Acute Respiratory Distress Syndrome and Spondylitis Secondary to Salmonella Bacteremia
Shonosuke Tajima, Satoshi Katsura, Yugo Nakata, Taro Okumura, Shiori Jinnno, Keiko Narumiya, Michio Shigematu

TL;DR
A healthy man developed severe respiratory and spinal complications from a Salmonella infection, which is rare and highlights unusual disease progression.
Contribution
This case report documents the rare co-occurrence of ARDS and spondylitis in a healthy adult with non-typhoidal Salmonella bacteremia.
Findings
Non-typhoidal Salmonella infection led to ARDS and spondylitis in a previously healthy adult.
Respiratory failure improved rapidly with antibiotics, while spondylitis required prolonged treatment.
The case suggests possible mechanisms for ARDS development in Salmonella infections.
Abstract
Salmonella enterica subsp. enterica includes both typhoidal and non-typhoidal serovars. The former are more likely to cause systemic infections such as typhoid fever, while the latter typically result in localized gastroenteritis. The main symptoms of non-typhoidal Salmonella (NTS)infection are transient diarrhea, which typically resolves within approximately five days. However, in a few cases, it may worsen and cause multiorgan dysfunction. A 39-year-old healthy male developed an NTS infection, which likely manifested as enteritis, followed by Salmonella bacteremia, spondylitis, and acute respiratory failure. The patient required mechanical ventilatory support due to rapidly progressive respiratory failure; however, the respiratory condition improved within a short period following antibiotic therapy. Subsequently, prolonged antibiotic treatment was administered for spondylitis.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
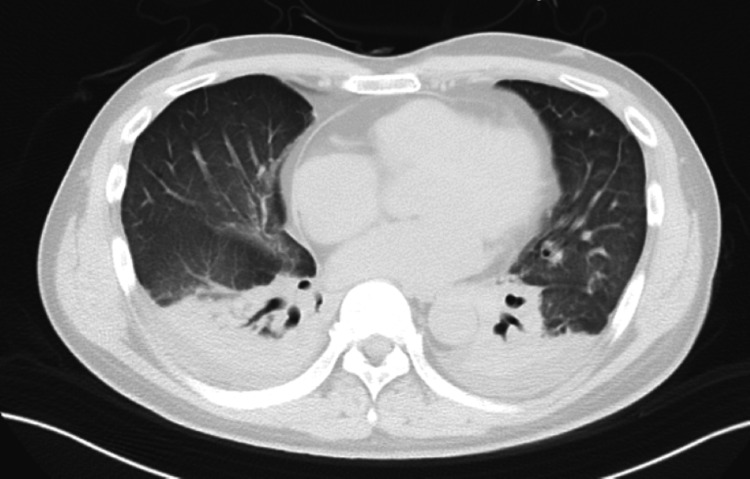 Figure 1
Figure 1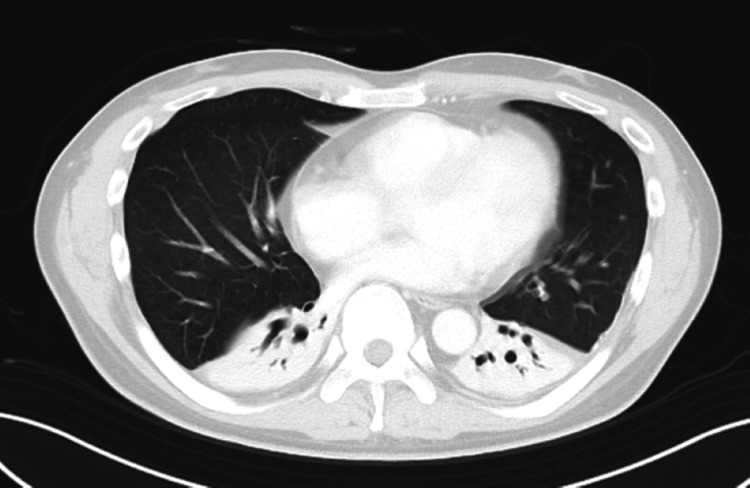 Figure 2
Figure 2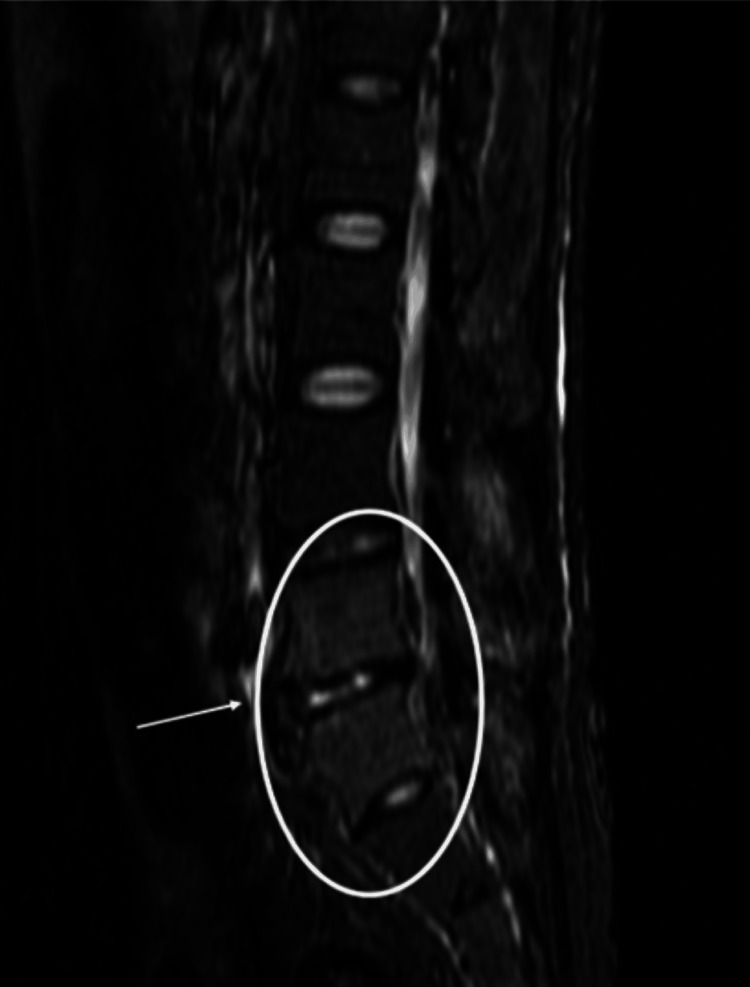 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Orthopedic Infections and Treatments · Bacterial Infections and Vaccines
Introduction
Salmonella enterica is a Gram-negative, facultative anaerobic bacillus belonging to the family Enterobacteriaceae. It includes typhoid strains, such as S. Typhi and S. Paratyphi A, as well as non-typhoidal Salmonella (NTS). S. Typhi and S. Paratyphi A cause typhoid and paratyphoid fever, respectively, and most cases of those diseases are accompanied by bacteremia. In contrast, gastrointestinal infections caused by NTS often resolve spontaneously in healthy adults and can occasionally progress to severe disease with multiple organ dysfunction, accompanied by bacteremia [1]. While pulmonary and skeletal manifestations associated with Salmonella bacteremia are well-documented, cases complicated by both acute respiratory distress syndrome (ARDS) and vertebral osteomyelitis remain exceedingly rare [2]. This case represents a rare instance of NTS bacteremia complicated by both ARDS and pyogenic spondylitis. The pathogenesis of ARDS in this report may involve a cytokine storm triggered by Salmonella infection. Additionally, the development of pyogenic spondylitis is presumed to result from hematogenous spread secondary to bacteremia [3].
Case presentation
A 39-year-old male truck worker developed frequent diarrhea and vomiting six weeks before admission to our hospital. At a local clinic, he was diagnosed with enteritis likely caused by raw eggs and shellfish consumed a few days earlier. Three weeks before admission, the diarrhea and vomiting recurred but resolved spontaneously. Two weeks later, he began experiencing fever (up to 38.3℃) and low back pain, which he attributed to his job.
Four days before referral, the back pain worsened, and despite taking analgesics, it did not improve, and he had difficulty moving. He visited the clinic, and a chest X-ray revealed infiltrates in both lung fields, and he was diagnosed as having pneumonia and hospitalized. MRI of the lumbar spine, performed to investigate the cause of the back pain, did not show any significant bone abnormality. Ceftriaxone was administered for pneumonia, but fever and elevated inflammatory markers persisted.
On the referral day, a follow-up chest and abdominal CT scan showed deterioration, and the patient was transferred to our hospital. Elevated C-reactive protein, procalcitonin, and D-dimer levels were shown. Biochemical results showed mildly elevated liver and biliary enzymes. HIV antibodies were negative. At the time of admission, arterial blood gas analysis showed 9.7 kPa with a nasal cannula at 5 L/min, indicating hypoxemic respiratory failure.
Chest X-ray showed diffuse ground-glass opacities in both lung fields. Chest CT revealed bilateral pleural effusion, thickening of the bronchovascular bundles, diffuse ground-glass opacities, and infiltrates surrounding the bronchovascular structures (Figure 1). Transthoracic echocardiography showed no wall motion abnormalities or valvular vegetations. Contrast-enhanced chest and abdominal CT did not reveal findings suggestive of pulmonary embolism, aortic dissection, or intra-abdominal hemorrhage.
Chest CT on admissionAxial chest CT image of a patient with ARDS secondary to Salmonella septicemia. The image reveals bilateral ground-glass opacities and patchy consolidations, predominantly in the posterior and basal lung regions. Bilateral mild pleural effusions are also noted.CT: computed tomography, ARDS: acute respiratory distress syndrome
The patient exhibited fever, tachycardia, tachypnea, and leukocytosis, fulfilling the criteria for systemic inflammatory response syndrome. Although septicemia due to bacterial infection was suspected, the referring physician had already administered ceftriaxone, and it was considered that the lung lesions might be caused by pathogens other than typical bacteria commonly associated with pneumonia. Legionellosis and chlamydia infections were cited as a differential diagnosis, and levofloxacin therapy was initiated.
The possibility of rapidly progressive interstitial lung disease associated with connective tissue disease was also considered, and a variety of autoantibodies were tested. However, follow-up results did not show significant elevations. On the second day of hospitalization, even with a 6 L/min oxygen mask, the PaO₂ was 7.5 kPa. Chest X-ray showed worsening reticular shadows in both lung fields. A follow-up chest CT revealed further progression of ground-glass opacities, bilateral pleural effusion, and dense infiltrates mostly confined to the dependent zones of bilateral lower lobes.
Given the worsening respiratory status, mechanical ventilation was initiated. Considering the possibility of worsening rapidly progressive interstitial lung disease, therapy with methylprednisolone 1000 mg/day was administered, and antibiotics were switched to piperacillin-tazobactam. A bronchoalveolar lavage revealed an increased neutrophil fraction (total cells: 7.40 × 10⁵/mL; neutrophils: 59%, lymphocytes: 12%, eosinophils: 0%, macrophages: 29%; CD4/CD8 ratio: 0.56). No bacteria were cultured from the lavage fluid, and the Gomori methenamine silver stain was negative.
On the third day, Salmonella O7 group (Salmonella Montevideo) was identified from blood cultures taken by the referring hospital. The patient was diagnosed with ARDS due to Salmonella bacteremia. Regarding the back pain, spondylitis associated with Salmonella bacteremia was considered highly likely. Since the causative bacteria were sensitive to ceftriaxone, the antibiotics were switched back to ceftriaxone.
Fever, inflammatory response, and respiratory status improved, and extubation was performed on the fifth day of referral. Oxygen therapy was discontinued on day 9 after transfer. A follow-up chest CT taken on the same day showed mild atelectasis and pleural changes in both lungs, but the ground-glass opacities and infiltrates significantly improved (Figure 2). The patient continued to improve, with no further deterioration in respiratory status or back pain. The patient was discharged on day 47 after transfer.
Chest CT on the ninth sick dayFollow-up axial chest CT image on day 9 in a patient with ARDS secondary to Salmonella septicemia. The image reveals near-complete resolution of the previous bilateral ground-glass opacities, with preservation of normal bronchovascular markings. There is persistent atelectasis or homogeneous opacities with air bronchograms extending internally in the bilateral dependent zones. Pleural effusions have completely resolved. This radiological improvement is consistent with clinical recovery.CT: computed tomography, ARDS: acute respiratory distress syndrome
Initially, it was difficult to explain pneumonia and back pain as a single entity. However, once bacteremia was identified, Salmonella infection-associated pyogenic spondylitis or reactive spondylitis was considered. It is noted that in cases of pyogenic spondylitis, MRI findings within two weeks of onset may not be obvious, so a re-evaluation of the lumbar spine MRI was performed on day 9 of hospitalization.
At that point, high signal areas were observed in the intervertebral spaces between L4 and S1 (L5 is congenitally absent) on STIR imaging (Figure 3). A biopsy was performed at the same site on day 17, but no bacteria were detected. Considering that more than two weeks had passed since the initiation of antibiotic treatment, and given the patient's young age and high vertebral bone density, it is believed that sufficient tissue could not be obtained with a needle biopsy.
MRI of the lumbar regionCoronal STIR MRI of the lumbar spine on day 9 of hospitalization. High signal intensity is observed around the intervertebral spaces between L4 and S1 (the circled area in the image), suggesting inflammatory changes consistent with early-stage pyogenic or reactive spondylitis. The L5 vertebral body is congenitally absent. These findings prompted CT-guided biopsy on day 17.STIR: short tau inversion recovery, MRI: magnetic resonance imaging, CT: computed tomography
At the time of admission, the patient complained of back pain so severe that they were unable to change positions. However, after approximately two months of antibiotic treatment, the back pain improved. MRI imaging showed that the high signal areas in the intervertebral discs on short tau inversion recovery (STIR) imaging had disappeared or reduced in size. However, the high signal in the vertebral bodies remained (Figure 4). Differentiating between pyogenic spondylitis and reactive spondylitis was difficult.
Post-treatment lumbar MRIFollow-up lumbar spine MRI after antimicrobial therapy for pyogenic spondylitis. Compared to the initial study, STIR images show a marked decrease in high signal intensity at the L4–S1 intervertebral spaces (the circled area in the image), indicating resolution of bone marrow edema. T1-weighted images demonstrate partial normalization of signal intensity in the L4 vertebral body, and contrast-enhanced fat-suppressed T1-weighted images show reduced enhancement at the L4–S1 endplates and adjacent soft tissue, consistent with decreased inflammatory activity.MRI: magnetic resonance imaging, STIR: short tau inversion recovery
However, after the completion of antibiotic therapy, sulfasalazine was added, and the back pain symptoms further improved. This suggests the possible involvement of reactive spondylitis. The antimicrobial therapy was initially administered via intravenous infusion for four weeks, followed by a switch to oral levofloxacin, which was continued for an additional six weeks to treat the spondylitis.
Discussion
Salmonella infection
Salmonella enterica is a Gram-negative, facultative anaerobic bacillus belonging to the family Enterobacteriaceae. It includes typhoidal Salmonella, such as S. Typhi and S. Paratyphi, as well as NTS. S. Typhi and S. Paratyphi cause typhoid and paratyphoid fever, respectively, and present as bacteremia in most instances. In contrast, gastrointestinal infections caused by NTS are relatively rarely accompanied by bacteremia. NTS species are well-known causes of foodborne illness in humans. Infections are commonly acquired through the consumption of raw or undercooked meat and eggs. NTS infections primarily cause acute gastroenteritis, which typically resolves within approximately five days without antibiotic treatment. In a few cases, following the resolution of initial gastrointestinal symptoms, Salmonella is thought to persist in anatomical sites such as the mesenteric lymph nodes, intestinal epithelium, reticuloendothelial organs, and the gallbladder, from which it may subsequently lead to hematogenous dissemination. Individuals with underlying conditions such as immunodeficiency, malignancy, AIDS, or sickle cell disease, as well as infants and the elderly, are at increased risk for progression to severe disease, including bacteremia. The incidence of bacteremia in pediatric patients has been reported to range from 10% to 20%, while the overall incidence across all age groups is approximately 8.8%. Furthermore, approximately 25% of Salmonella bacteremia cases are associated with focal infections, including osteomyelitis and spondylitis [4,5].
ARDS due to Salmonella bacteremia
Both typhoid and NTS infections rarely cause ARDS. In this case, ARDS is believed to have developed in the context of NTS bacteremia. ARDS caused by sepsis occurs when bacteria or bacterial-derived endotoxins and cytokines reach the lungs via the bloodstream, increasing vascular permeability [6]. This leads to the accumulation of exudate in the alveoli and a decrease in surfactant production, resulting in impaired ventilation and consequent pulmonary dysfunction. Reports exist of patients who survived ARDS due to NTS infections following steroid pulse therapy [7], suggesting that steroids may have contributed to symptom improvement in this case as well. When ARDS progresses, it can lead to diffuse alveolar damage (DAD), a pathological condition with a mortality rate of 35-50%. Furthermore, previous studies have reported that DAD, the hallmark histopathological finding of ARDS, is observed in approximately 56% of surgical lung biopsy specimens [8] and 45% of autopsy specimens [9] from patients diagnosed with ARDS. These findings suggest that while DAD is a common pathological correlate of ARDS, it is not universally present in all cases, possibly reflecting heterogeneity in the underlying lung injury patterns and the timing of tissue sampling. The variable presence of DAD underscores the complexity of ARDS as a clinical syndrome with diverse pathological substrates. By day 9 of hospitalization, the chest CT showed significant improvement in the diffuse ground-glass opacities and infiltrates confined to the dependent zones of both lungs, and the respiratory condition also rapidly improved. Therefore, it is considered that DAD did not develop in this patient.
Spondylitis due to Salmonella bacteremia
The causative pathogen of pyogenic spondylitis is most commonly Staphylococcus aureus (60-90%), followed by Escherichia coli, Pseudomonas aeruginosa, and fungi. Salmonella is responsible for less than 1% of cases [10]. Pyogenic spondylitis caused by Salmonella is often associated with underlying conditions, such as connective tissue diseases, malignancies, or sickle cell disease [11]. In contrast, reactive spondylitis is more frequently observed following infections with pathogens such as Salmonella or Campylobacter. There have been reports of pyogenic spondylitis or reactive spondylitis following Salmonella bacteremia, with approximately 25% of cases of Salmonella bacteremia leading to localized foci of infection, such as osteomyelitis or spondylitis [1].
Antibiotic treatment for Salmonella bacteremia
The general recommended duration of antibiotic treatment for Salmonella bacteremia is 14 days, but when complicated by osteomyelitis, intravenous antibiotics are required for more than four weeks [12]. Antibiotic therapy was continued until the back pain symptoms resolved. In this case, ceftriaxone was administered until day 28 (counted from the referring physician’s initial treatment), after which it was switched to oral levofloxacin. Even after the switch to oral medication, no worsening of the respiratory status or upper airway symptoms was observed, and the inflammatory response did not escalate.
Conclusions
We encountered a rare case of NTS bacteremia complicated by acute respiratory failure and spondylitis. Although the patient developed ARDS and required mechanical ventilation, their condition improved rapidly, and they recovered without any lasting sequelae. While spondylitis associated with Salmonella bacteremia is uncommon, it should be considered when patients present with constant back pain.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A severe case of non typhoidal salmonella associated with multiple organ damage- case study and literature review Georgian Med News Bansal R Zhamutashvili M Gognadze T Dolmazishvili E Jojua N 981022024 https://pubmed.ncbi.nlm.nih.gov/38963211/38963211 · pubmed ↗
- 2Salmonella bacteremia: a case with miliary lung lesions and spondylitis Radiology GRRH FESB 8608626819571344191310.1148/68.6.860 · doi ↗ · pubmed ↗
- 3Clinical manifestations of salmonellosis in man; an evaluation of 7779 human infections identified at the New York Salmonella Center N Engl J Med SAI WIJW 1128113425619571345200610.1056/NEJM 195706132562402 · doi ↗ · pubmed ↗
- 4Manual of Clinical Microbiology 13th Edition Salmonella 759Hoboken (NJ)Wiley 7462023 https://www.wiley.com/en-us/Manual+of+Clinical+Microbiology%2C+4+Volume+Set%2C+13th+Edition-p-9781683674290
- 5Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases 5th Edition Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 27252736 Philadelphia (PA)Churchill Livingstone 2232000
- 6Clinical presentation of extraintestinal infections caused by non-typhoid Salmonella serotypes among patients at the University Hospital in Cracow during an 7-year period Pol J Microbiol Kedzierska J Piatkowska-Jakubas B Kedzierska A 4147572008 https://pubmed.ncbi.nlm.nih.gov/18610655/18610655 · pubmed ↗
- 7Salmonella panama and acute respiratory distress syndrome in a traveler taking a proton pump inhibitor J Travel Med Heysell SK Thomas TA Morrison AR Barry M 4604631520081909080410.1111/j.1708-8305.2008.00258.x · doi ↗ · pubmed ↗
- 8Acute respiratory distress syndrome: advances in diagnosis and treatment JAMA Fan E Brodie D Slutsky AS 69871031920182946659610.1001/jama.2017.21907 · doi ↗ · pubmed ↗