Elective Caesarean Delivery in a Patient With May-Hegglin Anomaly: Its Concerns and Review of the Literature
Yuki Julius Ng, Jin Yun Lee, Callie Foo, Wei Kang Lee

TL;DR
A woman with May-Hegglin anomaly safely delivered via caesarean section, and most pregnancies with this condition have normal outcomes.
Contribution
A review of 96 pregnancies with May-Hegglin anomaly reveals delivery safety and minimal complications.
Findings
85.4% of pregnancies with May-Hegglin anomaly had uneventful deliveries.
Only one case of postpartum hemorrhage was possibly linked to May-Hegglin anomaly.
Most infants delivered from mothers with May-Hegglin anomaly had no complications.
Abstract
May-Hegglin anomaly (MHA) is an autosomal dominant haematological disorder that is commonly misdiagnosed as idiopathic thrombocytopenic purpura. The presence of leukocyte inclusion bodies differentiates it from other causes of thrombocytopenia. There is a lack of agreement on the perioperative management of patients with MHA. Our patient was a 33-year-old lady with underlying MHA, gravida 2 para 1 at 37 weeks of pregnancy, who was electively admitted for lower-segment caesarean section under general anaesthesia. The caesarean delivery was uneventful, and the mother and baby were discharged without any complications from the operation. In this patient, an intra-abdominal drain was inserted to drain any postoperative intra-abdominal bleeding; however, the drain produced minimal haemoserous drainage, which was similarly observed in her first pregnancy. We performed a systematic search of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
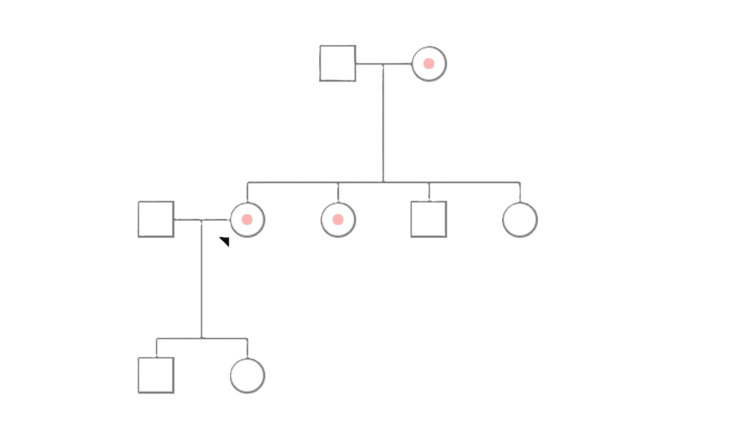 Figure 1
Figure 1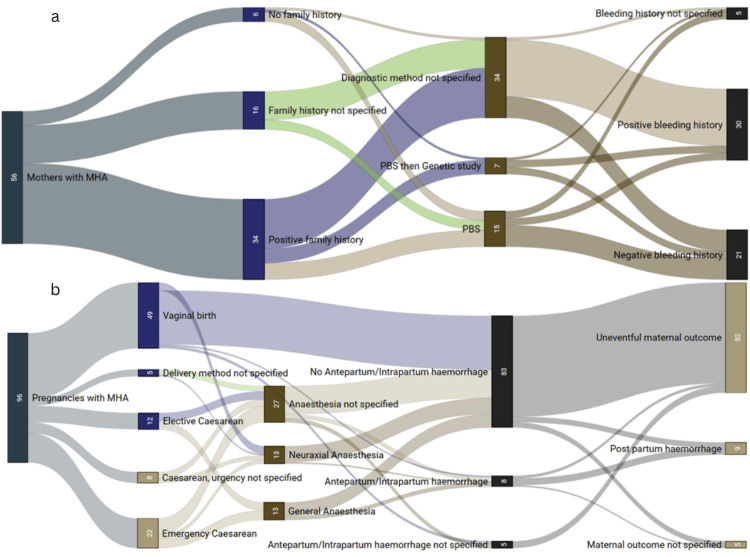 Figure 2
Figure 2| Blood parameters | Result | References |
| Haemoglobin | 164 | 130 - 170 g/L |
| White cells | 6.9 | 4.0 - 11.0 x10^9/L |
| Platelets | 56 | 150 - 400 x10^9/L |
| Prothrombin time | 9.8 | 10 - 13.2 s |
| International normalised ratio | 0.87 | 0.8 - 1.2 |
| Activated partial thromboplastin time | 23.8 | 25.1 - 36.5 s |
| Total bilirubin | 5 | <21 umol/L |
| Alkaline phosphatase | 32 | 30 - 130 U/L |
| Alanine aminotransferase | 40 | 10 - 60 U/L |
| Sodium | 138 | 133 - 146 mmol/L |
| Potassium | 4.2 | 3.5 - 5.3 mmol/L |
| Urea | 3 | 2.5 - 7.8 mmol/L |
| Creatinine | 60 | 59 - 104 umol/L |
| Estimated glomerular filtration rate (eGFR) | >90 | >90 ml/min |
| Author, year published | Number of pregnancies in the paper | Background | Country (paper published) | Ethnicity | Age | Family history of MHA | G/P/M (M = miscarriage) | Methods of diagnosis | Time of diagnosis (e.g., 10 gestational weeks) | Age of diagnosis with MHA | Bleeding history prior to pregnancy | Management plan | Mode of delivery | If operated, the mode of anaesthesia | Platelets prior to delivery | PT | aPTT | INR | Bleeding time | Platelet transfusion | Bleeding complication (maternal) | Other complications (maternal) | Estimated blood loss (ml) | Fetal complications | Fetal outcome | Maternal outcome |
| Takashima et al. (1992) [ | 1 | No history of bleeding, underwent appendicectomy at 15 and was uneventful. Diagnosed as ITP at 23 after p/w URTI and treatment with 50 mg prednisone/day | Japan | Japanese | 26 | Unknown | Primigravidarum | PBS | 17+2 weeks of gestation | 26 | No bleeding tendency | None | SVD | - | 35,000 | Not specified | Not specified | Not specified | Not specified | No | No | Uneventful | Not specified | Uneventful, MHA + in utero following cordocentesis | Uneventful | Uneventful |
| Muzannar et al. (2017) [ | 3 | Initially diagnosed with ITP, treated with steroids, multiple platelet transfusions, and 4 cycles of rituximab. Initially, ITP was unresponsive to treatment, and splenectomy was done with minimal blood loss | Saudi Arabia | Not specified | Not specified | Yes | G5P3M2 | PBS, bone marrow biopsy | After 2nd pregnancy | Not specified | No bleeding tendency | 1: platelet 18 units and cryo 6 units + IVIG. 2: 6 units of platelets, IVIG, and prednisolone. 3: 6 units of platelets | 1: LSCS. 2: SVD. 3: LSCS | 1: GA. 3: Epidural | 1:22,000. 2: 7,000. 3: 13,000 | Normal | Normal | Normal | Normal | Yes | 1: No. 3: Not specified | Uneventful | Not specified | Not specified | Not specified | Uneventful |
| Magann et al. (1999) [ | 1 | Initially misdiagnosed as ITP, treated with steroids and IVIG | United States of America | Not specified | 28 | Unknown | Primigravidarum | PBS | Not specified | 28 | No bleeding tendency | 6 units of platelets | LSCS | GA | 29,000 | Not specified | Not specified | Not specified | Not specified | Yes | No | Uneventful | Not specified | Ambiguous genitalia, fetal growth restriction, MHA | Uneventful | Uneventful |
| Guruparan et al. (2021) [ | 1 | - | Sri Lanka | Sri Lankan | 29 | Yes | Primigravidarum | PBS | Not specified | 24, following family screening | No bleeding tendency | 6 units of platelets prior to operation | LSCS | SA | 30,000 | Not specified | Not specified | Not specified | Not specified | Yes | No | Uneventful | Not specified | Uneventful | Uneventful | Uneventful |
| Nelson et al. (1993) [ | 2 | - | United States | Caucasian | 31 | Unknown | 1: G3P0M2. 2: G4P1M2 | Not specified | Prior 3rd pregnancy | Not known | History of 2 miscarriage during the 1st trimester of 1st and 2nd pregnancy | No medication was given to the mother. The patient underwent elective LSCS under GA in view of the risk of fetal thrombocytopenia | 1: LSCS. 2: LSCS | 1: GA. 2: GA | 1: 84,000. 2: 80,000 | Not specified | Not specified | Not specified | Not specified | No | No | Uneventful | 1: 600. 2: Not specified | 1: MHA (+). 2: Uneventful | Uneventful | Uneventful |
| Kotelko (1989) [ | 1 | P/w at 41 weeks with ROM. Observed for 24 hours, and a trial of labour was offered with induction of labour and augmentation, but failed. | United States of America | Not specified | 31 | Unknown | Primigravidarum | Not specified | Prior to pregnancy | Not Known | No bleeding tendency, even during tooth extraction | 6 units of type-specific platelets, 100% O2 FM, IVI 1500 ml lactated Ringer's, spinal anaesthesia with 5% lidocaine with 1:200,000 epinephrine & 0.5 mg morphine sulphate. Emergent LSCS due to failed IOL | LSCS | SA | 24,000 | Normal | Normal | Normal | Normal | No | Yes | Uneventful | 700 | MHA (+) | Uneventful, male, alive. platelet count of 41,000 | PPH secondary vaginal tear |
| Fishman et al. (2009) [ | 7 (3 mothers) | Incidental finding on a blood test on one of the family members. 3 sisters with MHA on anaesthesia during delivery | United States of America | Not specified | Not specified | Yes | Para 3 | Not specified | Prior to pregnancy | Not specified | No bleeding tendency | Not specified | 1: SVD. 2: SVD. 3: SVD | 1: Epidural. 2: Epidural. 3: Epidural | 1: 100,000. 2: 47,000. 3: 26,000 | Normal | Normal | Normal | Normal | No | No | Uneventful | Not specified | Not specified | Uneventful, MHA+, one neonate had 35 platelet count | Uneventful |
| United States of America | Not specified | Not specified | Yes | Para 2 | Not specified | Prior to pregnancy | Not specified | No bleeding tendency | Not specified | 1: SVD. 2: SVD | 1: Epidural. 2: Epidural | 1: 48,000. 2: 26,000 | Normal | Normal | Normal | Normal | No | No | Uneventful | Not specified | Not specified | Uneventful | ||||
| United States of America | Not specified | Not specified | Yes | Para 2 | Not specified | Prior to pregnancy | Not specified | No bleeding tendency | Not specified | 1: LSCS. 2: LSCS | 1: SA. 2: SA | 1: 14,000. 2: 81,000 | Normal | Normal | Normal | Normal | No | No | Uneventful | Not specified | Not specified | Uneventful | ||||
| Amodeo et al. (2021) [ | Twin pregnancy | Monochorionic, diamniotic twins | Italy | Not specified | 32 | Unknown | Primigravidarum | PBS | Postpartum day 1 | 32 | No bleeding tendency | Emergent LSCS at 32+1 weeks due to altered umbilical and medial cerebral artery flowmetry of the second fetus | LSCS | Not specified | Not specified | Not specified | Not specified | Not specified | Not specified | No | No | IUGR of twin 1 and cerebral anomalies of both twins on ultrasound. Fetal MRI showed mild ventriculomegaly associated with a cyst in the velum interpositum | Not specified | Both twins are MHA (+) with mild ventriculomegaly and a cyst of the velum interpositum without evidence of obstruction of CSF circulation | Twin 1: Male, alive. Weight: 1490g. Platelet: 12,000. No bleeding complications. Twin 2: Male, alive. Weight: 2010 g. Platelet: 24,000. No bleeding complications | Uneventful |
| Landy et al. (1987) [ | 2 | 1st and 3rd pregnancy. 3rd pregnancy with antiplatelet antibody positive and placenta previa | United States of America | Caucasian | 17 (1st), 24 (3rd) | Yes | 1: Primigravida. 3: G3P1M1 | Not specified | After 1st pregnancy | 18 | No known bleeding history, bleeding after cervical cone biopsy | Not known (1st), HLA-matched platelet, but did not correct bleeding time, cryoprecipitate and steroids were also given. Emergent LSCS in view of placenta previa (3rd) | 1: SVD. 3: LSCS | 3: Not specified | 3: 22,000 | Not specified | Not specified | Not specified | Not specified | 1: No. 2: Cryoprecipitate. 3: No | 1: No. 2: No. 3: Heavy painless vaginal bleed postpartum | - | 1: No. 3: 1000 ml | 1. Uneventful. 3: MHA (+) | Uneventful | 1: PPH, transfused 8 pints of packed cells. 3: PPH, transfused platelets and cryoprecipitate |
| Pajor et al. (1999) [ | 1 | Chronic proliferative glomerulonephritis, initially misdiagnosed with ITP and treated with steroids and splenectomy | Hungary | Hungarian | 25 | Unknown | Para 2 | PBS | 10 years postpartum | 25 | Easy bruising prior to first pregnancy | 1: platelet concentrate. 2: not specified | 1: LSCS. 2: LSCS | Not specified | 1: 70,000. 2: 100,000 | Not specified | Not specified | Not specified | Not specified | 1: Yes. 2: Not specified | No | Uneventful | Not specified | Uneventful | Uneventful | Uneventful |
| Takabayashi et al. (2007) [ | 1 | Antiplatelet antibody (-) | Japan | Japanese | 26 | Unknown | Primigravidarum | Not specified | Not known | Not known | No bleeding tendency | Elective LSCS under GA | LSCS | GA | 49,000 | Not specified | Not specified | Not specified | Not specified | No | No | No | Not known | Not specified | Uneventful | Uneventful |
| Binder et al. (2003) [ | 2 | Initially misdiagnosed as ITP (minimal response to steroids); uneventful pregnancy course | Prague | Not specified | Not specified | Unknown | Not specified | Not specified | Routine antenatal blood test (wrong diagnosis) | Not known | Not specified | Corticosteroid administered, response was minimal | LSCS | GA | 34,000 | Not specified | Not specified | Not specified | Not specified | Yes | No | No | 400 ml | Uneventful | Uneventful | Uneventful |
| Initially misdiagnosed as ITP (minimal response to steroids ), developed signs of pre-eclampsia | Prague | Not specified | Not specified | Unknown | Not specified | Not specified | Routine antenatal blood test (wrong diagnosis) | Not known | Not specified | Trial of labour with induction of labour (unsuccessful). Subsequent LSCS. Corticosteroid administered, response was minimal | LSCS | GA | 27,000 | Not specified | Not specified | Not specified | Not specified | Yes | No | No | 700 ml | Uneventful | Uneventful | Uneventful | ||
| Kim et al. (2012) [ | 1 | No known medical illness | Korea | Korean | 39 | Yes | Primigravidarum | PBS, bone marrow biopsy, genetic study (MYH9) | 12 weeks of gestation | 39 | Not specified | Not specified | LSCS | Not specified | Not specified | Normal | Normal | Normal | Normal | Not specified | Not specified | Not specified | Not specified | Bilateral temporal cephalohematoma, MHA (+) | Uneventful | Uneventful |
| Urato et al. (1998) [ | 1 | P/w SROM and contraction | United States of America | Not specified | 31 | Yes | Primigravidarum | FBC | Prior pregnancy | 29 | No bleeding tendency, slight heavy periods for 4-5 days | Not specified | SVD | - | 16,000 | Not specified | Not specified | Not specified | Not specified | No | No | No | Not specified | Uneventful | Uneventful | Uneventful |
| Chatwani et al. (1992) [ | 1 | P/w spontaneous ROM at >39 weeks. Ultrasound showed no frank breech presentation of the fetus | United States of America | Caucasian | 28 | Unknown | G4P0M3 | Not specified | Prior pregnancy | Several years prior | Bleeding gums 1 week prior to admission. Otherwise, no bleeding tendency | 12 units of platelet transfusion prior to surgery | LSCS | Not specified | 34,000 | Not specified | Not specified | Not specified | Not specified | Yes | No | No | Not specified | MHA (-) | Uneventful | Uneventful |
| Chabane et al. (2001) [ | 3 | Developed PROM with fever and abnormal labour progress | France | French | 24 | Unknown | Para 3 | FBC/PBS | 24 weeks of gestation | 24 | No bleeding tendency | Platelet transfusion for the first pregnancy | 1: LSCS. 2: LSCS. 3: LSCS | Not specified | 1: 45,000. 2: Not specified. 3: 32,000 | Normal | Normal | Normal | Normal | 1: Yes. 2: No. 3: No | No | No | Not specified | 1: MHA (-). 2: MHA (-). 3: MHA (+) | Uneventful | Uneventful |
| Siddiqui et al. (1991) [ | 1 | Antiplatelet antibody (+); initially misdiagnosed as immune thrombocytopenia. Subsequently, not responsive to steroids, IVIG, and splenectomy | United States | Caucasian | 22 | Yes | Primigravidarum | Not specified | After the current pregnancy | Not known | No bleeding tendency | Emergent LSCS due to HELLP syndrome | LSCS | GA | 22,000 | Not specified | Not specified | Not specified | Not specified | No | Yes, intermittent vaginal bleeding | HELLP Syndrome | Not known | MHA (-) | Uneventful | Persistent thrombocytopenia despite plasmapheresis and continued steroids post delivery |
| Ishii et al. (1993) [ | 1 | - | Japan | Japanese | 25 | Yes | Primigravidarum | Routine antenatal blood test | During routine antenatal blood test follow-up | 25 | Not specified | Elective LSCS under GA due to the risk of fetal thrombocytopenia | LSCS | GA | 49,000 | Not specified | Not specified | Not specified | Not specified | Yes | No | No | 997 | MHA (-) | Uneventful | Uneventful |
| Kinsella et al. (1999) [ | 1 | Initially misdiagnosed as ITP (steroid and IVIG used for autoimmune thrombocytopenia). Antiplatelet antibody (-) | United States | Not specified | 28 | Yes | Primigravidarum | Routine antenatal blood test | Not known | 28 | No bleeding tendency | Elective LSCS due to the risk of fetal thrombocytopenia | LSCS | GA | 29,000 | Not specified | Not specified | Not specified | Not specified | Yes | Not specified | No | Not known | Intrauterine growth restriction with ambiguous genitalia. MHA (+) | Uneventful | Uneventful |
| Duff et al. (1985) [ | 1 | The patient had concurrent rhesus sensitisation | USA | Not specified | 23 | Yes | Primigravidarum | Not specified | Prior to the current pregnancy | 19 | Bleeding after tooth extraction | Platelet transfusion x2 and blood transfusion postoperation due to prolonged bleeding time. Elective LSCS due to uncertain risks of vaginal delivery and patient's choice | LSCS | SA | 67,000 | Not specified | Not specified | Not specified | Not specified | Yes | No | none | 1000 | MHA (+) | Uneventful | Oozing surgical site, transfused platelets |
| Fayyad et al. (2002) [ | 3 | Incidental finding of low platelet count (40) during 1st trimester of her first pregnancy. Platelet count ranged from 40 to 61 throughout her pregnancy | United Kingdom | Not specified | 25 | Unknown | Primigravidarum | PBS | During 1st trimester of her first pregnancy | 25 | No bleeding tendency | 1: Emergency LSCS at 36 weeks because of sudden severe proteinuric hypertension along with elevated liver enzymes. 2: Sudden cessation of fetal movements. Subsequent u/s showed IUD. 3: Patient had two-week assessments of fetal growth and weekly biophysical profile by ultrasound from 24 weeks onwards. Results were normal. Elective LSCS planned at 37 weeks | 1: LSCS. 2: SVD. 3. LSCS | Not stated | 1: 50,000. 2: 162,000. 3: 129,000 | Not specified | Not specified | Not specified | Not specified | No | No | None | 1: Average blood loss. 2. Not specified. 3: Average blood loss | 1: No complications. 2: Stillbirth (no thrombocytopenia). 3: No complications | 1: Uneventful. 2: Intrauterine fetal demise, macerated, female, weight: 3.4 kg. Placental changes suggest uteroplacental insufficiency caused fetal demise. 3: Uneventful | Uneventful |
| Tordjeman et al. (1996) [ | 1 | Diagnosed with MHA after a check-up due to an episode of acute abdominal pain | France | Not specified | 30 | Unknown | Primigravidarum | Not specified | Prior to pregnancy | 21 | Yes, easy bruising | Forceps vaginal delivery due to failure to progress | Forceps delivery | - | 54,000 | Not specified | Not specified | Not specified | Not specified | No | No | None | Not known | MHA (-) | Uneventful | Uneventful |
| Garcia-Horton et al. (2020) [ | 1 | - | Canada | Not specified | 29 | Yes | Not specified | PBS, genetic study | 8 weeks of gestation | 29 | No bleeding tendency | Yes | SVD | Epidural | 32,000 | Not specified | Not specified | Not specified | Not specified | Yes | No | No | Not known | MHA (-) | Uneventful | Uneventful |
| Favier et al. (2018) [ | 2 | Underwent appendectomy at 15 and received a platelet transfusion, but developed angioedema and anaphylaxis. Had p.Met1934 TrpfsX mutation in exon 40 of the MYH9 gene. ISTH bleeding score was 3 | France | Not specified | 41 | Unknown | Para 2 | Genetic study | Infancy | Infancy | Yes (epistaxis, minor wounds, and cutaneous) | 1: No special management. 2: eltrombopag 50 mg/day at 36 weeks of gestation and platelets at 30 | 1: LSCS. 2: LSCS | 1: GA. 2: SA | 1: 26,000. 2: 179,000 | Not specified | Not specified | Not specified | Not specified | No | 1: Uterine atony treated with sulprostone. 2: bleeding from the incision site after starting LMWH 12 hours after LSCS. No transfusion. Hb11.2 post surgery | no | Not specified | 1: MHA (+). 2: MHA (+) | Uneventful | Uneventful |
| Giordano et al. (2020) [ | 1 | Had deafness, macrothrombocytopenia, and bleeding episodes since childhood, MCDA twin pregnancy with CVI cyst diagnosed at 19 weeks of gestation via USG | Italy | Italian | 32 | Unknown | Not specified | Genetic study | Prior pregnancy | 30 | Yes (epistaxis and menorrhagia) | IV TXA 1 g given prior to GA | LSCS | GA | 16,000 | Not specified | Not specified | Not specified | Not specified | Yes | No | No | Not known | Twin 1: MHA (+), CVI cyst. Twin 2: MHA (+), CVI cyst | Uneventful | Uneventful |
| Conte et al. (2018) [ | 1 | Initially misdiagnosed as ITP during the first pregnancy, unresponsive to steroids and gamma globulin | Chile | Not specified | 51 | Yes | Para 2 | PBS, bone marrow biopsy, genetic study | Age 50 | 50 | No bleeding tendency | Not specified | 1: SVD. 2: Not specified | Not specified | - | Normal | Normal | Normal | Normal | Not specified | Not specified | Uneventful | Not specified | Not specified | Not specified | Uneventful |
| Chin et al. (2017) [ | 1 | Diagnosed with ITP at 5 years old; however, unresponsive to steroids with subsequent loss to follow-up. Peripheral blood smear at 24 weeks of gestation showed signs of MHA | Malaysia | Not specified | 26 | Yes, only known after a genetic study was done for the patient's family tree | Not specified | Genetic study | After the current pregnancy | 26 | No bleeding tendency | Spontaneous labour at 38 weeks with a platelet count of less than 10. Given platelet transfusion (unknown units) | SVD | - | <10,000 | Not specified | Not specified | Not specified | Not specified | Yes | No | None | 200 | Uneventful | Uneventful | Uneventful |
| Rosen et al. (1997) [ | 1 | She and her mother had AUB. 303 mg/dl --> 458 mg/dl fibrinogen level (N: 180-350) | Germany | German | 25 | No, but the mother was symptomatic | Primigravidarum | PBS, aggregometer | 11 weeks + 4 days | 25 | Yes, prolonged menstrual bleeding | ELLSCS at 38 + 4 weeks for breech and given DDAVP 8 amp postoperation | LSCS | Not stated | 26,000 | 117% -> 129% | Not mentioned | Not mentioned | More than 20 minutes | No | No | No | Not mentioned | Uneventful | Uneventful | Managed with 8 amp of DDAVP IV |
| Yamashita et al. (2016) [ | 1 | The patient had a low platelet count, and a subsequent peripheral blood smear in the 1st trimester demonstrated suspicion of MYH9 disorder. Pure tone audiometry showed bilateral sensorineural hearing loss, and she had underlying gestational diabetes mellitus treated with medico-nutritional therapy | Japan | Japanese | 35 | FH (mother and grandmother) of thrombocytopenia and difficulty hearing | Primigravidarum | PBS | After delivery | 35 | No bleeding tendency | Elective LSCS at 37 weeks in view of breech presentation | LSCS | GA | 60,000 | Not specified | Not specified | Not specified | Not specified | No | No | None | 867 ml | MHA (-) | Uneventful | Uneventful |
| Safiullina et al. (2022) [ | 3 | Menarche at 14, first pregnancy at the age of 34 | Russia | Russian | 34 | Yes | Not specified | PBS, genetic study | Prior pregnancy, there was an incidental finding of platelets at 50 | 29 | Yes, AUB, epistaxis, ecchymosis, and easy bruising. No episodes of bleeding/APH | ELLSCS at 38 weeks | LSCS | Not specified | Not specified | Not specified | Not specified | Not specified | Not specified | Yes | No | None | Not mentioned | MHA (+) | Uneventful | Uneventful |
| Menarche at 14, first noted bleeding tendencies at age 24 (petechiae and platelet count at 28). Treated with oral steroids, but no effect, so splenectomy was done with no effective outcomes | Russia | Russian | 36 | Yes | Not specified | PBS, genetic study | After pregnancy | 38 | Yes, petechiae at the lower extremities | ELLSCS at 28 weeks | LSCS | Not specified | Not specified | Not specified | Not specified | Not specified | Not specified | Ambiguous | Yes | None | Not mentioned | Uneventful | Uneventful | Uneventful | ||
| Born in 1959, menarche at age 14 | Russia | Russian | Not specified | Yes | Para 2 | Not specified | After pregnancy | 57 | Yes, heavy menstrual bleeding | Not specified | Not specified | Not specified | Not specified | Not specified | Not specified | Not specified | Not specified | No | No | No | Not mentioned | Uneventful | 1: Uneventful. 2: Uneventful | Uneventful | ||
| García Vallejo et al. (2014) [ | 1 | - | Mexico | Latina | 28 | No | Primigravidarum | PBS | During 3rd trimester | Discovered at 18 but confirmed at 28 | No bleeding tendency | Emergency LSCS at 39+5 weeks following failed IOL with prostin. Pain management: IV paracetamol 1 g every 6 hours & IV pethidine 25 mg every 4 hours alternating | LSCS | GA | 20,900 | Normal | Normal | Normal | Normal | No | No | No | 500 ml | Uneventful | Uneventful | Uneventful |
| Kumazawa et al. (2019) [ | 1 | Diagnosed with ITP at age 4, spontaneous conception and platelet count was 4x10^4 at 13+2 weeks | Japan | Japanese | 29 | Yes, family history of thrombocytopenia | Primigravidarum | PBS | 13+2 weeks | 29 | No bleeding tendency | IOL at 38+2 due to oligohydramnios (4.9 cm) | SVD | - | 134,000 | Not specified | 26.6 s | 1 | Not specified | No | No | No | 275 ml | MHA (+) | Uneventful | Uneventful |
| Gausis et al. (1969) [ | 2 | During week 28 of 2nd pregnancy, had vaginal bleeding and epistaxis | Italy | Caucasian | 32 | No | 1: primigravida. 2: G2P1 | PBS | During week 28 of 2nd pregnancy | 36 | Easy bruising, vaginal bleeding, epistaxis | 1: Not known. 2: Spontaneous vaginal delivery at 28 weeks | 1: Not specified. 2: SVD | Not specified | 1: 50,000. 2: 50,000 | Not specified | Not specified | Not specified | Not specified | No | 1: Frequent epistaxis. 2: Vaginal bleeding and extensive leg bruises | No | Not known | Uneventful | 1: Uneventful. 2: Stillborn, macerated dead baby | Uneventful |
| Budde et al. (1979) [ | 1 | Hematoma after breast operation | Germany | Not specified | 21 | Unknown | Primigravidarum | Not specified | Prior to the current pregnancy | Not known | Postoperative bleeding | Not specified | SVD | - | 30,000 | Not specified | Not specified | Not specified | Not specified | No | No | No | Average | Uneventful | Uneventful | Uneventful |
| Bettaieb et al. (1991) [ | 2 | 1: Negative antiplatelet antibody. 2: Positive antiplatelet antibody, history of prior twice miscarriages | France | Not specified | Not specified | Yes | 1: G1P0M2. 2: G2P1M2 | Not specified | Prior to 1st pregnancy (1st week of life) | Not known | Epistaxis, menorrhagia, easy bruising, twice miscarriages | 1: 3 times platelet transfusion. 2: 3 times platelet transfusion and IVIG used to prevent neonatal alloimmune thrombocytopenia. Elective LSCS due to the risk of fetal thrombocytopenia | 1: LSCS. 2: LSCS | Not specified | 1: 10,000. 2: Not specified | Not specified | Not specified | Not specified | Not specified | No | No | History of prior twice miscarriages | Not known | 1: Uneventful. 2: MHA (+) | 1: Uneventful. 2: Uneventful | Uneventful |
| Turnquest et al. (1994) [ | 2 | Initially misdiagnosed as ITP and thrombocytopenia unresponsive to steroids, IVIG, and splenectomy | United States | Not specified | 19 | Yes | Primigravidarum | Routine antenatal blood test | During the antenatal check-up in 1st pregnancy | 19 | Gum and nose bleeding | 1: Cordocentesis at 38 weeks. 2: Cordocentesis at 37 weeks | 1: LSCS. 2: LSCS | Not specified | 1: 82,000. 2: 37,000 | Not specified | Not specified | Not specified | Not specified | Not specified | No | 1: Non-reassuring fetal tracing. 2: Footling breech presentation after spontaneous rupture of membranes | Not known | 1: Uneventful. 2: Uneventful | 1: Uneventful. 2: Uneventful | Uneventful |
| Kumi et al. (1999) [ | 1 | Diagnosed at 5-6 years old during a routine check-up | Japan | Japanese | 21 | Unknown | Primigravidarum | Not specified | Prior to pregnancy | 6 | Menorrhagia | Not specified | Forceps-assisted delivery | - | 80,000 | Not specified | Not specified | Not specified | Not specified | No | No | Prolonged fetal bradycardia | 780 | MHA (-) | Uneventful | Uneventful |
| Scurlock et al. (2005) [ | 1 | Twins | United States | Not specified | 28 | Yes | Primigravidarum | Not specified | Not known | Not known | No bleeding tendency | Not specified | SVD | - | Not specified | Not specified | Not specified | Not specified | Not specified | No | No | No | Not known | Twin 1: MHA (+). Twin 2: MHA (+) | Twin 1: Uneventful. Twin 2: Uneventful | Uneventful |
| Filanovsky et al. (2009) [ | 1 | - | Israel | Not specified | 24 | Unknown | Primigravidarum | Routine antenatal blood test | During the current pregnancy | 24 | No bleeding tendency | Not specified | Not specified | Not specified | 21,000 | Not specified | Not specified | Not specified | Not specified | Not specified | No | Not known | Not known | Not known | Not known | Not known |
| Bizzaro et al. (1999) [ | 33 (4 twin births) | Data were obtained from one large family | United States of America | Italian | 21-83 | Yes | Not specified | Not specified | Prior pregnancy | Not specified | No bleeding tendency | Not specified | 30 SVD (4 twins) and 3 LSCS | Not specified | 87,000 | Not specified | Not specified | Not specified | Not specified | No | No | No | Not specified | Uneventful | 20 affected with MHA out of 37, with a platelet range of 48-115. Another 7 cases where the father had the anomaly, they were delivered vaginally without complications | Uneventful |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSexual Differentiation and Disorders · Urological Disorders and Treatments · Prenatal Screening and Diagnostics
Introduction
May-Hegglin anomaly (MHA) is a rare, autosomal dominant inherited haematological disorder characterised by the presence of giant platelets, inclusion bodies in granulocytes, and thrombocytopenia [1-4]. MHA can be misdiagnosed as idiopathic thrombocytopenic purpura (ITP) and treated with ineffective treatments, such as corticosteroids and splenectomy [4]. The definitive diagnosis of MHA is limited to those with leukocytic inclusion bodies, due to aggregates of abnormal non-muscle myosin heavy chain and no other organ dysfunction [2]. The presence of these inclusion bodies in leukocytes but not platelets differentiates MHA from other causes of thrombocytopenia, such as ITP [2]. Despite its recognition as a genetic disorder associated with a specific gene mutation, there is still a lack of consensus on the optimal perioperative management for patients with MHA undergoing surgery. We describe a patient diagnosed with MHA who underwent an elective lower-segment caesarean section under general anaesthesia with prophylactic platelet transfusion and tranexamic acid before induction. We also performed a systematic search and review of the literature to discuss clinical aspects of the findings in terms of obstetric, anaesthesia, and paediatric concerns. This case was written according to the CARE (Case Report) guidelines.
Case presentation
We report a case of a 33-year-old pregnant woman, gravida 2 para 1, at 37 weeks of amenorrhea, electively admitted to our hospital for lower-segment caesarean section, in view of an underlying MHA. Antenatally, she had a previous history of caesarean section done for her first pregnancy; her postoperative outcome was uneventful, with an intraoperative drain showing minimal drainage with an estimated blood loss of 500 ml intraoperatively. Throughout both of her pregnancies, she did not have any antenatal or antepartum haemorrhage. Before admission, she did not have any spontaneous bleeding, easy bruising, petechiae, gum, nasal, or mucosal bleeds, or any previous requirement for transfusion. Her bleeding stopped well (compared with her peers) in the past from minor trauma and injury. She was otherwise not in labour, and had irregular tightening and good fetal movement. Her cervix was closed, and she had zero contractions in 10 minutes. Her bedside antenatal scans were corresponding to date, and the cardiotocograph was reassuring.
A multidisciplinary team meeting between obstetrics, haematology, anaesthesiology, and paediatrics was carried out to keep each team updated and ready for delivery. The obstetrics team led the discussion and brought the other team together to discuss the best method of delivery and a proper plan with anticipation. The pathophysiology and the bleeding risk were explained and stratified by the haematology team and further discussed with anaesthesiology to provide the lowest risk possible. The paediatrics team were informed of the method of delivery and its potential risk to the newborn child.
Delivery outcome
The patient underwent a lower-segment caesarean section under general anaesthesia. Intraoperatively, four units of platelets and 1 g of tranexamic acid were given before skin incision. The operation was uneventful, with an estimated blood loss of 500 ml. The baby was born cephalic, with clear liquor. An intra-abdominal drain was inserted. Postoperative vaginal examination showed no blood clots upon evacuation, and there were no bruises seen over the postoperative site. The lochia loss was reduced on day two postoperatively. The intra-abdominal drain produced minimal haemoserous content and was taken out after two days postoperatively (this was also previously performed for her first pregnancy).
Fetal outcome
Her baby boy was born with an Apgar score of 5 at one minute, 9 at five minutes, and 10 at 10 minutes. Post delivery, her baby required two cycles of positive pressure ventilation and was admitted to the nursery for close monitoring. Birth weight was 2.84 kg. After admission, the baby was able to oxygenate; however, he remained in the nursery for phototherapy for neonatal jaundice secondary to G6PD. The baby’s platelet count was 345k/uL.
Her previous baby girl was born flat, requiring intubation, likely due to the general anaesthesia. The baby girl is currently well and healthy; however, the patient reported that the doctors mentioned the baby girl has low platelets and is likely to have MHA. After her first pregnancy, her thrombocytopenia was investigated, and since then her family has been screened for MHA (Figure 1). Blood investigations of the patient are presented in Table 1.
Pedigree of the patient’s family who is affected by MHA.Arrowhead: our patient. Dotted figure: May-Hegglin anomaly (MHA).
Her prothrombin time was 9.8 seconds, international normalised ratio was 0.87, and activated partial thromboplastin time was 23.8 seconds. Her platelet trend was as follows: 63k/uL - 58k/uL - four units of platelets transfusion - 56k/uL - 90k/uL (postoperation) - 81k/uL. Her previous preoperative platelet trend was as follows: 44k/uL - 57k/uL (postoperation) - 52k/uL.
Peripheral blood film (PBF) showed evidence of low platelets at 47k/uL during her first pregnancy. There was the presence of basophilic cytoplasmic inclusion bodies seen in neutrophils resembling Döhle bodies. Her platelets were mildly reduced (26-33/HPF), with no platelet clumps or fibrin seen, but the presence of large and giant platelets was noted, which were suggestive of MHA.
Follow-up
She was under haematology and obstetrics clinic follow-up. In both visits, the patient reported no signs of haemorrhage during and after puerperium and did not require any intervention. However, she underwent close monitoring under the haematology team every month for the past six months to catch any bleeding tendencies from the operation. The patient had an otherwise uneventful pregnancy.
Discussion
MHA is an autosomal dominant giant platelet disorder characterised by abnormally large platelets with defective leucocytes and thrombocytopenia [3]. A literature search was conducted using PubMed, MEDLINE, Embase, CENTRAL, Global Health, Global Index Medicus, Scopus, Canadian Agency for Drugs and Technologies in Health (CADTH), Networked Digital Library of Theses and Dissertations (NDLTD), Public Affairs Information Service (PAIS), bioRxiv, Google Scholar, and Google search. Our search strategy was “May Hegglin anomaly” AND “pregnancy”. We included all languages, case reports, case series, and cohort studies that included primary data analysis. Articles in languages other than English were translated to English with a visual multilingual neural machine tool for further interpretation and data extraction. We utilised articles that analysed secondary data to further our search for published literature. A total of 100 articles were found after removing repeated titles, but only 40 were selected. Clinical data were extracted from these articles, which concern obstetrics, anaesthesia, and paediatric concerns where possible. There were 96 reported pregnancies by 56 mothers, which are collated and summarised (Figure 2, panel a).
Panel a: Proportion of mothers with family history, methods of diagnosis of MHA, and their previous history. Panel b: Proportion of number of pregnancies, mode of delivery, anaesthesia, and maternal outcomes.MHA: May-Hegglin anomaly; PBS: peripheral blood smear.
The preferred method of diagnosis for MHA is a genetic study for the MYH9 gene, present on chromosome 22q12-2A, due to its rarity; however, a thorough evaluation with peripheral blood smear (PBS) is recommended in those with a positive family history of bleeding diathesis. Among the 56 mothers, 26.8% (n = 15) were diagnosed with PBS, 60.7% (n = 34) were unspecified, and 12.5% (n = 7) were diagnosed with PBS and confirmed with genetic studies. Among 56 mothers, 60.7% (n = 34) had a positive family history, 10.7% (n = 6) had a negative family history, and 28.6% (n = 15) had an unspecified family history. The majority of mothers (53.6%, n = 30) had a positive bleeding history, 37.5% (n = 21) did not have a bleeding history, and 8.9% (n = 6) of the reported mothers did not specify a bleeding history. Curiously, 60% (n = 9) of those who were diagnosed with PBS had a negative bleeding history. However, 80% (n = 24) of those who had positive bleeds did not specify the diagnostic method of MHA. But for those who were confirmed with PBS, 20% (n = 3) had a history of bleeding, which is still a considerably high proportion from the pooled population. Of those who had a positive family history of MHA, 61.8% (n = 21) of mothers were not reported with the method of diagnosis. The common misdiagnosis is ITP due to its similarities in clinical presentation; hence, genetic testing should be done to confirm the diagnosis.
In our literature review (Table 2), there were a total of 96 pregnancies and the majority (51%, n = 49) were via vaginal delivery, followed closely by lower-segment caesarean section (LSCS) at 43.8% (n = 42), and 5.2% (n = 5) of deliveries were unspecified. Of those pregnancies that were delivered via caesarean section, 52.4% (n = 22) were emergency deliveries, 28.6% (n = 12) were elective, and 11.9% (n = 5) were unspecified. A total of 64.3% (n = 27) of those who required caesarean section did not report the mode of anaesthesia, 31% (n = 13) were done under general anaesthesia, and 14.3% (n = 6) were done under neuraxial anaesthesia. Epidural analgesia was given to three mothers who gave birth via six vaginal deliveries. The majority of pregnancies (86.5%, n = 83) did not have any antepartum or intrapartum haemorrhage, only 8.3% (n = 8) experienced either antepartum or intrapartum haemorrhage, and the rest were not specified. Among those who did not have a history of antepartum or intrapartum haemorrhage, only 4.8% (n = 4) resulted in postpartum haemorrhage, and the other five pregnancies that had postpartum haemorrhage were from those mothers who had a history of antepartum or intrapartum bleeding. Postnatally, the majority of mothers had an uneventful recovery at 85.4% (n = 82) whilst only 9.7% (n = 9) developed postpartum haemorrhage. Four of them were treated with blood products, and 5.2% (n = 5) were unspecified. Among the nine mothers with postpartum haemorrhage, we only attributed one patient with bleeding potentially from MHA from a surgical site oozing. The rest had other risk factors such as placenta praevia (n = 1), HELLP (haemolysis, elevated liver enzymes, and low platelets) syndrome (n = 1), uterine atony (n = 2), and unspecified(n = 4). The descriptive data of this review suggest a possible reassurance of uneventful pregnancies; however, those with a history of bleeding have a potentially increased risk of postpartum haemorrhage. This suggests that individuals affected by MHA may have an increased risk of bleeding, which was seen in other cases [4]. To properly stratify the risk of bleeding and its clinical implications, more studies with higher levels of evidence and proper data collection should be performed. Given the rarity of this disease, it would be more feasible for a multicentre prospective study to observe risks and possible guidelines to guide future clinicians further (Figure 2, panel b).
Anaesthesia concerns
It is reassuring that all patients who underwent neuraxial anaesthesia in our literature search did not experience epidural-spinal haematoma. One of the case series performed neuraxial anaesthesia for seven patients with MHA who underwent vaginal deliveries and caesarean sections [10]. In our search, only 9.7% had postpartum haemorrhage, and none of them experienced spinal haematoma. According to the review of the documented literature, which spans over 54 years, technology in diagnostics and care in general has improved for obstetric patients, and the rate of postpartum haemorrhage is likely lower than the finding in this current case study.
There is no consensus for an absolute lower platelet count limit that grants safety for neuraxial anaesthesia. "The literature is insufficient to assess whether a routine platelet count can predict anaesthesia-related complications in uncomplicated parturients" [43]. Within the guideline, 77% of anaesthetists strongly agreed and 21.3% agreed that ordering platelets should be individualised and based on patient history, physical examination, and clinical signs [43]. This is also shown in our literature search, showing that mothers with underlying MHA but otherwise an uncomplicated pregnancy usually have an uneventful pregnancy and delivery. However, mothers with MHA with an added issue of placenta previa, HELLP syndrome, or preeclampsia, for example, have a tendency to experience postpartum haemorrhage (Figure 2). A thromboelastography (TEG) could also be a valuable analysis of MHA, which may guide clinicians in assessing haemostasis. A case report that analysed the TEG of preterm twins showed normal or slightly reduced platelet function despite low platelet counts (12-28 × 103 per mm^3^) [11]. The use of TEG is, however, discretionary as literature is scarce with respect to patients with MHA. To properly understand the nature of platelets in this regard requires further research.
Obstetrics concerns
Prophylactic platelet transfusion prior to delivery to reduce the risk of postpartum haemorrhage is discretionary. There were isolated postpartum haemorrhage cases, such as uterine atony and uterine inversion, which resolved without platelet transfusion [10,27,34]. The majority of patients underwent vaginal delivery, including instrument-assisted delivery, and most had uneventful outcomes. However, instrumental delivery remains a relative contraindication for patients with thrombocytopenia and should be used with caution to prevent complications such as cephalohematoma or intraventricular haemorrhage.
MHA is a rare cause of thrombocytopenia in pregnancy. It is often detected with a complete blood count, followed by a PBS due to its availability, cost-effectiveness, and interpretability, but it carries a risk of misdiagnosis as ITP [44,45]. We found 14 mothers who were misdiagnosed with ITP and were unresponsive to steroids, intravenous immunoglobulins, and splenectomy [13,15,28,29]. None of the literature reported the use of intra-abdominal drains to detect intra-abdominal bleeding and therefore may not be useful in cases of MHA. A multidisciplinary approach between the obstetrics, anaesthesia, paediatrics, and haematology teams should be carried out to plan for the anticipated delivery. Although PBS as a form of diagnosis is widely accepted, its sensitivity and specificity have never been described or observed. Understanding this may potentially reduce the misdiagnosis of ITP and reduce unnecessary surgery and expensive medication.
Paediatric concerns
Amongst the 103 infants delivered, 85.4% (n = 88) had no associated complications at birth, and 7.8% (n = 8) of infants had complications at birth. These complications were intrauterine fetal demise, bilateral temporal cephalohematoma, intracranial cyst, and ambiguous genitalia. There were two cases of intrauterine fetal demise from two separate mothers, where one was reported to have uteroplacental insufficiency as the cause, and the second case did not discuss the cause. Only one case of spontaneous bilateral temporal cephalohematoma was reported, and this baby was delivered via caesarean section. There were no further complications. In the peripartum period, 95.3% (n = 41) of infants with MHA reported no bleeding tendencies, even in infants who had instrument-assisted delivery or circumcision. This can raise an argument that, in spite of the low platelet count, the risk of bleeding is minimal. It was theorised that the absence of bleeding may be explained by the normality of platelet function guaranteed by a total mass of giant platelets equivalent to that of a normal subject [4]. Most studies suggest that individuals with MHA are asymptomatic, tests of platelet function and aggregation are typically normal, and platelet defects responsible for excessive bleeding have not been defined [2].
Limitations
Some mothers have multiple pregnancies, which may skew the data presentation. Not all data were captured in each case, and most of the articles were of low-quality evidence, which may not be ideal for describing the risks and best practices. With the interest in treating this population of patients, a global multicentre data-capturing method should be employed to further understand the clinical implications of MHA and how to approach MHA in pregnancy.
Conclusions
MHA is a rare disease that needs a multidisciplinary approach to plan for safe delivery in obstetric patients. The literature suggests that mothers with MHA generally have an uneventful delivery via all methods. Children who were delivered did not have any complications pertaining to MHA. In terms of anaesthetics, all types of anaesthetic methods seem to be safe without direct complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Organization for Rare Disorders. May Hegglin anomaly 5 2025 403404 Philadelphia, PA Lippincott Williams & Wilkins 2008 https://rarediseases.org/rare-diseases/may-hegglin-anomaly
- 2CHAPTER 32 - Disorders affecting megakaryocytes and platelets: inherited conditions Blood and Bone Marrow Pathology, Second Edition White JG 491521 London, UK Churchill Livingstone 2011 https://www.sciencedirect.com/science/article/abs/pii/B 9780702031472000328?via%3Dihub
- 3Pregnancy complicated with May-Hegglin anomaly Sri Lanka J Obstet Gynaecol Guruparan K Sooriyakumar T Muhunthan K 117119432021 https://sljog.sljol.info/articles/10.4038/sljog.v 43i 2.7988
- 4May-Hegglin anomaly and uncomplicated vaginal delivery: a report of 41 cases Am J Obstet Gynecol Bizzaro N 2262271811999 https://www.ajog.org/article/S 0002-9378(99)70473-4/abstract 10.1016/s 0002-9378(99)70473-410411837 · doi ↗ · pubmed ↗
- 5Prenatal diagnosis and obstetrical management of May-Hegglin anomaly: a case report Fetal Diagn Ther Takashima T Maeda H Koyanagi T Nishimura J Nakano H 18618971992149290710.1159/000263697 · doi ↗ · pubmed ↗
- 6Epidural anesthesia for labor and delivery in a patient with May-Hegglin anomaly: a case report Local Reg Anesth Muzannar AM Al Harbi M Rathore R 53581020172849636010.2147/LRA.S 125811 PMC 5417665 · doi ↗ · pubmed ↗
- 7May-Hegglin anomaly in a pregnancy complicated by intrauterine growth restriction and ambiguous genitalia Mil Med Magann EF Kinsella MJ Bidus MA Morrison JC 607608164199910459277 · pubmed ↗
- 8Obstetric and anesthetic considerations in the May-Hegglin anomaly. A case report J Reprod Med Nelson LH Dewan DM Mandell GL 311313381993 https://pubmed.ncbi.nlm.nih.gov/8501742/8501742 · pubmed ↗