Acute rupture of a sinus of Valsalva aneurysm with dehiscence of the tricuspid valve
Maxwell Marlowe, Jeffrey Weiner, English Flack, Craig Mathis, Karla G. Christian, Garrett N. Coyan

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
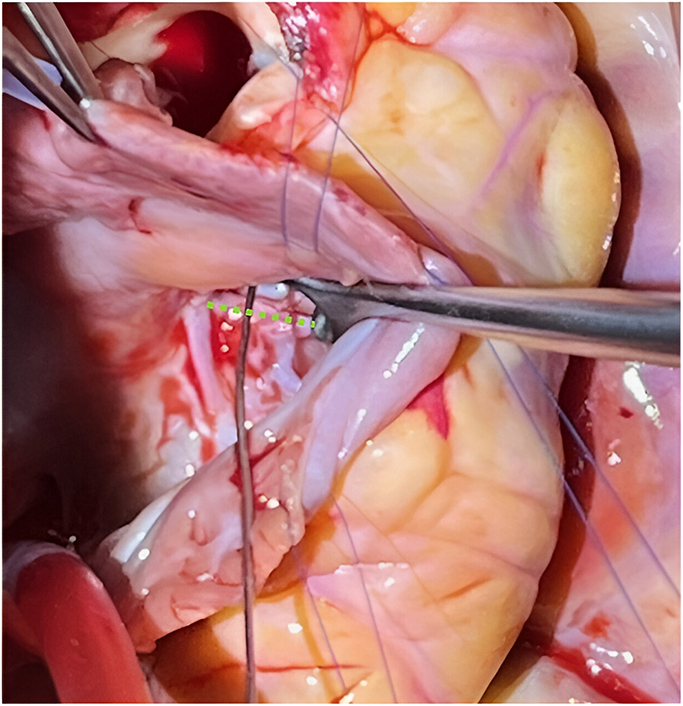 Figure 1
Figure 1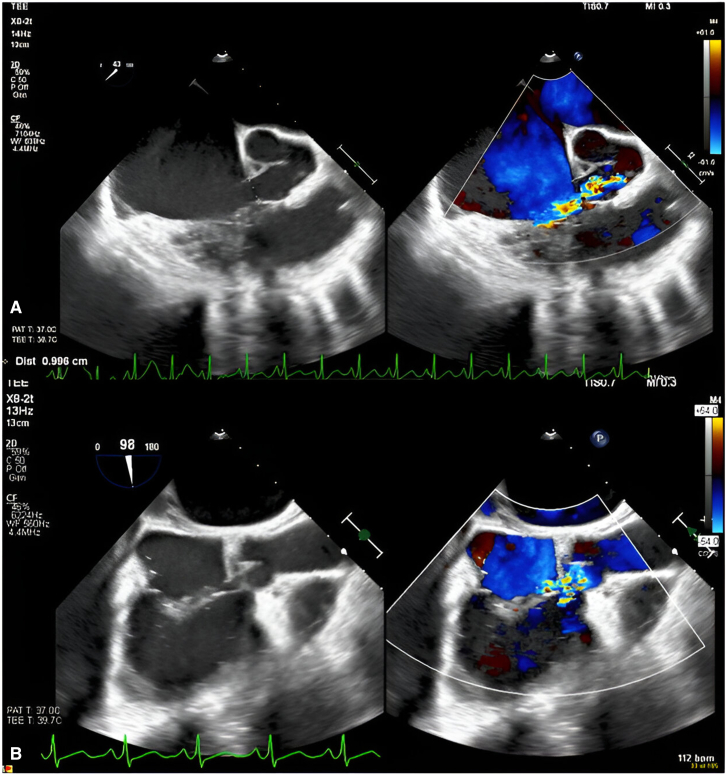 Figure 2
Figure 2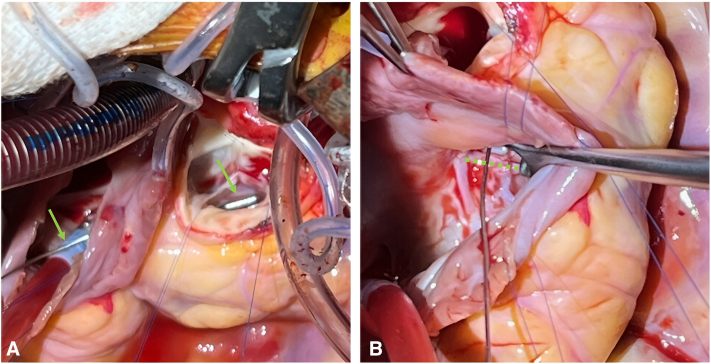 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Artery Anomalies · Aortic Disease and Treatment Approaches · Infective Endocarditis Diagnosis and Management
Ruptured SOVA with dehiscence of the tricuspid valve (dotted green line). Central MessageA unique case of tricuspid valve dehiscence due to ruptured sinus of Valsalva aneurysm required valve resuspension and commissuroplasty for successful repair.
Ruptured sinus of Valsalva aneurysm (SOVA) can present urgently and most commonly rupture into the right ventricle (RV). We present a unique case of spontaneous rupture of a right SOVA into the atrioventricular junction, leading to dehiscence of the anterior leaflet of the tricuspid valve (TV). Institutional review board approval was not required; informed written consent for publication was obtained.
Case Report
An otherwise-healthy 15-year-old male athlete with a previously normal findings on transthoracic echocardiogram (TTE) performed for murmur evaluation and no evidence of infection presented to his primary physician with 3 days of chest pain, tachypnea, orthopnea, and new murmur. TTE obtained upon transfer to our facility demonstrated 9-mm rupture of a right SOVA into the right atrium (RA) with a 7-mm perimembranous ventricular septal defect (VSD). Preoperative transesophageal echocardiogram showed a 1-cm right SOVA ruptured into the RA, mild tricuspid regurgitation (TR), and a perimembranous VSD (Figure 1).Figure 1A, TEE depicting an ∼1-cm ruptured SOVA with color flow Doppler demonstrating aliased flow along the apical portion of the tricuspid valve. B, TEE image depicting color flow originating from the ruptured SOVA splaying over the tricuspid valve annulus. The ventricular portion was initially considered a VSD; however, there was no VSD on direct examination, so this was attributable to the flow pattern around the dehiscence defect of the tricuspid valve. TEE, Transesophageal echocardiogram; SOVA, sinus of Valsalva aneurysm; VSD, ventricular septal defect.
Intraoperative inspection via the aortic root and RA demonstrated a 1-cm ruptured right SOVA into the RA/RV junction with dehiscence of the TV at the anterior-septal commissure (Figure 2). There was no VSD, and tricuspid chordal apparatus was intact. The internal aneurysmal sac was resected, and the sinus was patched internally from the aortic side with an autologous pericardial patch and a running 6-0 polypropylene suture. The TV was resuspended with two 5-0 polypropylene pericardial-pledgeted mattress sutures passed inferior to superior through the annulus and valve leaflets, sandwiching the SOVA aneurysm tract edges to reenforce closure from the atrial side. Anterior-septal commissuroplasty was performed to improve TV function. The patent foramen ovale was closed before RA closure and weaning from cardiopulmonary bypass.Figure 2A, Metal coronary probe (green arrows) passing from the right atrioventricular junction through the ruptured sinus of Valsalva aneurysm into the right coronary sinus of the aorta after aneurysm sac resection. B, Metal probe passing through the ruptured sinus of Valsalva aneurysm, the anterior septal commissure of the tricuspid valve is detached/delaminated from the annulus (dotted green line) in this region.
Postoperative transesophageal echocardiogram showed no residual shunting, trivial to mild TR, and normal biventricular function. The patient was extubated in the operating room, transferred from the intensive care unit on postoperative day 1, and discharged on postoperative day 3.
He was readmitted 2 weeks later with atrial flutter requiring cardioversion and sotalol with subsequent rhythm control. He has returned to baseline functional status, and follow-up TTE demonstrated stable repair and normalized right-sided chamber sizes.
Discussion
SOVA is rare and can be either congenital or acquired. The most common location of SOVA is the right coronary sinus, most commonly rupturing into the RV. Tricuspid involvement is infrequent and has been rarely described in literature. The most common reports of involvement being associated with the “windsock” of the aneurysm, causing coaptation defect in the valve or high-velocity ruptured SOVA flow, leading to forced systolic opening of the TV.1 The effects of SOVA can lead to either TR or stenosis.2 One case described the septal leaflet as being “traumatized” but intact, and it was repaired by tricuspid annuloplasty.3
This case was unique in that the ruptured SOVA led to dehiscence of the anterior leaflet of the TV requiring surgical resuspension of the TV. The large shunt from the ruptured SOVA and the location near the anterior septal commissure likely led to the suspicion that the shunt was a VSD, but direct inspection revealed this flow pattern was attributable to flow around the dehisced TV. This diagnostic possibility should be considered in acute rupture scenarios and can be addressed by resuspension of the TV while supporting the SOVA repair from the right atrial-ventricular junction. Additional support and repair techniques such as commissuroplasty can also be applied to minimize tricuspid valve regurgitation, and annuloplasty may be indicated to support repairs in patients with a dilated annulus/complex repair. As the result of extreme right-sided chamber dilation, postoperative arrhythmias can also be seen and should be managed per institutional protocols.
Conflict of Interest Statement
The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wilson V.C.Jacob A.van der Walt L.M.Sasse A.A multimodality approach to a rare case of ruptured sinus of Valsalva aneurysm with tricuspid valve involvement: a case report Eur Heart J Case Rep 792023 ytad 45410.1093/ehjcr/ytad 454PMC 1051665937743896 · doi ↗ · pubmed ↗
- 2Kuroda M.Takahashi K.Matsumoto S.Oshima M.Impact of intraoperative transesophageal echocardiography for noncoronary sinus of Valsalva aneurysm with severe tricuspid regurgitation J Cardiothorac Vasc Anesth 3482020216921733222402310.1053/j.jvca.2020.02.034 · doi ↗ · pubmed ↗
- 3Gibbs K.L.Reardon M.J.Strickman N.E.Hemodynamic compromise (tricuspid stenosis and insufficiency) caused by an unruptured aneurysm of the sinus of Valsalva J Am Coll Cardiol 75198611771181395837710.1016/s 0735-1097(86)80242-x · doi ↗ · pubmed ↗