Significance of the cribriform pattern in predicting the prognosis of lung adenocarcinoma patients: A systematic review and meta-analysis
Jun Peng, Xianquan Zhang, Yan Huang, Changhui Liu, Shuyang Li, Jinfeng Liu

TL;DR
This study finds that the cribriform pattern in lung adenocarcinoma is linked to worse survival and should be classified as a high-grade tumor subtype.
Contribution
The study establishes the cribriform pattern as an independent risk factor and proposes its classification as a high-grade histological subtype.
Findings
The cribriform pattern is associated with a hazard ratio of 2.05 for worse overall survival in lung adenocarcinoma patients.
Patients with cribriform pattern and positive air space spread have a significantly worse prognosis (HR: 2.58).
The cribriform pattern should be classified as a high-grade tumor subtype due to its impact on prognosis.
Abstract
A number of studies have shown that various histological subtypes of lung adenocarcinoma have different clinical prognoses, but the cribriform pattern, as a unique histological subtype, plays an important role in the prognosis of patients with lung adenocarcinoma. In this meta-analysis, we evaluated the role of the cribriform pattern in the overall survival of patients with lung adenocarcinoma, which may provide valuable information for the treatment of patients with lung adenocarcinoma. This also provides an important basis for dividing the cribriform pattern into a new histological subtype and classifying it. We searched the literature from the PubMed, Embase, Cochrane and Web of Science online databases; extracted the data and characteristics of each study; and extracted and calculated hazard ratios (HRs) with 95% confidence intervals (CIs) to evaluate the impact of the cribriform…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
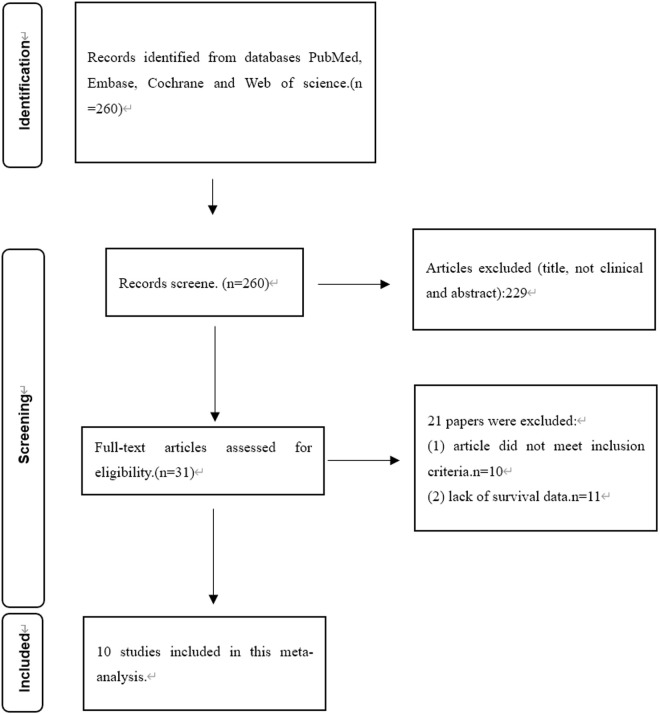 Fig 1
Fig 1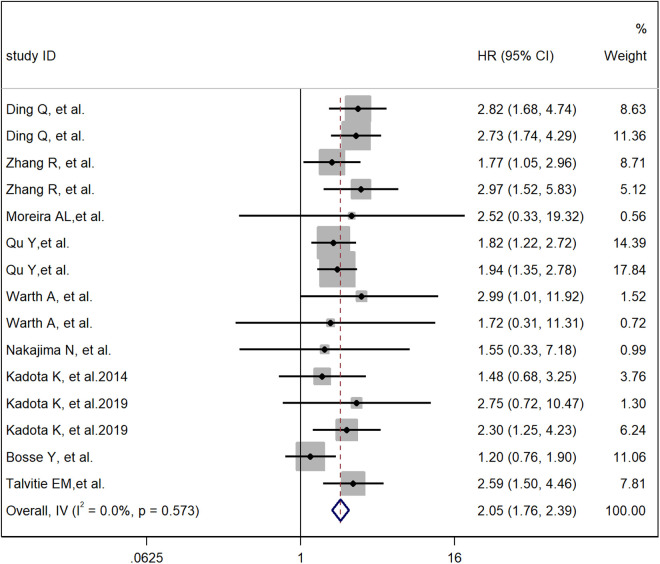 Fig 2
Fig 2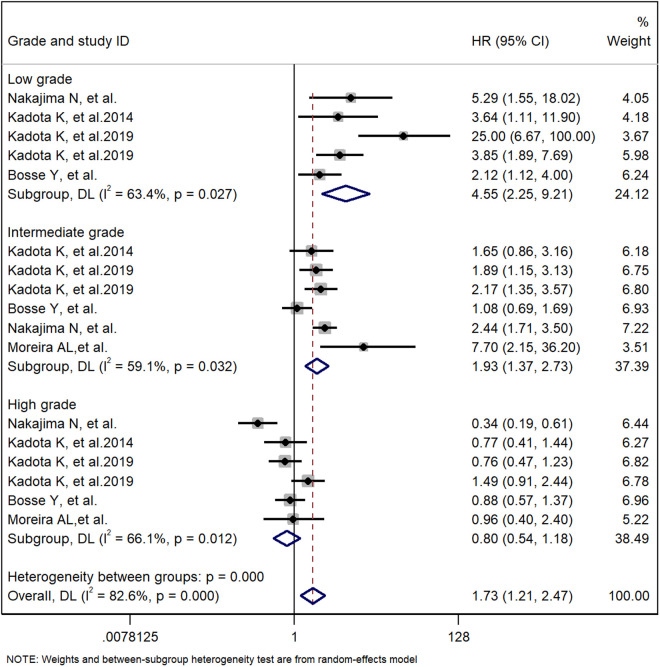 Fig 3
Fig 3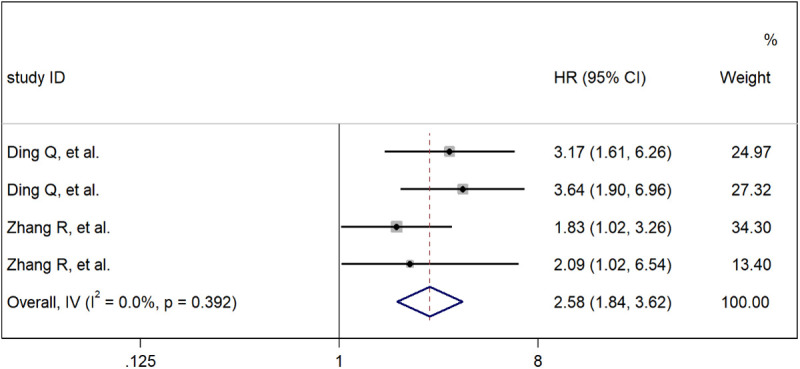 Fig 4
Fig 4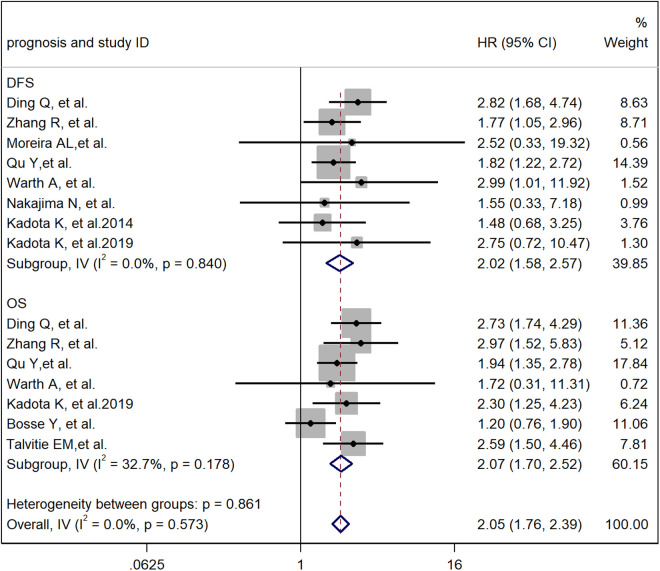 Fig 5
Fig 5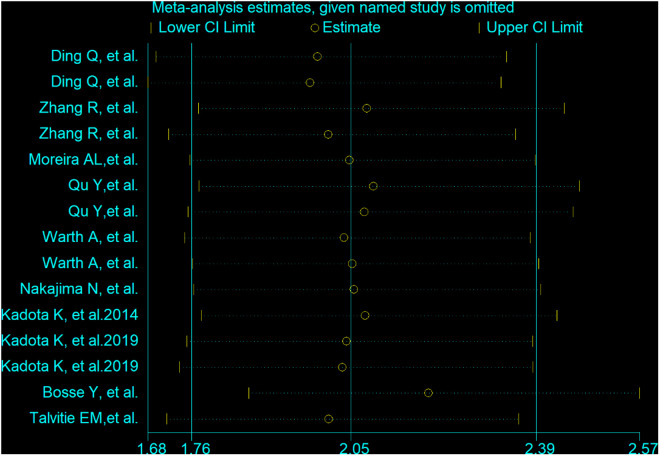 Fig 6
Fig 6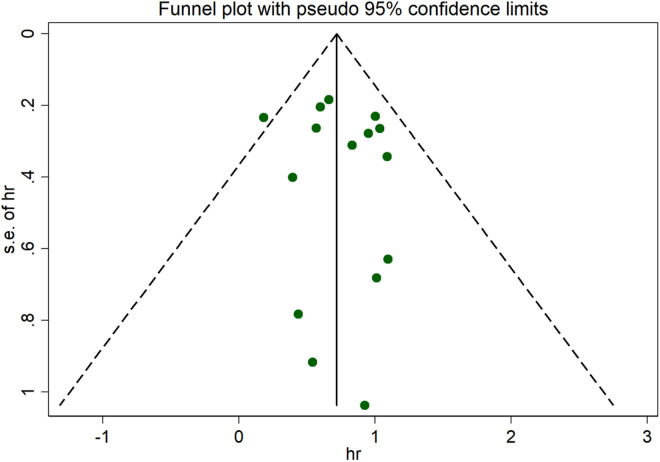 Fig 7
Fig 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Diagnosis and Treatment · Lung Cancer Treatments and Mutations · Radiomics and Machine Learning in Medical Imaging
Introduction
Lung cancer is the tumor with the highest mortality rate in the world [1], and lung adenocarcinoma (LUAD) is currently the most common histological subtype, accounting for 40% of all cases [2]. Lung adenocarcinomas are histologically heterogeneous [3] and are usually composed of a mixture of multiple growth modes. At present, when the World Health Organization (WHO) classifies lung cancer, most adenocarcinomas are mixed subtypes [4]. The International Association for the Study of Lung Cancer (IASLC), American Thoracic Society (ATS), and European Respiratory Society (ERS) [5] classify lung adenocarcinomas on the basis of their main patterns, including adenocarcinoma in situ, microinvasive adenocarcinoma, acinar, solid, micropapillary, papillary, and squamous pathological subtypes. Various histological subtypes of lung adenocarcinoma have different clinical prognoses [6]. There is a unique histological pattern called the cribriform pattern, which was included in lung adenocarcinoma by the World Health Organization (WHO) in 2015 [7]. The cribriform pattern is defined as invasive back-to-back fusion of tumor glands, poorly formed glandular spaces, lack of stroma, or invasive nests of tumor cells creating glandular cavities without solid components [8]. The main pathological subtypes of lung cancer are classified into low, intermediate, and high grades. The low grades include adenocarcinoma in situ, microinvasive adenocarcinoma and squamous, the intermediate grades include papillary and acinar, and the high grades include micropapillary and solid [4]. Most studies have shown that the prognosis of patients with the cribriform pattern is similar to that of patients with high-grade tumors. Therefore, we studied whether the cribriform pattern has an impact on the overall survival of patients with lung adenocarcinoma and whether the cribriform pattern should be considered a new histological subtype of lung adenocarcinoma.
Materials and methods
Search strategy
The studies were retrieved from the PubMed, Embase, Cochrane and Web of Science online databases by two reviewers. The following keywords were used to search for relevant studies: “cribriform” and “lung adenocarcinoma” or “pulmonary adenocarcinoma” and “prognostic”. The selected studies were published before September 2024. Two authors independently and manually screened the reference lists of the original articles for further relevant research.
Inclusion and exclusion criteria
The inclusion criteria for studies were as follows: (1) patients with lung adenocarcinoma were included as research subjects; (2) patients underwent surgical resection for therapeutic purposes; (3) the relationship between the cribriform pattern and the overall survival rate of patients with lung adenocarcinoma was studied; and (4) they study type was a randomized controlled trial (RCT) or an observational study. The exclusion criteria for studies were as follows: (1) included tissues or materials from animals rather than from humans; (2) research subjects had a history of other malignant tumors; (3) research subjects had undergone preoperative adjuvant chemoradiotherapy; (4) survival results were not reported or could not be calculated; and (5) overviews, seminar papers, reviews, reports, letters and duplicate publications.
Data extraction and quality assessment
Two reviewers independently screened the detected studies, and any disagreements were discussed and resolved with a third reviewer. Based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement, we extracted the following data: first author’s name, publication year, country and region, number of study subjects, follow-up time (basic unit: months), HR, 95% CI, overall survival (OS) and recurrence-free survival (DFS) (Table 1). For some HRs and 95% CIs that were not reported in the literature, we used Engauge Digitizer 11.1 to read the relevant data from the Kaplan‒Meier curve and then estimated the HR and 95% CI. When univariate and multivariate analyses were performed simultaneously, we selected the latter as a more precise treatment of the results.
Table 1: Basic characteristics of the included studies.
Two reviewers independently assessed the quality of the selected studies using the guidelines of the Newcastle–Ottawa Quality Assessment Scale (NOS), with scores ranging from 0 to 9 for each study. The scoring method includes three parts: selection (0–4 points), comparability (0–2 points) and result evaluation (0–3 points). Studies with NOS scores ≥6 were considered to be of high quality (Table 2) .
Table 2: Newcastle–Ottawa quality assessment scale (NOS).
The protocol was registered on the PROSPERO website with the registration number CRD42024562637. The relevant registration information can be obtained from the following website: https://www.crd.york.ac.uk/prospero/#searchadvanced.
Statistical analysis
STATA 14.0 was used to conduct the meta-analysis. For unknown HRs, we obtained Kaplan‒Meier curves from the original literature by using the software Engauge Digitizer. Heterogeneity was assessed via Cochran’s Q test and Higgins’ I^2^ statistic. When I^2^ < 50% or p > 0.10, the heterogeneity was considered low, and the fixed effects model was adopted. When I^2^ > 50% or p < 0.10, heterogeneity was considered obvious. We first analyzed the random effects model. Publication bias was described by funnel plots and Egger’s and Begg’s bias tests.
Results
Characteristics of eligible studies and quality assessment
We searched for literature from PubMed, Embase, Cochrane, and Web of Science, and obtained a total of 260 papers. After screening for title, abstract and type of study, 229 articles were excluded based on the established criteria. We then conducted a full review of the remaining 31 articles, of which 10 were eligible for meta-analysis The results of the subgroup analysis are shown in Table 3. In a flow chart of the study selection process (Fig 1), we summarized the main features of the 10 included studies.
Table 3: Results of the subgroup analysis.
Flow diagram for retrieving eligible articles.
Meta-analysis
A meta-analysis method was used to study the impact of the cribriform pattern on the prognosis of lung adenocarcinoma patients. We selected a cribriform component with more than 5% identity in pathological tissues as a sieve-like pattern, and the HR of the relationship between the cribriform pattern and the overall survival rate of lung adenocarcinoma patients was 2.05 (95% CI: 1.76–2.39) (Fig 2). These findings suggest that LUAD with a cribriform component is an independent risk factor for poor prognosis. Through observation, we found that there was a significant correlation between the cribriform pattern subtype and low- and intermediate-grade tumors but no significant correlation with high-grade tumors. The pooled HRs were 2.12 (95% CI: 1.12–4.00), 7.70 (95% CI: 2.15–36.20) and 0.96 (95% CI: 0.54–2.40) (Fig 2). These findings suggest that the cribriform pattern subtype should be considered a new histological subtype of lung adenocarcinoma and classified as a high-grade tumor. In the cribriform pattern, there is a significant correlation between STAS positivity and STAS negativity in the prognosis of lung adenocarcinoma patients. Therefore, STAS positivity in the cribriform pattern is an independent risk factor for a worse prognosis in lung adenocarcinoma patients. We have analyzed all the articles in the study and analyzed the staging of lung adenocarcinoma. A total of 5487 patients were enrolled, of which 3769 were in stage I, accounting for 68.7%. This indicates that cribriform patterns are an independent factor contributing to poor prognosis in early lung adenocarcinoma patients.
Meta-analysis of total HRs based on the cribriform pattern.
The cribriform pattern should be used as a histological subtype of high-grade tumors to influence the postoperative prognosis of patients with lung adenocarcinoma
The main pathological subtypes of lung cancer are classified into low, intermediate, and high grades. The low grades include adenocarcinoma in situ, microinvasive adenocarcinoma and squamous, the intermediate grades include papillary and acinar, and the high grades include micropapillary and solid [4]. In our meta-analysis, we compared the prognostic relationships between the cribriform pattern and low-grade, intermediate-grade, and high-grade tumors in patients with lung adenocarcinoma and obtained pooled HRs of 2.12 (95% CI: 1.12–4.00), 7.70 (95% CI: 2.15–36.20) and 0.96 (95% CI: 0.54–2.40), respectively (Fig 3). These findings indicate that there is a clear correlation between the cribriform pattern subtype and low- and intermediate-grade tumors and that the cribriform pattern subtype has a worse prognosis than lower- to intermediate-grade tumors do. There was no significant association with high-grade tumors, suggesting that both the cribriform pattern subtype and high-grade tumors have similar prognoses for patients with lung adenocarcinoma. Therefore, the cribriform pattern subtype should be regarded as a new histological subtype of lung adenocarcinoma and classified into high-grade tumors together with solid carcinoma and micropapillary adenocarcinoma.
Meta-analysis of subtotal HRs based on the grade of lung adenocarcinoma.
Patients with STAS-positive lung adenocarcinoma in the cribriform pattern have a worse prognosis
In our meta-analysis, we further compared the prognostic impact of STAS positivity versus that of STAS negativity in patients with lung adenocarcinoma in the cribriform pattern. Our results clearly indicate a significant correlation between STAS positivity and STAS negativity in the screening pattern and the prognosis of lung adenocarcinoma patients, with a combined HR of 2.58 (95% CI: 1.84–3.62; Fig 4). Therefore, this may indicate that STAS positivity in the cribriform pattern is an independent risk factor for a worse prognosis in patients with lung adenocarcinoma. The presence of cribriform components and a positive status should be considered synergistic prognostic factors for LUAD.
Meta-analysis of subtotal HRs based on STAS.
Effect of the cribriform pattern on OS and DFS in patients with lung adenocarcinoma after surgery
In some studies [9], the cribriform pattern was shown to be an independent risk factor for postoperative DFS and OS in patients with lung adenocarcinoma, but other studies have denied this view [13]. In our meta-analysis, we combined these studies and compared the relationships between the cribriform pattern and DFS and OS after surgery in patients with lung adenocarcinoma. The results clearly revealed a significant correlation between the cribriform pattern and DFS, with a combined HR of 2.02 (95% CI: 1.58–2.57; Fig 5), and there was a significant correlation between the cribriform pattern and OS, with a combined HR of 2.11 (95% CI: 1.64–2.71; Fig 5). Therefore, we believe that the cribriform pattern can serve as an independent risk factor for postoperative DFS and OS in patients with lung adenocarcinoma.
Meta-analysis of subtotal HRs based on the OS and DFS of LUAD patients.
Sensitivity analysis and Publication bias
In the comprehensive meta-analysis, sensitivity analysis checks were performed to explore the sources of heterogeneity (Fig 6). Regardless of whether the fixed effects model or the random effects model was used, the results were similar. We used Begg’s funnel plot and Egger’s linear regression test to test for publication bias. Egger’s test revealed that there was no significant publication bias in this study (p > 0.05). The shape of the funnel plot was visually symmetrical, with no evidence of publication bias (Fig 7).
Sensitivity analysis chart.
Funnel plot.
Discussion
Currently, the impact of the cribriform pattern on the survival of patients with lung adenocarcinoma has been widely studied worldwide [8,18,19]. We summarized the latest progress in the research on the cribriform pattern in patients with lung adenocarcinoma in recent years, focusing on the impact of the cribriform pattern on the postoperative prognosis of patients with lung adenocarcinoma and the fact that the cribriform pattern should be regarded as a new tissue subtype and classified as a high-grade tumor type with a poor prognosis.
In this meta-analysis, we found that the cribriform pattern was closely associated with poor prognosis in patients with lung adenocarcinoma after surgery. The cribriform pattern was an independent risk factor for prognosis after surgery for lung adenocarcinoma. In addition, when the cribriform pattern was compared with low-grade, intermediate-grade, and high-grade tumors, the combined HRs were 2.12 (95% CI: 1.12–4.00), 7.70 (95% CI: 2.15–36.20), and 0.96 (95% CI: 0.54–2.40), respectively. These findings indicate that there is a significant correlation between the cribriform pattern subtype and low- and intermediate-grade tumors but that there is no significant correlation with high-grade tumors. Therefore, the cribriform pattern subtype should be considered a new histological subtype of lung adenocarcinoma and classified as a high-grade tumor along with solid carcinoma and micropapillary adenocarcinoma, which is consistent with the conclusion of the study by Q. Ding et al. [9]. In addition, we determined that there was a significant correlation between STAS positivity and STAS negativity in the cribriform pattern with respect to the prognosis of patients with lung adenocarcinoma, with a combined HR of 2.58 (95% CI: 1.84–3.62). These findings suggest that STAS positivity in the cribriform pattern is an independent risk factor for poor prognosis in patients with lung adenocarcinoma, that STAS may affect the survival of patients with adenocarcinoma with cribriform components, and that the presence of cribriform components and STAS positivity should be considered synergistic prognostic factors for LUAD. Comprehensive research clearly revealed a significant correlation between the cribriform pattern and DFS and OS, with combined HRs of 2.02 (95% CI: 1.58–2.57) and 2.11 (95% CI: 1.64–2.71), respectively. Therefore, we believe that the cribriform pattern can serve as an independent risk factor for postoperative DFS and OS in patients with lung adenocarcinoma. We can see from the figure that heterogeneity was found among the studies. We explored heterogeneity by omitting each individual study and repooling the HRs of the remaining studies, and we found that no specific study affected the overall HR. Subgroup analyses were performed, and the results presented different HRs and heterogeneity among subgroups, which may explain the source of heterogeneity in the meta-analysis. In addition, there may be no significant difference in the length of follow-up of patients (as shown in the figure). This observation may be attributed to the fact that some patients with lung adenocarcinoma have a high degree of malignancy or are already in the advanced stage when they are examined, and their survival time is relatively short; however, this is also the value of our study.
This meta-analysis is the first to investigate the effect of the cribriform pattern on the overall survival of patients after surgery for lung adenocarcinoma and to investigate whether the cribriform pattern should be considered a new histological subtype of lung adenocarcinoma and should be classified as a high-grade tumor together with solid carcinoma and micropapillary adenocarcinoma. These findings provide a prognostic basis for patients with lung adenocarcinoma with a cribriform pattern and a new treatment direction for patients with lung adenocarcinoma after surgery, providing a basis [4] for many therapeutic advances through accurate diagnosis and molecular and biomarker testing that promote molecular targeting and immunotherapy [20,21]. In addition, the cribriform pattern should be considered a new histological subtype of lung adenocarcinoma in the future and should be classified as a high-grade tumor together with solid carcinoma and micropapillary adenocarcinoma.
Although our analysis revealed that the cribriform pattern plays an important role in the prognosis of patients with lung adenocarcinoma in predicting the final outcome, several shortcomings remain. First, owing to the small number of articles and research subjects included in this meta-analysis, when more standard-design studies are performed in the future, the cribriform pattern subtype will be regarded as a new histological subtype of lung adenocarcinoma and will be classified as a high-grade tumor together with solid carcinoma and micropapillary adenocarcinoma. This conclusion will eventually be confirmed. Second, this study revealed significant heterogeneity in demographics, methods of determining the presence of the cribriform pattern in patients with lung adenocarcinoma, and measurements and adjustments for confounders. Although we used appropriate meta-analysis techniques with a random effects model, we were unable to explain this difference, but sensitivity analyses revealed that the risk estimates were reliable across various quality factors. Third, some HRs could not be obtained directly from the articles. We estimated HRs from Kaplan‒Meier curves via Engauge Digitizer version 11.1, which may reduce the reliability of our results.
Conclusion
In conclusion, this meta-analysis demonstrated that LUAD with a cribriform component was an independent risk factor for poor prognosis. The cribriform pattern subtype should be considered a new histological subtype of lung adenocarcinoma and classified as a high-grade tumor. A positive STAS status in the cribriform pattern is an independent risk factor for poor prognosis in patients with lung adenocarcinoma, and the presence of cribriform components and positive STAS status should be considered synergistic prognostic factors for LUAD. The cribriform pattern can serve as an independent risk factor for postoperative DFS and OS in patients with lung adenocarcinoma. The above conclusions need additional research to enhance their persuasiveness.
Supporting information
S1 FilePRISMA checklist.(DOCX)
S2 FileAll retrieved articles.(XLSX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Li Y, Yan B, He S. Advances and challenges in the treatment of lung cancer. Biomed Pharmacother. 2023;169:115891. doi: 10.1016/j.biopha.2023.115891 37979378 · doi ↗ · pubmed ↗
- 2Naranjo S, Cabana CM, La Fave LM, Romero R, Shanahan S-L, Bhutkar A, et al. Modeling diverse genetic subtypes of lung adenocarcinoma with a next-generation alveolar type 2 organoid platform. Genes Dev. 2022;36(15–16):936–49. doi: 10.1101/gad.349659.122 36175034 PMC 9575694 · doi ↗ · pubmed ↗
- 3Soltis AR, Bateman NW, Liu J, Nguyen T, Franks TJ, Zhang X, et al. Proteogenomic analysis of lung adenocarcinoma reveals tumor heterogeneity, survival determinants, and therapeutically relevant pathways. Cell Rep Med. 2022;3(11):100819. doi: 10.1016/j.xcrm.2022.100819 36384096 PMC 9729884 · doi ↗ · pubmed ↗
- 4Nicholson AG, Tsao MS, Beasley MB, Borczuk AC, Brambilla E, Cooper WA, et al. The 2021 WHO classification of lung tumors: impact of advances since 2015. J Thorac Oncol. 2022;17(3):362–87. doi: 10.1016/j.jtho.2021.11.003 34808341 · doi ↗ · pubmed ↗
- 5Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011;6(2):244–85. doi: 10.1097/JTO.0b 013e 318206 a 221 21252716 PMC 4513953 · doi ↗ · pubmed ↗
- 6Xie L, Kong H, Yu J, Sun M, Lu S, Zhang Y, et al. Spatial transcriptomics reveals heterogeneity of histological subtypes between lepidic and acinar lung adenocarcinoma. Clin Transl Med. 2024;14(2):e 1573. doi: 10.1002/ctm 2.1573 38318637 PMC 10844893 · doi ↗ · pubmed ↗
- 7Travis WD, Brambilla E, Nicholson AG, Yatabe Y, Austin JHM, Beasley MB, et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J Thorac Oncol. 2015;10(9):1243–60. doi: 10.1097/JTO.0000000000000630 26291008 · doi ↗ · pubmed ↗
- 8Zhang R, Hu G, Qiu J, Wu H, Fu W, Feng Y, et al. Clinical significance of the cribriform pattern in invasive adenocarcinoma of the lung. J Clin Pathol. 2019;72(10):682–8. doi: 10.1136/jclinpath-2019-205883 31253654 · doi ↗ · pubmed ↗