) | 6 (1.75%) |
| More than once a day | 10 (2.92%) | 10 (2.92%) | |
| More than once a week | 12 (3.51%) | 17 (4.97%) | |
| Once a month | 24 (7.02%) | 5 (1.46%) | |
| No symptoms | 199 (58.19%) | 41 (11.99%) | |
| Chronic cough | Every two weeks | 11 (3.22%) | 4 (1.17%) |
| More than once a day | 6 (1.75%) | 14 (4.09%) | |
| More than once a week | 10 (2.92%) | 12 (3.51%) | |
| Once a month | 16 (4.68%) | 4 (1.17%) | |
| No symptoms | 220 (64.33%) | 45 (13.16%) | |
| Change in voice | Every two weeks | 7 (2.05%) | 5 (1.46%) |
| More than once a day | 5 (1.46%) | 10 (2.92%) | |
| More than once a week | 7 (2.05%) | 12 (3.51%) | |
| Once a month | 19 (5.56%) | 9 (2.63%) | |
| No symptoms | 225 (65.79%) | 43 (12.57%) | |
| Sleep disturbance | Every two weeks | 22 (6.43%) | 8 (2.34%) |
| More than once a day | 24 (7.02%) | 23 (6.73%) | |
| More than once a week | 50 (14.62%) | 29 (8.48%) | |
| Once a month | 32 (9.36%) | 3 (0.88%) | |
| No symptoms | 135 (39.47%) | 16 (4.68%) | |
| Nausea and vomiting | Every two weeks | 18 (5.26%) | 9 (2.63%) |
| More than once a day | 10 (2.92%) | 16 (4.68%) | |
| More than once a week | 28 (8.19%) | 11 (3.22%) | |
| Once a month | 28 (8.19%) | 10 (2.92%) | |
| No symptoms | 179 (52.34%) | 33 (9.65%) | |
| Dysphagia | Every two weeks | 14 (77.78%) | 4 (22.22%) |
| More than once a day | 6 (28.57%) | 15 (71.43%) | |
| More than once a week | 12 (52.17%) | 11 (47.83%) | |
| Once a month | 12 (66.67%) | 6 (33.33%) | |
| No symptoms | 219 (83.59%) | 43 (16.41%) | |
| Sore throat | Every two weeks | 9 (47.37%) | 10 (52.63%) |
| More than once a day | 7 (38.89%) | 11 (61.11%) | |
| More than once a week | 12 (60.00%) | 8 (40.00%) | |
| Once a month | 31 (70.45%) | 13 (29.55%) | |
| No symptoms | 204 (84.65%) | 37 (15.35%) | |
| Dyspepsia | Every two weeks | 13 (54.17%) | 11 (45.83%) |
| More than once a day | 22 (51.16%) | 21 (48.84%) | |
| More than once a week | 26 (50.98%) | 25 (49.02%) | |
| Once a month | 19 (95.00%) | 1 (5.00%) | |
| No symptoms | 183 (89.71%) | 21 (10.29%) | |
| Weakness or fatigue | Every two weeks | 18 (72.00%) | 7 (28.00%) |
| More than once a day | 31 (47.69%) | 34 (52.31%) | |
| More than once a week | 39 (72.22%) | 15 (27.78%) | |
| Once a month | 23 (92.00%) | 2 (8.00%) | |
| No symptoms | 152 (87.86%) | 21 (12.14%) | |
| Loss of appetite | Every two weeks | 17 (70.83%) | 7 (29.17%) |
| More than once a day | 14 (41.18%) | 20 (58.82%) | |
| More than once a week | 26 (57.78%) | 19 (42.22%) | |
| Once a month | 28 (87.50%) | 4 (12.50%) | |
| No symptoms | 178 (86.23%) | 29 (13.77%) | |
| Bloating | Every two weeks | 17 (73.91%) | 6 (26.09%) |
| More than once a day | 31 (48.44%) | 33 (51.56%) | |
| More than once a week | 38 (67.86%) | 18 (32.14%) | |
| Once a month | 25 (92.59%) | 2 (7.41%) | |
| No symptoms | 152 (88.37%) | 20 (11.63%) | |
| Diarrhea | Every two weeks | 17 (68.00%) | 8 (32.00%) |
| More than once a day | 12 (48.00%) | 13 (52.00%) | |
| More than once a week | 14 (56.00%) | 11 (44.00%) | |
| Once a month | 27 (84.38%) | 5 (15.63%) | |
| No symptoms | 193 (82.13%) | 42 (17.87%) | |
| Constipation | Every two weeks | 22 (75.86%) | 7 (24.14%) |
| More than once a day | 21 (56.76%) | 16 (43.24%) | |
| More than once a week | 29 (61.70%) | 18 (38.30%) | |
| Once a month | 29 (85.29%) | 5 (14.71%) | |
| No symptoms | 162 (83.08%) | 33 (16.92%) |
| Duration of Symptoms | No GERD (n, %) | Yes GERD (n, %) | Total |
| Less than six months | 31 (68.89%) | 14 (31.11%) | 45 |
| Six months to 1 year | 99 (96.12%) | 4 (3.88%) | 103 |
| One year to 3 years | 68 (81.93%) | 15 (18.07%) | 83 |
| More than three years | 32 (49.23%) | 33 (50.77%) | 65 |
| I had no symptoms | 33 (71.74%) | 13 (28.26%) | 46 |
| Total | 263 | 79 | 342 |
| Variable Category | No GERD (N (%) | Yes GERD N (%) | Total N (%) | p-value |
| Gender | 0.616 | |||
| Female | 182 (53.2%) | 57 (16.7%) | 239 (69.9%) | |
| Male | 81 (23.7%) | 22 (6.4%) | 103 (30.1%) | |
| Total | 263 (76.9%) | 79 (23.1%) | 342 (100%) | |
| Age Category | ||||
| 18-29 | 150 (43.9%) | 29 (8.5%) | 179 (52.3%) | 0.018 |
| 30-44 | 70 (20.5%) | 31 (9.1%) | 101 (29.5%) | |
| 45-59 | 37 (10.8%) | 16 (4.7%) | 53 (15.5%) | |
| 60+ | 6 (1.8%) | 3 (0.9%) | 9 (2.6%) | |
| Total | 263 (76.9%) | 79 (23.1%) | 342 (100%) | |
| Nationality | ||||
| Non-Saudi | 25 (7.3%) | 8 (2.3%) | 33 (9.6%) | |
| Saudi | 238 (69.6%) | 71 (20.8%) | 309 (90.4%) | |
| Total | 263 (76.9%) | 79 (23.1%) | 342 (100%) | 0.87 |
| BMI Category | ||||
| Normal weight (18.5-24.9) | 103 (30.1%) | 31 (9.1%) | 134 (39.2%) | 0.638 |
| Obese (>=30) | 71 (20.8%) | 18 (5.3%) | 89 (26.0%) | |
| Overweight (25-29.9) | 70 (20.5%) | 26 (7.6%) | 96 (28.1%) | |
| Underweight (<18.5) | 19 (5.6%) | 4 (1.2%) | 23 (6.7%) | |
| Total | 263 (76.9%) | 79 (23.1%) | 342 (100%) | |
| Marital Status | ||||
| Divorced | 6 (1.8%) | 4 (1.2%) | 10 (2.9%) | 0.005 |
| Married | 112 (32.7%) | 46 (13.5%) | 158 (46.2%) | |
| Single | 145 (42.4%) | 28 (8.2%) | 173 (50.6%) | |
| Widow | 0 (0.0%) | 1 (0.3%) | 1 (0.3%) | |
| Total | 263 (76.9%) | 79 (23.1%) | 342 (100%) | |
| Educational Level | ||||
| Elementary | 0 (0.0%) | 1 (0.3%) | 1 (0.3%) | 0.263 |
| High school | 51 (14.9%) | 17 (5.0%) | 68 (19.9%) | |
| Middle school | 4 (1.2%) | 1 (0.3%) | 5 (1.5%) | |
| Postgraduate | 22 (6.4%) | 3 (0.9%) | 25 (7.3%) | |
| University | 186 (54.4%) | 57 (16.7%) | 243 (71.1%) | |
| Total | 263 (76.9%) | 79 (23.1%) | 342 (100%) | |
| Occupation | ||||
| Freelancer | 10 (2.9%) | 3 (0.9%) | 13 (3.8%) | 0.021 |
| Government sector | 60 (17.5%) | 20 (5.8%) | 80 (23.4%) | |
| Private sector | 40 (11.7%) | 15 (4.4%) | 55 (16.1%) | |
| Student | 100 (29.2%) | 15 (4.4%) | 115 (33.6%) | |
| Unemployed | 53 (15.5%) | 26 (7.6%) | 79 (23.1%) | |
| Total | 263 (76.9%) | 79 (23.1%) | 342 (100%) | |
| Income | ||||
| 5000-10000 | 49 (14.3%) | 24 (7.0%) | 73 (21.3%) | 0.064 |
| Less than 5000 | 140 (40.9%) | 33 (9.6%) | 173 (50.6%) | |
| More than 10000 | 74 (21.6%) | 22 (6.4%) | 96 (28.1%) | |
| Total | 263 (76.9%) | 79 (23.1%) | 342 (100%) | |
| Smoking Status | ||||
| Current smoker | 19 (5.6%) | 8 (2.3%) | 27 (7.9%) | 0.542 |
| Ex-smoker | 17 (5.0%) | 8 (2.3%) | 25 (7.3%) | |
| Non-smoker | 208 (60.8%) | 57 (16.7%) | 265 (77.5%) | |
| Passive smoker | 19 (5.6%) | 6 (1.8%) | 25 (7.3%) | |
| Total | 263 (76.9%) | 79 (23.1%) | 342 (100%) | |
| Domains of QOL | GERD Mean ± SD | Non-GERD Mean ± SD | p-value |
| Physical and Mental Health | 3.3 ± 1.2 | 3.7 ± 1.1 | 0.001 |
| Social Life and Relationships | 3.3 ± 1.2 | 3.5 ± 1.2 | 0.0001 |
| Personal Abilities and Productivity | 3.3 ± 1.1 | 3.4 ± 1.2 | 0.001 |
| Environmental Aspects | 2.8 ± 1.1 | 3.0 ± 1.2 | 0.017 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastroesophageal reflux and treatments · Helicobacter pylori-related gastroenterology studies · Eosinophilic Esophagitis
Introduction
In recent years, gastroesophageal reflux disease (GERD) has emerged as a significant global health concern. It is a motility disorder caused by the frequent reflux of stomach contents into the esophagus or oral cavity. Common symptoms of GERD include heartburn, regurgitation of gastric contents into the oropharynx, dysphagia, chest pain, water brash, and globus sensation [1].
The pathophysiology of GERD is multifactorial. It involves transient relaxation and dysfunction of the lower esophageal sphincter (LES) resting tone, delayed gastric emptying, impaired peristalsis, insufficient esophageal acid clearance, reduced salivation, impaired mucosal resistance, and increased intra-abdominal pressure in obese individuals [1].
Several risk factors for GERD have been proposed, with the most established being alcohol consumption, family history of GERD, and high BMI [1].
Management of GERD requires a stepwise approach, with the primary goals being symptom control, healing of esophagitis, and prevention of complications or recurrence. Treatment includes lifestyle modification, acid suppression medications (such as antacids or proton pump inhibitors), and in certain cases, surgical intervention through antireflux procedures [2].
Pharmacological treatment is effective for approximately 80% of patients with recurrent but non-progressive GERD. However, early identification of the remaining 20% with progressive disease is critical, as they may develop serious complications such as Barrett’s esophagus or esophageal strictures. Surgical intervention is recommended early in such cases to prevent severe outcomes [2].
Our study was driven by the limited number of studies on GERD in the Eastern Region of Saudi Arabia and the observation that GERD prevalence is higher in Saudi Arabia compared to Western and East Asian countries. While the global prevalence of GERD ranges from 10% to 25%, reported rates in Saudi Arabia range from 20% to 61%, specifically, 20.4% in the Eastern Province, 61.8% in Arar, and 45.4% in Riyadh [3].
Additionally, GERD has been found to be more prevalent in older adults and is associated with several risk factors, including sociodemographic characteristics, smoking, family history, high BMI, types of food and beverages, fast food diets, physical inactivity, and various health conditions. Food and dietary habits have been linked to GERD in numerous studies. Spicy foods, in particular, are known triggers, and one study observed a negative association between coffee consumption and GERD symptoms [4].
High BMI is considered a major risk factor in the development of GERD. Cross-sectional epidemiological studies have consistently shown that obese individuals are more likely to experience GERD than those with a normal BMI [5].
Therefore, the purpose of this study is to increase awareness of the relationship between GERD and obesity. Given the scarcity of published research on this topic in the Eastern Region, and the lack of studies that include a control group, we aimed to address this gap by including both obese and non-obese participants. We also focused on the relationship between meal-to-sleep intervals and GERD risk and severity, an aspect that was overlooked in a previous cross-sectional study conducted in the Eastern Province of Saudi Arabia [6].
Materials and methods
This study was an observational, descriptive, cross-sectional study conducted across various cities in the Eastern Province of Saudi Arabia, including Dammam, Aseer Province, Al-Khobar, Al-Jubail, Hofuf, and Ras Tanura. Data collection was carried out over a three-month period, from October 2024 to December 2024. The study population included male and female participants aged 18 years and older, both Saudi and non-Saudi individuals, with a BMI of 30 kg/m² or higher. Only residents of the Eastern Province were included, while pregnant women were excluded. The estimated sample size was 314 participants, calculated using Epi Info software version 7.2 (Centers for Disease Control and Prevention, Atlanta, GA, USA), based on a 95% confidence level and a 5% margin of error. A convenience sampling technique was used to recruit participants.
Data collection methods, instruments used, and measurements
A self-administered questionnaire was distributed through Google Forms via social media platforms, including WhatsApp, Telegram, and X (formerly Twitter). To maximize reach and participation from the target population, periodic announcements were posted to reshare the questionnaire link on these platforms. The questionnaire consisted of six sections. Sections one to four collected socio-demographic information, including gender, age, nationality, pregnancy status, place of residence, marital status, educational level, monthly income, occupation, body weight, height, and smoking status. The fifth section assessed whether the participant had been diagnosed with GERD, while the sixth section measured and evaluated GERD symptoms, their duration, and the presence of additional symptoms. The questionnaire was adapted from a previous study on GERD prevalence conducted in Abha [4]. Additionally, seven questions were added to address limitations noted in recent research on GERD in the Eastern Province of Saudi Arabia [6]. BMI was calculated by dividing weight in kilograms by the square of height in meters. The classification of BMI followed WHO guidelines: underweight (<18.5), healthy weight (18.5-24.9), overweight (25-29.9), and obese (≥30) [7].
A pilot study was conducted with ten individuals and staff members to identify any ambiguous or confusing items. Following the pilot, three experts reviewed the questionnaire to assess its validity and reliability. One week later, the questionnaire was re-administered to the same pilot participants to evaluate test-retest reliability.
Data management and analysis plan
The data were entered into a Microsoft Excel sheet and subsequently analyzed using the SPSS. Data from participants involved in the pilot study, as well as those who met the exclusion criteria, were not included in the final analysis. Categorical variables were summarized as frequencies (numbers and percentages), while measures of central tendency (mean, median) were calculated for continuous variables. A p-value of <0.05 was considered statistically significant. Chi-square tests were used to assess whether there were significant differences between the expected and observed frequencies across categories.
Statistical analysis
The data were cleaned, managed, and coded using Microsoft Excel 2019 (Microsoft Corporation, Redmond, WA). Statistical analyses were conducted using R (RStudio, version 1.4.1106; RStudio, Inc.). Descriptive statistics were generated, including frequency distributions and cross-tabulations, which were assessed using the chi-square test. Confidence intervals (95% CI) were calculated, and multivariate logistic regression analysis was applied to identify predictors of the dependent variables. A p-value of less than 0.05 was considered statistically significant.
Ethical considerations
Ethical approval for the study was obtained from the Ethics Committee of King Faisal University (#KFU-REC-2024-SEP-ETHICS2604). Participation in the study was entirely voluntary, with no incentives or rewards offered. All participants were informed about the purpose of the study and their right to refuse participation or withdraw at any point without consequence. Confidentiality and privacy of all participants were maintained throughout the research process.
Results
Out of 438 participants, 342 were included after exclusions. As presented in Table 1, the majority were female (239; 69.9%) and aged 18-29 years (179; 52.3%). Most participants were Saudi nationals (309; 90.4%) and were classified as having average weight (134; 39.2%), followed by overweight (96; 28.1%) and obese (89; 26.0%). Regarding marital status, 173 (50.6%) were single, while 158 (46.2%) were married. The majority held a university degree (243; 71.1%). Occupationally, 115 (33.6%) were students, followed by participants employed in the government (80; 23.4%) and private sectors (55; 16.1%). Income levels showed that 173 (50.6%) earned less than 5,000 SAR per month. Regarding smoking status, 265 (77.5%) of participants were non-smokers. Finally, 79 (23.1%) of the participants were diagnosed with GERD.
The prevalence of GERD symptoms among the 342 participants is presented in Table 2. Overall, 153 (44.7%) participants reported no epigastric pain, including 141 (41.2%) without GERD and 12 (3.5%) with GERD. Frequent epigastric pain (more than once per week) affected 98 (28.7%) participants, equally distributed between the GERD and non-GERD groups (49; 14.3% each). Food reflux occurring more than twice per week was reported by 55 (16.1%) participants, with a higher prevalence among those with GERD (40; 11.7%) compared to non-GERD participants (15; 4.4%). Heartburn was reported more than twice per week by 76 (22.2%) participants, predominantly among the GERD group (53; 15.5%) compared to the non-GERD group (23; 6.7%).
Table 3 shows that symptom duration varied among participants. Of the 342 participants, 64 (18.7%) had no GERD symptoms. Short-term symptoms (<6 months) were reported by 45 (13.2%), while 103 (30.1%) had symptoms lasting 6-12 months. A duration of 1-3 years was reported by 83 (24.3%), and 65 (19.0%) experienced symptoms for more than three years. Notably, long-term symptoms (>3 years) were nearly equally distributed between the GERD (33; 50.8%) and non-GERD (32; 49.2%) groups.
Table 4 shows that GERD was significantly associated with age (p = 0.018, Cramér’s V = 0.17), marital status (p = 0.005, Cramér’s V = 0.19), and occupation (p = 0.021, Cramér’s V = 0.18). Higher GERD rates were observed in the 30-44 age group, among married individuals, and those who were unemployed or employed in the government sector. Other factors such as gender, nationality, BMI, education, income, and smoking status showed no significant association with GERD (p > 0.05), though slightly higher GERD prevalence was noted among non-smokers and those with lower income.
Comparisons of different quality of life (QoL) domains and sociodemographic characteristics are shown in Table 5. Participants with GERD had significantly lower scores in physical and mental health (3.3 ± 1.2 vs. 3.7 ± 1.1, p = 0.001), social life and relationships (3.3 ± 1.2 vs. 3.5 ± 1.2, p = 0.0001), and personal abilities and productivity (3.3 ± 1.1 vs. 3.4 ± 1.2, p = 0.001). Environmental aspect scores were also lower among the GERD group (2.8 ± 1.1 vs. 3.0 ± 1.2, p = 0.017).
As illustrated in Figure 1, food avoidance patterns among study participants (N = 342) revealed that spicy foods were the most frequently avoided dietary category (89; 26%), followed closely by fatty foods (86; 25.1%). Equal proportions of participants reported avoiding fast food and caffeinated beverages/soft drinks (58; 17%) each. A smaller subset (51; 14.9%) reported no dietary restrictions from the listed categories.
Patterns of food avoidance among study participants.
Figure 2 presents the self-reported risk factors associated with GERD among study participants. The most frequently identified risk factor was lack of physical activity (n = 145), followed by eating spicy food (n = 105), eating large amounts of food (n = 103), and the absence of any identifiable risk factors (n = 104). Other commonly reported factors included drinking soft drinks (n = 85) and consuming acidic foods or beverages (n = 80). Only 32 participants reported a family history of GERD as a risk factor. These findings emphasize the importance of lifestyle-related behaviors, particularly diet and physical activity, in the development and management of GERD.
Risk factors of GERD among the participants.GERD: Gastroesophageal reflux disease.
Discussion
This study investigated the prevalence, risk factors, and effects of GERD among 342 mostly young Saudi nationals, with a significant majority being female (69.9%) and well-educated (71.1% possessing university degrees). The results underscore a substantial burden of GERD symptoms, correlations with lifestyle and sociodemographic characteristics, and a marked deterioration in QOL among those affected.
The research indicated a significant prevalence of GERD symptoms, with 22.2% of subjects reporting recurrent heartburn and 16.1% experiencing food reflux. These findings correspond with earlier research in Saudi Arabia, indicating a GERD prevalence between 20% and 45%, highlighting an escalating health issue in the region [8]. Chronic cough, dysphagia, and sleep problems were prevalent among GERD patients, aligning with global literature that associates GERD with extra-esophageal symptoms [9]. A significant percentage of individuals (26%) abstained from spicy meals and 25% from fatty foods, indicating that dietary alterations are a common self-management tactic; however, therapeutic advice may be required for optimal symptom regulation.
Identified key risk variables included physical inactivity, reported by 145 participants, and the consumption of spicy foods. These findings align with global studies linking sedentary lifestyles and specific dietary practices to a heightened risk of GERD [10]. The study found that 28.1% of participants were overweight and 26% were obese, supporting the link between obesity and GERD, which is attributed to increased intra-abdominal pressure and dysfunction of the lower esophageal sphincter [11]. However, this study did not identify a statistically significant correlation between BMI and GERD, in contrast to some previous research, potentially due to the younger age demographic or sample characteristics.
Age and marital status showed a significant correlation with GERD (p = 0.018 and p = 0.005, respectively), with older and married individuals demonstrating a higher prevalence of symptoms. This may be attributed to lifestyle modifications, stress, or dietary habits associated with married life [12]. Notably, gender, educational attainment, and wealth did not exhibit significant correlations, contrary to several studies indicating a higher frequency of GERD among males or individuals from lower socioeconomic strata [13]. This discrepancy may be due to the predominantly young, female, and educated sample in this study.
A troubling discovery was that 50.8% of GERD participants reported symptoms persisting for over three years, suggesting chronicity and possible inadequate treatment. In contrast, 71.7% of individuals without GERD reported no symptoms, highlighting the importance of early identification and management of GERD to avoid complications such as esophagitis or Barrett’s esophagus [14]. The significant prevalence of chronic sufferers may indicate deficiencies in healthcare access, awareness, or treatment compliance.
GERD markedly reduced participants’ QoL, especially in the physical and mental health domains (p = 0.001). The adverse impacts on social life, productivity, and general well-being correspond with global evidence indicating that GERD diminishes work performance and daily functioning [15]. The research emphasizes the necessity for comprehensive GERD management, incorporating nutritional guidance, lifestyle changes, and psychological support to alleviate these effects.
Limitations
This study has several limitations, notably its cross-sectional design, which prevents causal inferences. The predominance of young, educated women may limit generalizability to other demographic groups. Moreover, the use of self-reported symptoms introduces the possibility of recall bias. Future long-term research using diverse samples and objective diagnostic methods (e.g., endoscopy) could enhance the validity of these findings.
Conclusions
GERD is a common and burdensome condition among young Saudi individuals, significantly affecting their quality of life. While key modifiable risk factors include dietary habits and physical inactivity, this study also identified a significant association between GERD and both age and marital status. Public health strategies that encourage healthier lifestyles, early medical evaluation, and comprehensive GERD management are essential to alleviating its burden. Future research should focus on long-term outcomes and effective treatment strategies in similar populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gastroesophageal reflux disease Prim Care Kellerman R Kintanar T 5615734420172913252010.1016/j.pop.2017.07.001 · doi ↗ · pubmed ↗
- 2Gastroesophageal Reflux Disease Antunes C Aleem A Curtis SA Treasure Island, FL Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 441938/28722967 · pubmed ↗
- 3Prevalence of gastroesophageal reflux disease and its impact on the quality of life among obese individuals in Al-Baha Region, Saudi Arabia Cureus Elshennawy AT Shatla IM Agwa RH 016202410.7759/cureus.63073 PMC 1120032038933342 · doi ↗ · pubmed ↗
- 4Prevalence and factors associated with gastroesophageal reflux disease among primary health care attendants at Abha city, southwestern Saudi Arabia Saudi Pharm J Alsaleem MA Awadalla NJ Shehata SF 597602292021 https://www.sciencedirect.com/science/article/pii/S 13190164210007733419426610.1016/j.jsps.2021.04.020PMC 8233534 · doi ↗ · pubmed ↗
- 5Obesity and GERD Gastroenterol Clin North Am Chang P Friedenberg F 1611734320142450336610.1016/j.gtc.2013.11.009PMC 3920303 · doi ↗ · pubmed ↗
- 6Prevalence of gastroesophageal reflux disease and associated risk factors in the Eastern Region, Saudi Arabia Cureus Al Ghadeer HA Alabbad ZE Al Shaikh SB 013202110.7759/cureus.19599 PMC 867107634926068 · doi ↗ · pubmed ↗
- 7Body mass index (BMI): a screening tool analysis Cureus Khanna D Peltzer C Kahar P Parmar MS 014202210.7759/cureus.22119 PMC 892080935308730 · doi ↗ · pubmed ↗
- 8Obesity is an independent risk factor for GERD symptoms and erosive esophagitis Am J Gastroenterol El-Serag HB Graham DY Satia JA Rabeneck L 124312501002005 https://journals.lww.com/ajg/abstract/2005/06000/obesity_is_an_independent_risk_factor_for_gerd.7.aspx 1592975210.1111/j.1572-0241.2005.41703.x · doi ↗ · pubmed ↗