B-cell extracellular vesicle biomarkers for detection of antibody-mediated rejection in lung transplantation
Laxminarayana Korutla, Yun Zhu Bai, Nicole DeMarais, Sriharsha Talapaneni, Robert Hu, Vincent Burke, Daniel Kreisel, Prashanth Vallabhajosyula

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
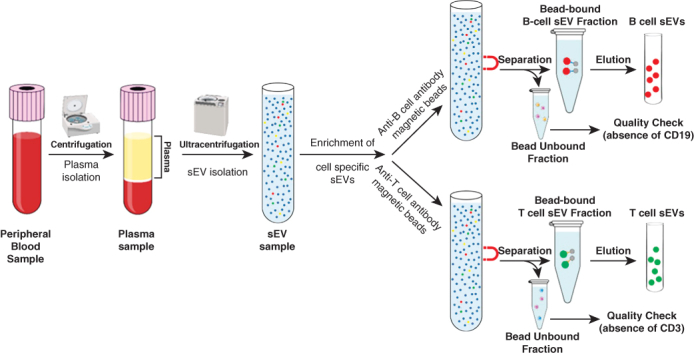 Figure 1
Figure 1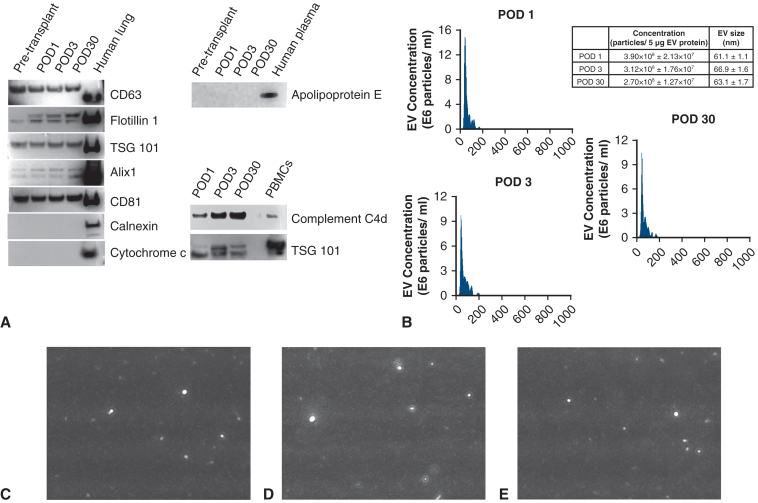 Figure 2
Figure 2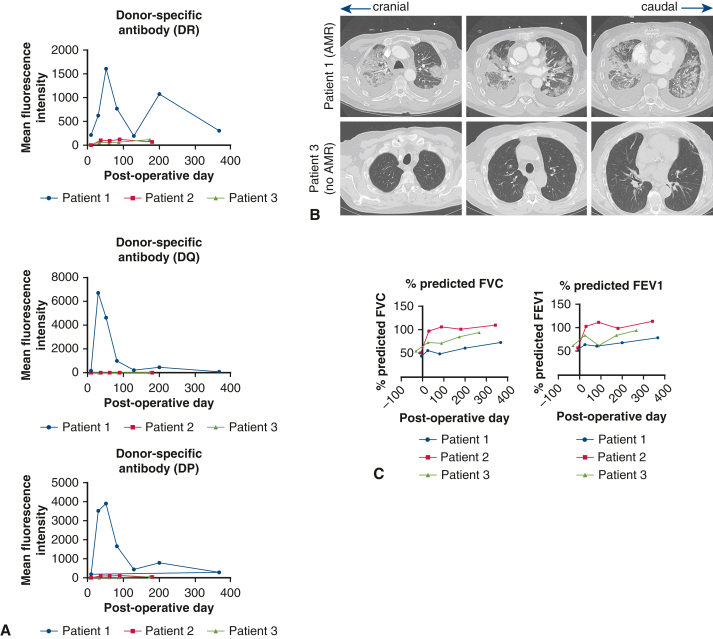 Figure 3
Figure 3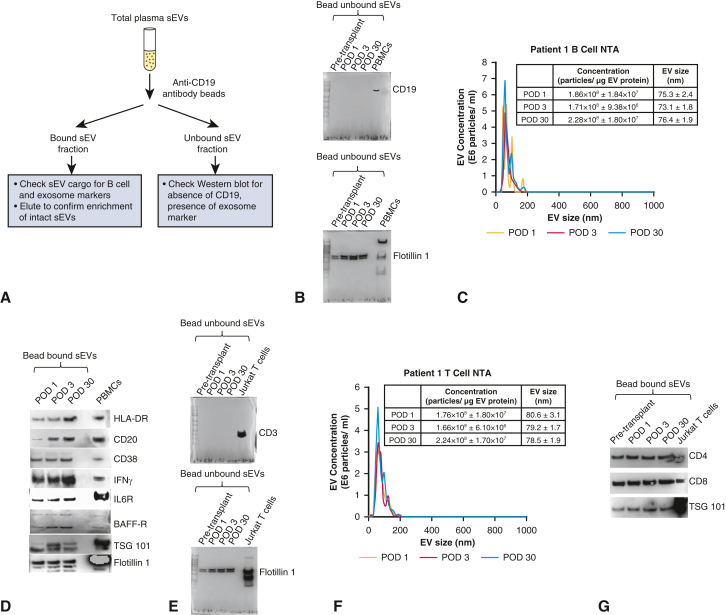 Figure 4
Figure 4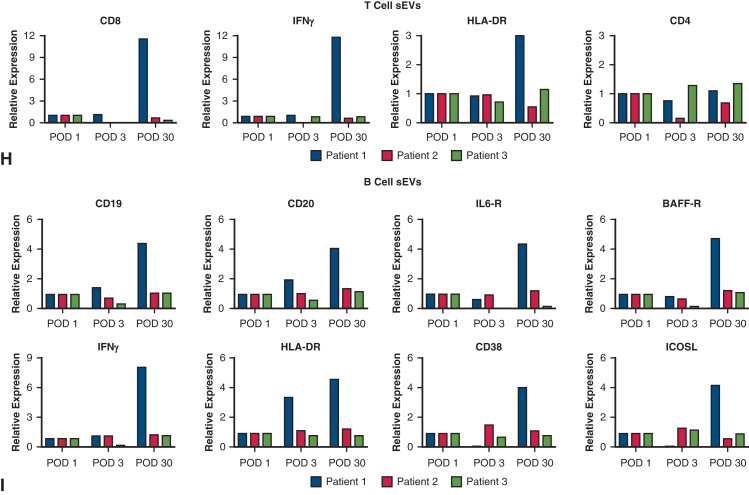 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Renal Transplantation Outcomes and Treatments · Medical Imaging and Pathology Studies
B-cell small extracellular vesicle enrichment as biomarkers of antibody mediated rejection. Central MessageThere is a critical need for biomarkers of AMR. We developed a novel circulating B-cell extracellular vesicle platform as biomarker of AMR in lung transplantation.
Lifelong surveillance for allograft rejection is a major cornerstone of care for patients after lung transplant. Antibody-mediated rejection (AMR) significantly contributes to allograft dysfunction, yet its noninvasive diagnosis and treatment monitoring remain challenging.1 We have been investigating cell/tissue-specific small extracellular vesicles (sEVs) as noninvasive biomarkers for transplant rejection monitoring, including in lung transplantation.2^,^3 We recently developed a novel biomarker platform for acute cellular rejection (ACR) monitoring based on T-cell sEV cargo profiling.4 Building on this, we hypothesized that because ACR leads to changes in circulating T-cell sEVs, AMR would induce changes in circulating B-cell sEV cargoes, enabling its noninvasive diagnosis. B-cell–specific EV enrichment from peripheral blood has never been reported before and the biology of circulating B-cell EVs in transplantation remains largely unexplored. Thus, our platform introduces a novel approach to noninvasive AMR monitoring. Herein, we report the development of a B-cell–specific sEV platform that demonstrated distinct cargo changes in a patients undergoing lung transplant with AMR compared with 2 patients without AMR/ACR.
We studied 3 bilateral lung transplant recipients (patients 1-3). Patient 1 developed mixed AMR and ACR; patients 2 and 3 did not have ACR or AMR. Peripheral blood was collected on postoperative days (PODs) 1, 3, and 30, with surveillance transbronchial lung biopsies performed on POD 30. Unlike patients 2 and 3, patient 1 developed de novo donor-specific antibodies on POD 30 and presented with dyspnea and pulmonary infiltration on computed tomography (Figure 1, A and B). Pulmonary function tests were performed for functional vital capacity and forced expiratory volume in 1 second measurements (Figure 1, C). This demonstrated improvement in functional vital capacity and forced expiratory volume in 1 second compared with pretransplant measurements in all 3 patients, but the least improvement was seen in patient 1 (Figure 1, C). This patient received treatment for mixed ACR/AMR with thymoglobulin, high-dose steroids, carfilzomib, tocilizumab, and intravenous immunoglobulin therapy. Patients 2 and 3 had uneventful postoperative courses without development of donor-specific antibodies and biopsies demonstrating no ACR or AMR.Figure 1. Pertinent clinical data for patients 1 to 3 are shown. A, Donor-specific antibody titers for human leukocyte antigen (HLA) DQ, HLA-DP, and HLA-DR in patients 1 through 3 are shown. Patient 1 showed acute upregulation of donor-specific antibodies at the postoperative day 30 time point. B, Computed tomography imaging is shown for patients 1 and 3. Acute bilateral infiltration was noted in patient 1 at the postoperative day 30 time point. C, Pulmonary function tests for patients 1 through 3 are shown. Compared with pretransplant lung volumes, all 3 patients demonstrated improved forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1) after bilateral lung transplantation, but patient 1 showed the least improvement.
We isolated plasma sEVs enriched with exosomes using serial ultracentrifugation (Appendix E1), characterized sEVs per the Society of Extracellular Vesicles guidelines,5 including expression of exosome markers CD63, flotillin-1, TSG101, alix-1, and CD81 on Western blot, along with absence of calnexin (endoplasmic reticulum marker), cytochrome c (mitochondria marker), and apolipoprotein E (plasma lipoprotein marker) (Figure E1, A, and Table E1). By nanoparticle tracking analysis, the isolated nanoparticles phenotyped as sEVs (Figure E1, B-E). B-cell–specific sEVs were enriched from the plasma sEV pool using anti-CD19 antibody-conjugated beads (Figure 2, A). As quality control, the bead-unbound sEVs were analyzed for the absence of CD19 but presence of flotillin-1 (Figure 2, B). The bead-bound sEVs representing B-cell sEVs were analyzed by nanoparticle tracking analysis (Figure 2, C) and Western blot for expression of B-cell activation protein markers, including CD20, class II human leukocyte antigen (HLA)-DR, CD38, interferon gamma (IFNγ), interleukin 6 receptor, and B-cell activating factor receptor (Figure 2, D). Furthermore, several of these markers were more highly expressed at the POD 30 time point of AMR diagnosis in patient 1. Similarly, we enriched T-cell sEVs using anti-CD3 antibody-conjugated beads and analyzed both bound and unbound fractions (Figure 2, E-G).4 Collectively, this suggested that AMR may lead to changes in protein cargoes of circulating B-cell sEVs.Figure 2. Circulating T-cell sEV and B-cell small extracellular vesicles (sEV) cargoes in a patient undergoing lung transplant with mixed acute cellular rejection/antibody-mediated rejection (ACR/AMR). A, Workflow for B cell sEV enrichment and downstream analysis is shown. B, Anti-CD19 antibody bead-unbound sEVs were analyzed by Western blot for CD19 absence and flotillin-1 (exosome marker) expression. Patient 1 data are shown. Peripheral blood mononuclear cells (PBMCs) are positive control. C, For patient 1, nanoparticle tracking analysis (NTA) of eluted anti-CD19 antibody bead-bound sEVs is shown. D, For patient 1, Western blot for expression of B-cell activation markers human leukocyte antigen (HLA) DR, CD20, CD38, interferon gamma (IFNγ), interleukin 6 receptor (IL6-R), B-cell activating factor receptor (BAFF-R), and exosome markers TSG101 and flotillin-1 in B-cell sEVs is shown. E, Western blot of T-cell sEVs, enriched from plasma total sEV pool using anti-CD3 antibody beads, is shown for CD3 absence and flotillin-1 expression in patient 1. Jurkat T-cells positive control is shown. F, NTA of eluted T-cell sEVs is shown for patient 1. G, Western blot for expression of T-cell markers, CD4, and CD8 in T-cell sEVs is shown for patient 1. H, Reverse transcription quantitative real-time polymerase chain reaction (RT-qPCR) assays for T-cell sEV messenger RNA cargoes CD8, IFNγ, HLA-DR, and CD4 in patients 1 through 3 at postoperative days (PODs) 1, 3, and 30 time points are shown. Upregulation of T-cell activation markers CD8, IFNγ, and HLA-DR, was seen at POD 30 time point in patient 1 only. I, RT-qPCR assays for B-cell sEV messenger RNA cargoes, CD19, CD20, IL6-R, BAFF-R, IFNγ, HLA-DR, CD38, and inducible co-stimulator ligand (ICOSL), in patients 1 through 3 at PODs 1, 3, and 30 time points are shown. Upregulation of these markers was observed in patient 1, POD 30 time point of AMR.
Next, we developed methodologies for characterization of messenger RNA (mRNA) cargoes of sEVs by reverse transcription quantitative real-time polymerase chain reaction.E1 For ACR, we quantified T-cell sEV mRNA cargoes for markers of T-cell alloreactivity (CD8, IFNγ, HLA-DR, and CD4) (Table E2). We compared relative expression at PODs 3 and 30 to POD 1 (baseline). Patient 1 with mixed ACR/AMR showed upregulation of markers of T-cell alloreactivity, including CD8, IFNγ, and HLA-DR on POD 30 (Figure 2, H), whereas patients 2 and 3 exhibited marker expression levels similar to baseline across all time points (Figure 2, H). During AMR, alloreactive B-cells become activated and upregulate expression of several markers, including CD19, CD20, interleukin 6 receptor, B-cell activating factor receptor, IFNγ, HLA-DR, CD38, and inducible co-stimulator ligand.E2 Therefore, we assessed whether circulating B-cell sEVs carry the mRNA signatures for these markers, and if so, whether they are upregulated with AMR. We developed reverse transcription quantitative real-time polymerase chain reaction assays for these 8 mRNAs for analysis in B-cell sEVs. In patient 1, these markers of B-cell activation were upregulated at the POD 30 time point compared with the PODs 1 and 3 time points, coinciding with AMR/ACR diagnosis and treatment (Figure 2, I). Patients 2 and 3 showed unchanged B-cell sEV marker expression across all time points (Figure 2, I). These results demonstrate that B-cell sEV cargoes, which reflect increased B-cell alloreactivity, were selectively upregulated only in the patient who developed AMR.
Conclusions
We detail the development of a circulating B-cell sEV platform that demonstrated time-specific, distinct cargo changes in a patient undergoing lung transplant diagnosed with mixed ACR/AMR compared with a matched analysis in 2 patients undergoing lung transplant without rejection. This case series introduces and supports further investigation of this platform. If validated, the B-cell sEV platform would constitute a novel noninvasive biomarker for AMR surveillance in lung transplantation, supplementing/minimizing the need for invasive, resource-intensive transbronchial biopsy and its associated complications. It would permit more frequent AMR monitoring via simple peripheral blood sampling, thus directly influencing long-term care of patients undergoing lung transplant.
Conflict of Interest Statement
The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Berry A.I.Hachem R.R.Antibody-mediated rejection after lung transplantation Ann Transl Med 8620204113235585510.21037/atm.2019.11.86PMC 7186640 · doi ↗ · pubmed ↗
- 2Habertheuer A.Ram C.Schmierer M.Circulating donor lung-specific exosome profiles enable noninvasive monitoring of acute rejection in a rodent orthotopic lung transplantation model Transplantation 106420227547663399318010.1097/TP.0000000000003820 · doi ↗ · pubmed ↗
- 3Habertheuer A.Chatterjee S.Japp A.S.Donor extracellular vesicle trafficking via the pleural space represents a novel pathway for allorecognition after lung transplantation Am J Transplant 2272022190919183528512710.1111/ajt.17023 · doi ↗ · pubmed ↗
- 4Korutla L.Hoffman L.R.Rostami S.Circulating T cell specific extracellular vesicle profiles in cardiac allograft acute cellular rejection Am J Transplant 24320244194353829500810.1016/j.ajt.2023.10.021PMC 12257922 · doi ↗ · pubmed ↗
- 5Welsh J.A.Goberdhan D.C.I.O’Driscoll L.Minimal information for studies of extracellular vesicles (MISEV 2023): from basic to advanced approaches J Extracell Vesicles 1352024 e 1245110.1002/jev 2.12404 PMC 1085002938326288 · doi ↗ · pubmed ↗
- 6Livak K.J.Schmittgen T.D.Analysis of relative gene expression data using real-time quantitative PCR and the 2−ΔΔCT method Methods 25420014024081184660910.1006/meth.2001.1262 · doi ↗ · pubmed ↗
- 7Heeger P.S.Haro M.C.Jordan S.Translating B cell immunology to the treatment of antibody-mediated allograft rejection Nat Rev Nephrol 2020242182323816866210.1038/s 41581-023-00791-0 · doi ↗ · pubmed ↗