Poverty and the health of children and adolescents at the end of the COVID-19 pandemic. Results of the KIDA study
Miriam Blume, Elvira Mauz, Mira Tschorn, Kristin Manz, Anja Schienkiewitz, Jennifer Allen, Jens Hoebel, Petra Rattay

TL;DR
This study compares the health of children and adolescents at risk of poverty with those from wealthier families after the COVID-19 pandemic.
Contribution
The study provides new insights into health disparities among children from low-income families post-pandemic.
Findings
Children at risk of poverty are more likely to have poor health compared to those from higher-income families.
Low-income children are less likely to participate in organized sports but show no difference in school-based sports.
Health disadvantages for low-income youth require societal and local interventions.
Abstract
During the COVID-19 pandemic, young people at risk of poverty were particularly affected by contact restrictions as well as by daycare centre and school closures. The aim here is to describe the health status of young people at risk of poverty in comparison to their peers from financially better-off families at the end of the pandemic. The analyses are based on the data of 3- to 15-year-olds from the study German Children’s Health Update (2022/2023). Prevalences stratified by income were determined for selected indicators of health, health-related behaviour and psychosocial stress and resources. A comparison was made between families at risk of poverty and families with medium and high incomes. Poisson regressions were adjusted for parents’ level of education. Young people at risk of poverty are more likely to have poor health than their peers from financially better-off families.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
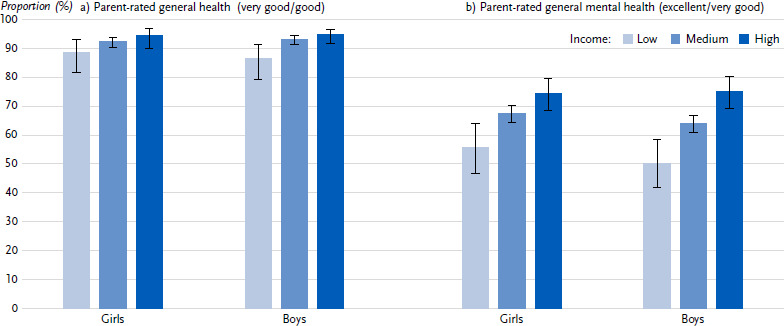 Figure 1
Figure 1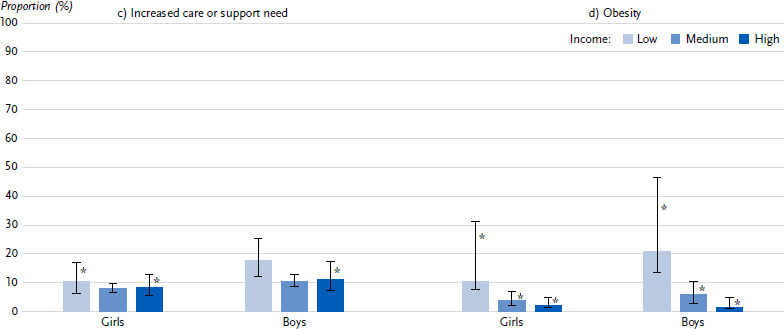 Figure 2
Figure 2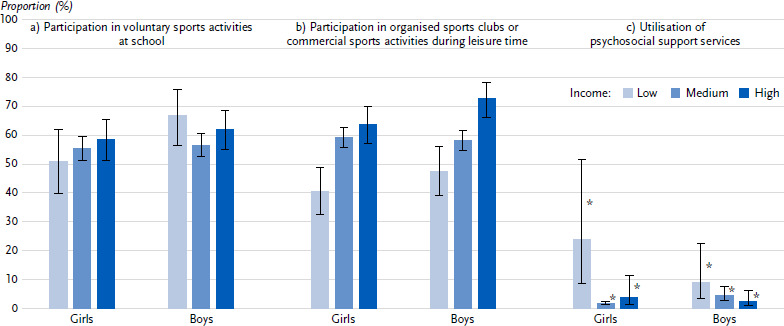 Figure 3
Figure 3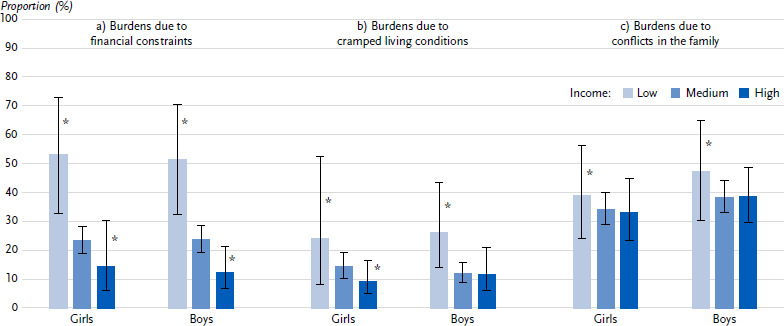 Figure 4
Figure 4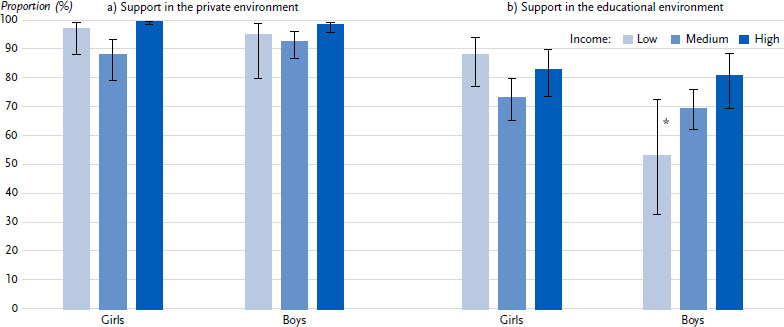 Figure 5
Figure 5- —Robert Koch Institute
- —Federal Ministry of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild and Adolescent Health
1. Introduction
According to Article 24 of the UN Convention on the Rights of the Child, all children have the right to the highest attainable standard of health [1]. However, the health opportunities of children and adolescents are unevenly distributed, even in a comparatively affluent country like Germany. Studies conducted for Germany show that children and adolescents who are at risk of poverty are more likely to have poorer health than their peers from financially better-off families [2–4].
According to the microcensus in 2022, 3.1 million children and adolescents under the age of 18 were at risk of poverty in Germany, more than one in five children (21.8 %) [5]. Children and adolescents from single-parent households [6], from families with many children [6] and from families with low education [7] or longer periods of unemployment [4] are particularly at risk of poverty. Poverty is characterised by numerous economic, social and cultural restrictions [8] and has an impact on almost all areas of children’s and adolescents’ lives. Children and adolescents at risk of poverty often experience deprivation, austerity, stigmatisation and shame in their lives [6]. Children and adolescents at risk of poverty often live in cramped living conditions with reduced opportunities to withdraw [3] and a less stimulating living environment [9]. In addition, families at risk of poverty often do not have enough money for a good quality, healthy diet [10]. Young people at risk of poverty also often experience disadvantages in the education system, which is reflected, for instance, in the strong correlation between family income and attendance at a ‘Gymnasium’ – the academically oriented secondary school track leading to university entrance qualifications [11]. Children and adolescents from families at risk of poverty therefore usually have poorer opportunities for development, education and good health from an early age [6].
The COVID-19 pandemic exacerbated the social disadvantage of poor children and adolescents in some respects [12], as young people from families at risk of poverty were particularly exposed to stress due to containment measures such as temporary contact restrictions, daycare and school closures or homeschooling [13]. Smaller homes and fewer financial resources made it difficult to provide care in the event of school closures and distance learning. In addition, parents with low levels of formal education were often unable to support children in homeschooling in the same way as parents with higher levels of formal education [13]. In the months at the end of and after the pandemic, rising prices for food, housing costs and mobility also had a greater negative impact on families living in poverty [1].
Internationally and for Germany, studies show that mental health problems [14–17] and lack of physical activity [18] increased in children and adolescents during the pandemic and have not returned to pre-pandemic levels afterwards [16].
Studies also show that socially disadvantaged children and adolescents in Germany had poorer health during and after the pandemic than their more affluent peers [12, 19–22]. The existing studies on health inequalities in children and adolescents in Germany during the COVID-19 pandemic focused on health differences and burdens depending on family wealth [19], multidimensional measures of social disadvantage [20, 21] or the socioeconomic situation of the living environment [12]. Differences depending on the family’s financial situation were only analysed in a survey of insured persons conducted by the Scientific Institute of the AOK at the beginning of 2022 [22]: both the physical and mental health of children was rated as very good or good more often by parents with a medium or high income than by parents with a low income. Children from low-income families were also affected by a lack of exercise more frequently than average. Although the study categorises family income, no data is reported explicitly for children and adolescents at risk of poverty. No nationwide results are currently available specifically on the health status of children and adolescents at risk of poverty in the context of the COVID-19 pandemic.
Key messages
- ►At the end of the pandemic, the health of children and adolescents at risk of poverty was worse than that of their peers from families with higher incomes.
- ►Children and adolescents at risk of poverty can be quite easily reached through programmes in the school setting: participation in voluntary sports activities at school was independent of income.
- ►Children and adolescents at risk of poverty are more burdened by financial restrictions and cramped living conditions than their peers from families with higher incomes.
- ►The utilisation of psychosocial support services with or for their children is higher among parents at risk of poverty than among families with higher incomes.
- ►Continuous monitoring is required to be able to analyse trends in health inequalities.
Taking this into account, the aim of this article is to provide an overview of the health status of children and adolescents from families at risk of poverty compared to financially better-off families at the end of the pandemic based on nationwide data.
To this purpose, the article examines the following questions:
How did health, health-related behaviour, psychosocial burdens and resources differ at the end of the pandemic between children and adolescents from families at risk of poverty and those with higher incomes?Are these differences independent of the educational status of the parents?
2. Methods
2.1 Study design and sample
The analyses were carried out using data from the study German Children’s Health Update (KIDA) (see Infobox), which is part of the study German Health Update (GEDA 2022/2023). The GEDA study is a cross-sectional survey conducted by the Robert Koch Institute to assess the health status of individuals aged 16 and older living in private households with their main residence in Germany at the time of data collection [23]. The survey is based on a dual-frame telephone sample, incorporating both mobile and landline phone numbers [24]. Between February 2022 and April 2023, the study design of GEDA was expanded to invite participating parents of children and adolescents aged 3 to 15, as well as 16- and 17-year-old adolescents themselves to take part in the KIDA study [23]. The KIDA study was designed to examine the health status and health-related behaviour of children and adolescents during the COVID-19 pandemic. Initially, telephone interviews were conducted with parents of 3- to 15-year-old children and with 16- to 17-year-old adolescents. Subsequently, between April 2022 and June 2023, a follow-up online survey was conducted with the same respondents.
For this analysis, only parental reports on children and adolescents aged 3 to 15 years were included. The analyses are based on data from 6,514 participants from the telephone survey and 2,760 participants from the online survey.
2.2 Indicators
The definition of risk of poverty in Germany and other member states of the European Union (EU) follows a relative concept of poverty. According to this, people are considered to be ‘at risk of poverty’ if they live in a household with such a low income that the household members are denied what is considered a ‘normal’ standard of living [6, 8]. According to the official definition, the risk-of-poverty threshold is undercut if the equivalised disposable income is less than 60 % of the median income of the total population [8, 25]. In this analysis based on KIDA data, the income groups were categorised using the median equivalised disposable income of € 1,982 for 2022 according to the Federal Statistical Office’s microcensus disposable [26] into ‘low’ (< 60 % of the median = at risk of poverty), ‘medium’ (60 % – <150 % of the median) and ‘high’ (≥ 150 % of the median) [25]. In order to calculate the equivalised disposable income, the disposable household income was divided by the sum of the means weights of all household members according to the new OECD scale [27]. This scale assigns a needs weighting of 1.0 to the first adult in the household, a needs weighting of 0.5 to each additional person in the household and a needs weighting of 0.3 to household members under the age of 14. The needs weighting is used to take cost savings in multi-person households through joint economic activity into account when determining the financial situation or risk of poverty of a household. Missing values for the equivalised disposable income were imputed using a multiple regression model. For this purpose, the respondents‘ information on their age, education and employment status as well as regional statistical information on the average disposable household income of the respondents’ region of residence were used. Further socio-demographic characteristics considered were the age of the children and adolescents (3 – 10 years and 11 – 15 years), the gender recorded on the birth certificate (female, male; children with an open gender entry were not taken into account) and the household’s highest level of education. The highest educational qualification of the household included the school and vocational qualifications of both parents. Using the CASMIN classification (Comparative Analyses of Social Mobility in Industrial Nations), the educational qualifications were categorised as ‘low’, ‘medium’ and ‘high’ [28].
KIDA – German Children’s Health UpdateMonitoring child health during and after the COVID-19 pandemicData holder: Robert Koch InstituteObjectives: provision of reliable information on the physical and mental health status and health-related behaviour of children and adolescents aged 3 to 17 years.Study design: nationwide cross-sectional telephone survey and follow-up in-depth online survey.Population: parents of children aged 3 – 15 years and adolescents aged 16 – 17 years who are integrated in the ongoing GEDA study.Sampling: random sample of landline and mobile phone numbers (dual frame method) from the sampling system of the ADM (Arbeitskreis Deutscher Markt- und Sozialforschungsinstitute e.V.).Sample size: telephone sample = 6,992 participants, online sample = 2,894 participantsStudy period: February 2022 until June 2023Further information in German is available at www.rki.de/kida
The following outcome variables were selected to represent different dimensions of health (see Annex Table 1):
►Health status: parent-rated general health, parent-rated general mental health, increased care or support need, obesity►Health-related behaviour: participation in voluntary sports activities at school, participation in organised sports clubs or commercial sports activities during leisure time, utilisation of psychosocial support services►Psychosocial burdens and resources: support in the educational and private environment, burdens due to financial constraints, cramped living conditions, and conflicts in the family
2.3 Statistical analyses
In the first step, stratified prevalences by income group, 95 % confidence intervals and p-values by chi-square were calculated separately for the overall group and by gender. For the health indicators from the telephone survey, Poisson regression was also used to check whether the interaction between gender and income is significant. Due to the small sample size, only the values for the prevalences of the overall group are reported for the health indicators from the online survey; results stratified by gender are only shown graphically. If the lower limit of the confidence interval is less than 2/3 of the prevalence, the relevant result is marked as statistically uncertain in the figure (*).
In the second step, Poisson regression was used to calculate adjusted prevalence ratios with 95 % confidence intervals for each health outcome. The prevalence ratio indicates the ratio of the prevalences of a group and a reference group. In Model 1, the results were adjusted for gender and age. In Model 2, the highest parental educational qualification of the household was also included in the modelling. Only cases with complete information on age, gender and parental education were included. P-values less than 0.05 were considered statistically significant.
All calculations were carried out using a design weighting, which is determined by the selection probability of the individual respondents, and an adjustment weighting, which adapts the sample to the population distribution with regard to the variables region, age, gender and level of education. As not all participants in the KIDA telephone survey also took part in the online survey, drop-out weights were calculated for these respondents using the information from the telephone survey in order to minimise selection effects [23].
3. Results
The description of the sample (Annex Table 2) shows that the proportion of children and adolescents at risk of poverty is 16.9 % in the telephone sample of the KIDA study and 11.0 % in the online sample. There is a strong correlation between disposable household income and parental education: 39.0 % of parents from families at risk of poverty have a low level of education, while this applies to only 5.7 % of parents in the high-income group. Similarly, 11.7 % of parents from families at risk of poverty have a high level of education compared to 66.2 % of high-income families.
3.1 Results of the bivariate analyses
Health status
With regard to health status, most indicators differ according to household income to the disadvantage of children and adolescents from families at risk of poverty (Annex Table 3). Their parents are less likely to rate their children’s general health as very good or good (87.4 %) than parents from medium- or high-income families (92.8 % and 94.6 % respectively). Furthermore, children and adolescents from families at risk of poverty are less likely to have excellent or very good parent-rated mental health (52.7 %) than their peers from high-income families (74.8 %). In addition, their parents report an increased care or support need more frequently (14.6 %) than parents with middle- or high-income (9.4 % and 9.8 % respectively). The obesity prevalence is more than three times higher among children and adolescents at risk of poverty (16.5 %) than among their peers from middle-income (5.0 %) or high-income (1.9 %) families. The differences in health according to income groups appear to be slightly more pronounced for boys than for girls, even if the interaction term of income and gender is not statistically significant (based only on the indicators of the telephone survey) (Figure 1).
Health-related behaviour
With regard to physical activity behaviour in childhood and adolescence, 57.6 % of parents stated that their child takes part in voluntary sports activities at school (Annex Table 3). Here, no differences were found between income groups. However, there is a statistically significant income gradient when it comes to participation in organised sports clubs or commercial sports activities during leisure time: while 67.9 % of children and adolescents in the high-income group make use of sports clubs or commercial sports activities, 58.7 % in the middle-income group and 44.5 % in families at risk of poverty do so. For both indicators, there were no differences between girls and boys in terms of the association with income (Figure 2). Psychosocial support services to overcome challenges in connection with the COVID-19 pandemic were utilised more frequently for or with children and adolescents at risk of poverty by their parents (15.9 %) than for children and adolescents in the middle- and high-income groups (3.1 % each) (Annex Table 3).?
Psychosocial burdens and resources
At the end of the pandemic, 52.3 % of children and adolescents from families at risk of poverty were burdened by financial restrictions, while this applied to 23.5 % of their peers from families in the middle-income group and 13.3 % from families in the high-income group (Annex Table 3). Burdens due to cramped living conditions were reported for just under a quarter of children and young people from families at risk of poverty. In families with a medium or high income, these burdens are lower (13.1 % and 10.5 % respectively). There are no statistically significant differences for stress caused by conflicts within the family.
In addition, children and adolescents from middle-income families (90.2 %) are less likely to receive private support than their peers from high-income families (98.8 %) (Annex Table 3). The proportion of children and young adolescents at risk of poverty who receive support in the private environment (95.7 %) lies between the middle- and high-income groups. In the school environment, 67.2 % of children and young people from low-income families, 71.3 % from middle-income families and 81.7 % from high-income families receive support, although the differences are not statistically significant. Gender-stratified analysis shows, however, that girls at risk of poverty receive support in the school environment significantly more often than boys at risk of poverty (Figure 4).
3.2 Results of the multivariate analyses
Controlling for gender and age (Model 1) in the multivariate regression analyses, the bivariate-observed differences by income remain (Table 1). Exceptions are the increased need for care and support, and support in the private environment, where there are no longer any statistically significant differences in income.
When parents’ level of education is added to the modelling (Model 2), the higher prevalence ratios for children and adolescents at risk of poverty are partially reduced compared to Model 1, but remain statistically significant. This applies to parents’ assessments of their children’s mental health, obesity, participation in sports clubs or commercial sports activities, use of psychosocial services and the burden of financial constraints. Only in the case of general health are there no longer any statistically significant differences in income after additionally controlling for parents’ level of education.
4. Discussion
The KIDA study describes the health status of children and adolescents at the end of the COVID-19 pandemic in Germany. The results show that children and adolescents at risk of poverty had poorer health opportunities in 2022/2023 than their peers from financially better-off families: they have poorer parent-rated general and mental health, are more likely to have increased care and support needs and to be obese; they are more often burdened by financial worries and cramped living conditions and are more likely to make use of psychosocial support services with their parents. In addition, they receive less support in their private environment and are less likely to take part in sports clubs or commercial sports activities during leisure time, while they participate in voluntary sports activities at school at a similar rate to their peers in higher income groups.
The reported results are largely in line with existing research findings: living in conditions with a risk of poverty and the experience of deprivation, shame and marginalisation that often go hand in hand with this are associated with impaired mental health in children and adolescents in particular [6]. This is already evident in previous nationwide studies, such as the German Health Interview and Examination Survey for Children and Adolescents (KiGGS Wave 2) from 2014 to 2017 [2]. Here, however, emotional and behavioural problems were measured as indicators of mental health (Strengths and Difficulties Questionnaire, SDQ), so that the results are not directly comparable. Data from the Scientific Institute of the AOK for the pandemic period also show that low-income mothers are significantly less likely to rate their children’s mental health as very good or good, and more likely to report a deterioration in their children’s mental health during the pandemic than mothers with a medium or high disposable household income [22].
With regard to the general health of their children as assessed by their parents, KiGGS Wave 2 (2014-2017) also shows that children and adolescents at risk of poverty are in poorer health than their peers from families with higher incomes [2]. However, while, in KiGGS Wave 2, 92.0 % of children and adolescents at risk of poverty were assessed by their parents as being in very good or good health [2], the KIDA study found this percentage to be only 87.4 %. Nevertheless, lower prevalences were also found for the middle- and high-income groups in the KIDA study than in KiGGS Wave 2. This may be due to a generally poorer assessment of health during the pandemic. However, it should be noted that the prevalences are not directly comparable due to the differences in the age range (KiGGS Wave 2: 3 – 17 years), the sampling design and the survey methods.
The increased care or support need observed here among children and adolescents at risk of poverty were measured using an item from the Children-with-Special-Health-Care-Needs-Screeners (CSHCN) and are therefore not comparable with results based on the overall screener or other items from the screener [2, 29]. During the COVID-19 pandemic, results from a study in Germany show that children with higher care needs (measured with the CSHCN Total Screener) receive less social support if they live in a family with a low socio-economic status than their peers from more affluent families [29]. No studies can be found specifically on the care and support needs of children and adolescents at risk of poverty after the pandemic, showing a research gap for Germany.
The higher prevalence of obesity observed among children and adolescents at risk of poverty is consistent with a nationwide study conducted before the pandemic [2]. The income-related differences in obesity prevalence appear more pronounced in the KIDA study compared to KiGGS Wave 2. However, in KiGGS Wave 2, body height and weight were obtained using standardized procedures in examination centres. In the KIDA study, these data are based on parental reports, which are less valid than objectively measured values [30]. It is evident that parents are often unable to provide accurate information on body height and weight, especially for older children and adolescents. In the KIDA study, the data were additionally collected via an online survey, which involved a smaller sample size, thereby resulting in prevalence estimates with greater statistical uncertainty. The association between poverty and obesity is mediated, among other factors, by diet and exercise: poverty can impede access to healthy food options [10], and to opportunities for sports and physical exercise [31]. The findings of the KIDA study also indicate this for participation in sport activities during leisure time.
According to the KIDA data, children and adolescents in families at risk of poverty are less likely to participate in sports clubs or commercial sports activities during leisure time, which is comparable with the results from KiGGS Wave 2 on sporting activity during leisure time in general [2]. Unlike in KiGGS Wave 2, however, the KIDA study explicitly asked whether they participate in sports clubs or commercial sports activities, i.e. organised sports activities. According to analyses of the Socio-Economic Panel, adolescents at risk of poverty aged 17 also make use of sports activities in clubs less frequently than adolescents not at risk of poverty [32]. Many commercial sports facilities (such as gyms, tennis lessons, ballet or swimming schools) involve costs that are a major barrier for families at risk of poverty [32, 33]. Support benefits from the education and participation package, a state support programme for young people from low-income families (e.g. subsidies for sports club fees), are often not claimed due to the perceived stigmatisation and shame involved. In addition, lack of awareness of the entitlement to benefits as well as the complicated application process often lead to non-utilisation of the support services [34]. It can also be assumed that high-priced commercial sports programmes are offered less frequently in socio-economically deprived residential areas. There are also associations between the physical activity behaviour of parents and their children [35]. Factors such as the parents’ sporting activity, their support and attitudes towards sport are discussed in this context as important factors for the child’s sporting and physical activity [36, 37].
In contrast to sports activities during leisure time, KIDA data shows that children and adolescents at risk of poverty participate in voluntary sports activities at school at a similar rate to their peers from families with higher incomes. Before the pandemic, there was even evidence of more frequent participation in voluntary sports activities at school among 17-year-old adolescents from households at risk of poverty [32]. Children and adolescents at risk of poverty can therefore be reached effectively with school programmes. The possibility of using these programmes free of charge could have great relevance here [32].
In addition to the increased need for care and support among children and adolescents at risk of poverty, the KIDA study also observed a higher utilisation of psychosocial support services by parents and children and adolescents at risk of poverty. However, on the basis of the KIDA study data, it was not possible to answer the question of whether the need for support was met – at least in part – by the services utilised. Analyses included in the KIDA quarterly reports [23], also show that parents at risk of poverty are more often unaware of the support services mentioned in the survey than families with medium or high incomes.
The increased burden on children and adolescents from families at risk of poverty due to cramped living conditions during the pandemic is supported by analyses using data from the Socio-Economic Panel [38]. In these analyses, cramped living space are most frequently reported by families receiving unemployment benefit II. The higher burden of cramped living conditions on children and adolescents at risk of poverty emphasises the importance of sufficient living space for the well-being of young people. The relevance of quantitatively and qualitatively sufficient living space is recognised, for instance, as important for a good family climate, space for socialising with friends and opportunities for retreat [3], which is why ‘sufficient living space’ was also defined as a goal for all member states within the European Child Guarantee [39]. In addition to the burdens caused by cramped living conditions, financial burdens for children and adolescents at risk of poverty were also reported most frequently. In 2022 and 2023 in particular, expenditure on food and heating costs, for example, rose sharply [40]. The limited financial resources and the associated restrictions for families at risk of poverty were therefore also noticeable with the children.
Although, according to the KIDA data, children and adolescents at risk of poverty are more likely to experience psychosocial burdens and health problems and have an increased need for care and support, the results show that, at the end of the pandemic, only two out of three children and adolescents always or mostly received support in the school environment. In the high-income group, this figure is eight out of ten children and adolescents. Even if the differences in income are not statistically significant, there is still a need for action here. With regard to the support perceived by parents for their children in the private environment, there are no differences according to family income. In all income groups, more than nine out of ten children and adolescents receive sufficient support in their private environment. However, in answer to this question, parents themselves rated the support they provide; it can be assumed that an assessment by the young people themselves could be somewhat different. Nevertheless, good support from the private environment is an important resource, especially for children and adolescents at risk of poverty.
The question of whether and to what extent income differences in health, health-related behaviour and psychosocial burdens and resources differ between girls and boys is not analysed in depth in this article. This would require studies with a larger sample size. The sample size is too small for a simultaneous stratification by income and gender, especially for the indicators collected in the online survey. Existing differences could therefore be underestimated or overlooked (ß-error). The results presented here in graphical form should therefore be viewed with great caution.
Even if the differences by gender with regard to the associations between income and health are not statistically significant, the associations appear to be stronger for boys than for girls. With regard to sports activities, it is known that boys participate more frequently than girls in organised sports clubs or commercial sports activities in their leisure time [41]. The association between income and participation in sports clubs or commercial sports activities during leisure time and participation in voluntary sports activities at school does not vary statistically significantly by gender. However, in the case of voluntary sports activities at school, differences tend to emerge in the association between participation and income: while girls at risk of poverty are slightly less likely to take part in voluntary sports activities clubs at school than girls in other income groups, boys at risk of poverty are slightly more likely to take part in these programmes than boys in other income groups. Support in the school environment is reported more frequently for girls by parents at risk of poverty than by parents with medium and high incomes. This is less often the case for boys. Whether this corresponds to reality or whether girls at risk of poverty report more frequent support in the school context than boys, or whether parents at risk of poverty are more dissatisfied with the support received by boys cannot be assessed with the data from the KIDA study.
The second research question aims to determine whether the reported differences in health, health-related behaviour and psychosocial burdens and resources can be attributed to a lower level of formal education among parents -which is often associated with poverty. Although some of the analysed associations with income are weakened, they basically hold up when the parents’ level of education is taken into account. This applies to parent-rated mental health, obesity, participation in sports clubs or commercial sports activities, utilisation of psychosocial services and the burden of financial constraints. This indicates an independent relevance of the income situation for these health aspects, which goes beyond the health relevance of education. In this respect, the KIDA results support previous findings for adulthood, which are available both internationally and for Germany and confirm the independent relevance of poverty or financial disadvantage as a social determinant of health [42, 43]. Only in the case of parent-rated general health are there no longer any statistically significant differences in income after adjustment for parents’ level of education.
4.1 Strengths and limitations
The strength of the KIDA study is that it provides data on a large number of health-related, social and socio-economic indicators as well as for different age groups in childhood and adolescence at the end of the pandemic, which also enables conclusions to be drawn regarding the health status of children and adolescents at risk of poverty.
One limitation of the present analysis is that the KIDA study is only partially representative of the nationwide population of children and adolescents. Access via the GEDA study resulted in no direct random selection of children and adolescents but of one parent. In addition, only some of the parents from the GEDA study took part in the KIDA study. Then again, fewer parents took part in the online survey than in the telephone survey. This dropout rate may have led to a selection of participants. For example, it cannot be ruled out that parents with high psychosocial burdens participated less frequently in the KIDA study. In particular, parents with a low level of education were less likely to take part in the KIDA study. A complex weighting procedure was used in order to be able to make population-based conclusions.
The combination of telephone and online survey was also accompanied by a change in the survey mode, which may have contributed to different response behaviour. When interpreting the results, it should also be considered that the data for 3- to 15-year-olds is based on information provided by their parents, which may differ from the children’s and adolescents’ self-reporting, particularly with regard to information on mental health, height or body weight [44]. As the KIDA study is a cross-sectional survey, no conclusions can be drawn from the analyses regarding causality or direction of effect.
4.2 Conclusions
At the end of the pandemic, the health of children and adolescents at risk of poverty continues to be appreciably worse than that of their peers from less precarious living conditions. Even though there is no clear evidence of an increase in health inequalities in childhood and adolescence in Germany at the end of the pandemic [12, 19–21], it can be assumed that children and adolescents growing up in poor living conditions will be more affected in the long term in terms of their well-being and their ability to cope with developmental tasks by the burdens of the pandemic, but also by current crises such as climate change, military conflicts within and outside Europe, and the economic downturn. Important developmental steps and experience in childhood and adolescence that were missed out during the pandemic or due to a lack of financial or social resources may not be recoverable, or only to a limited extent [45]. It is therefore possible that the increase in health inequalities in this cohort will only appear with a time lag, which is why future studies should pay particular attention to it and continue to monitor it from the perspective of health equity.
It is therefore particularly important to increase activities that improve both the living conditions and the individual health of children and adolescents living in poverty. While designing these interventions, the specific family circumstances of children and adolescents at risk of poverty should be taken into account; for example, if they live in single-parent households or families with many children. Health promotion is to be understood as a cross-sectional task that, in line with the World Health Organisation’s (WHO) health-in-all-policies approach, requires measures in various policy areas and thus the cooperation of many political departments as well as actors with practical experience and those from science and civil society [46]. Strategies to combat child and family poverty and to reduce disadvantages and marginalisation of children and adolescents living in poverty and at risk of poverty are at the top of the agenda. To this purpose, the recommendation on the introduction of a European Child Guarantee was adopted at European level in 2021 [39], which complements the European Union’s comprehensive children’s rights strategy [47]. This strategy is being implemented in Germany through the National Action Plan ‘New Opportunities for Children’ (‘Neue Chancen für Kinder’) [48], which was adopted in 2023 and aims to ensure better access for socially disadvantaged children and adolescents to early childhood care, education and upbringing, school-related activities, at least one healthy meal per school day, healthy food and adequate housing as well as healthcare. In the first progress report on the implementation of the National Action Plan for 2025, a statement from different civil society actors calls, among other things, for the formulation of measurable and time-bound targets that will allow monitoring the progress in reducing child poverty [49].
In addition to these infrastructural improvements, the introduction of a basic child protection guarantee is called for to ensure that all children and adolescents have a minimum standard of living, to protect them from poverty and to improve their opportunities for participation [50]. The UN Convention on the Rights of the Child recognises ‘[…] the right of every child to a standard of living adequate for the child’s physical, mental, spiritual, moral and social development’ [1]. The National Action Plan ‘New Opportunities for Children’ therefore also aims to increase parental labour-force participation, which can contribute to families’ economic stability [48]. The Children’s Rights Network is calling for all measures taken by the Federal Government to be scrutinised in terms of how they affect the situation of children and adolescents, and, in particular, groups at risk of poverty [51].
In order to adequately address the complexity of promoting health and reducing health inequalities in childhood and adolescence, political strategies and measures at federal and state levels need to be complemented by measures at the level of local communities and local living environments. According to the interministerial working group ‘Health effects of the coronavirus on children and adolescents’, measures to promote the health of children and adolescents should be connected to regulatory structures such as daycare centres or schools, which are accessible to all young people at a low threshold and without stigmatisation [52]. This recommendation is supported by the results of the KIDA study presented here, which show that children and adolescents at risk of poverty can be reached just as well as their peers from more affluent backgrounds through sports activities in a school context. Prevention chains are recognised as a suitable structural approach to prevention in order to coordinate the various measures and services offered by a local authority to promote health and reduce health inequalities in a targeted manner [53]. Prevention chains are designed to establish an integrated overall strategy and a sustainable network of support, counselling and promotion at a local level and with the participation of children, adolescents and families [53].
Beside this bundle of measures, Germany needs a nationwide and continuous monitoring of health and health inequalities in childhood and adolescence in order to recognise long-term trends, and to be able to rapidly identify problems in acute crises such as a pandemic. Furthermore, evaluation studies are needed to provide information on which measures are effective in reducing child poverty and health inequalities in practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Deutsches Kinderhilfswerk e.V. (eds.). Children’s Report Germany 2023. Child poverty in Germany 2023 [Kinderreport Deutschland 2023. Kinderarmut in Deutschland] 2023 [cited 28.02.2024]. Available from: https://www.bmfsfj.de/resource/blob/228174/f 84545059 dda 8d 42b 17e 419e 30c 40163/kinderreport-2023-data.pdf.
- 2Lampert T Kuntz B. Effects of poverty for health and health behavior of children and adolescents: Results from Ki GGS Wave 2. [Auswirkungen von Armut auf den Gesundheitszustand und das Gesundheitsverhalten von Kindern und Jugendlichen. Ergebnisse aus Ki GGS Welle 2.]. Bundesgesundheitsbl. 2019;62(10): 1263-74. doi: 10.1007/s 00103-019-03009-6.10.1007/s 00103-019-03009-631529186 · doi ↗ · pubmed ↗
- 3Bertelsmann Stiftung (eds.). Consequences of poverty for children and young people. Findings from empirical studies in Germany. [Armutsfolgen für Kinder und Jugendliche. Erkenntnisse aus empirischen Studien in Deutschland.]. 2016 [cited 15.01.2025]. Available from: https://www.bertelsmann-stiftung.de/de/publikationen/publikation/did/armutsfolgen-fuer-kinder-und-jugendliche.
- 4Tophoven S Lietzmann T Reiter S Wenzig C. Poverty patterns in childhood and adolescence. Longitudinal analyses of child poverty. [Armutsmuster in Kindheit und Jugend. Längsschnittbetrachtungen von Kinderarmut]. Gütersloh: Bertelsmann Stiftung; 2017.
- 5Statistisches Bundesamt. At-risk-of-poverty rates, federal states by socio-demographic characteristics (federal median). [Armutsgefährdungsquoten, Bundesländer nach soziodemografischen Merkmalen (Bundesmedian).]. [cited 12.02.2024]. Available from: https://www.statistikportal.de/de/sbe/ergebnisse/einkommen-armutsgefaehrdung-und-soziale-lebensbedingungen/armutsgefaehrdung-und-4.
- 6Funcke A Menne S. Child and youth poverty in Germany. [Kinderund Jugendarmut in Deutschland]. Gütersloh: Bertelsmann Stiftung; 2023 [cited 11.12.2023]. Available from: https://www.bertelsmann-stiftung.de/de/publikationen/publikation/did/factsheet-kinder-und-jugendarmut-in-deutschland.
- 7Statistisches Bundesamt. Children and young people of parents with a low level of education are particularly at risk of poverty. [Kinder und Jugendliche von Eltern mit niedrigem Bildungsabschluss besonders von Armut bedroht.]. Wiesbaden 2024 [updated 26.7.2023]. Available from: https://www.destatis.de/DE/Presse/Pressemitteilungen/2023/07/PD 23_N 045_63.html.
- 8Rat der Europäischen Union. Joint report of the Commission and the Council on social inclusion. [Gemeinsamer Bericht der Kommission und des Rates über die soziale Eingliederung.] 7101/04. Brüssel 2004 [cited 28.02.2024]. Available from: https://ec.europa.eu/employment_social/soc-prot/soc-incl/final_joint_inclusion_report_2003_de.pdf.