Endovascular Repair of Ascending Aortic Pseudoaneurysm (Zone 0) After Coronary Artery Bypass Grafting
Jonathan J. Szeto, Jason J. Han, Amit Iyengar, Rohan Shad, Chase R. Brown

TL;DR
This paper describes a successful endovascular repair of a rare aortic complication after heart surgery in a high-risk patient.
Contribution
The paper presents a novel application of endovascular techniques for treating a post-CABG aortic pseudoaneurysm.
Findings
Thoracic endovascular aortic repair was effective in treating a post-CABG aortic pseudoaneurysm.
The patient was at prohibitive risk for redo open surgery due to comorbidities.
Endovascular repair is a viable alternative for high-risk patients with post-CABG complications.
Abstract
Aortic pseudoaneurysms, rare but potentially life-threatening complications following coronary artery bypass grafting (CABG), are ideally addressed with re-exploration and open repair. We present a 67-year-old female who had recently undergone a CABG and developed a large mediastinal pseudoaneurysm from the site of the proximal saphenous vein graft anastomosis but was at prohibitive risk for redo open surgery due to significant comorbidities. An application of current endovascular devices was required to treat this post-CABG complication. Thoracic endovascular aortic repair of the ascending aorta was effective in treating the aortic pseudoaneurysm CABG complication in this patient who was at prohibitive risk of redo open surgery.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
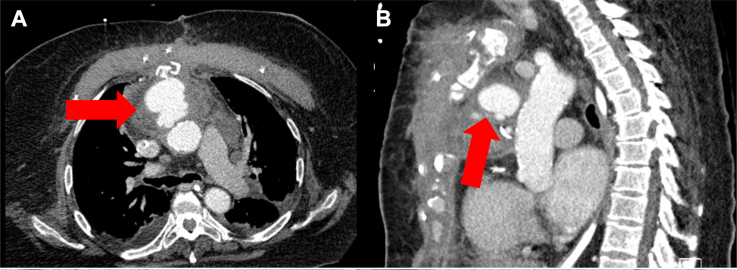 Figure 1
Figure 1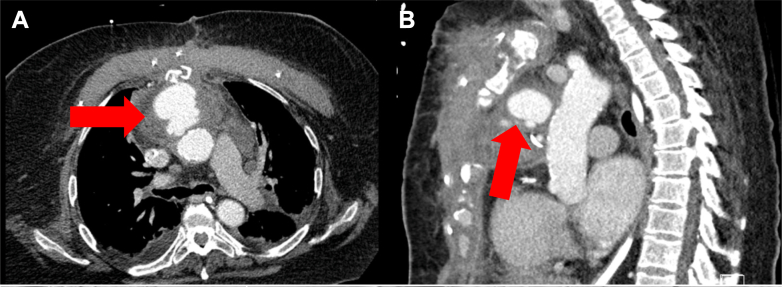 Figure 2
Figure 2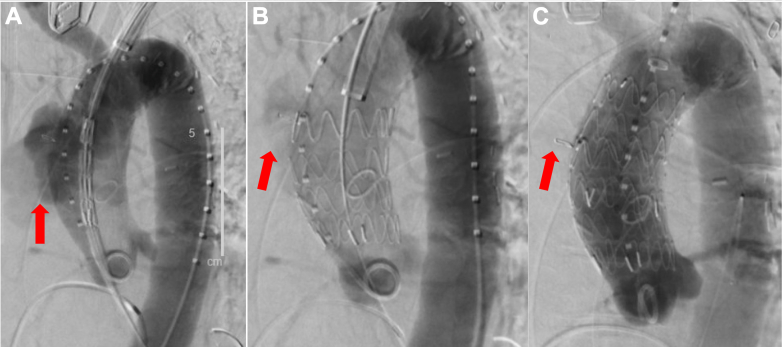 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Disease and Treatment Approaches · Aortic aneurysm repair treatments · Cardiac Valve Diseases and Treatments
Case summary
A 67-year-old female who recently underwent a coronary artery bypass graft involving bypassing 2 blocked coronary arteries (left internal mammary artery–left anterior descending artery and saphenous vein graft [SVG]–obtuse marginal) presented with worsening symptoms of weakness, dyspnea, peripheral edema, and chest pain during the same admission. A computed tomography angiogram was performed that showed a large mediastinal pseudoaneurysm arising from the site of the proximal SVG anastomosis on the ascending aorta (Figures 1 and 2). Given her severe chronic obstructive pulmonary disease, stage 3 chronic kidney disease, and prior sternal wound infection requiring pectoralis flap closure, the patient was deemed prohibitively high risk for redo open surgery and underwent an endovascular repair (Video 1).Take-Home Message
- •TEVAR of the ascending aorta can be a useful tool to address aortic complications arising from a coronary artery bypass graft procedure in patients who are at prohibitive risk of redo open surgery. Figure 1. Preoperative Contrast Enhanced Computed Tomography AngiographyPreoperative contrast-enhanced computed tomography angiography shows the ascending aorta zone 0 pseudoaneurysm (5 cm × 5 cm × 5 cm) arising in the saphenous vein graft anastomosis in both axial (A) and sagittal (B) views.Figure 2. Intraoperative Fluoroscopic AngiographyPseudoaneurysm (red arrow) before stenting (A), after inserting first proximal endovascular aortic repair endograft (EVAR) stent (B), and after inserting the second distal EVAR endograft stent to ensure complete exclusion (C). Insertion of the second EVAR stent led to full exclusion of the pseudoaneurysm.
Discussion
Aortic pseudoaneurysms are rare but potentially life-threatening complications following coronary artery bypass graft. Dehiscence at the proximal anastomosis, in part due to technical failure, can lead to rupturing of the aortic wall, causing a pseudoaneurysm. Although this clinical complication is ideally addressed with re-exploration and open repair, some patients are deemed prohibitively high risk for open surgery.1 Because of the lack of a U.S. Food and Drug Administration–approved endograft designed to treat ascending aortic pathology, creative application of current endovascular devices was required to prevent further growth or rupture of the pseudoaneurysm in this patient with suitable aortic anatomy. Medical or palliative care could be considered if the patient was not fit for an endovascular intervention; however, these approaches have poor prognoses.
Exclusion of the SVG–obtuse marginal anastomosis had the potential to cause acute myocardial ischemia. Thus, it was imperative to evaluate the patient’s coronary anatomy preoperatively via a left heart catheterization study (Video 2) and ensure bailout options that would protect against life-threatening myocardial infarction. In this case, we proceeded because the patient had adequate collateralization from her native left main coronary artery and the patent left internal mammary artery–left anterior descending artery graft. If this had not been the case, we considered stenting the lesion in her left main coronary artery before thoracic endovascular aortic repair (TEVAR) or simply tolerating a lateral wall myocardial infarction. Postoperatively, an electrocardiogram suggested no evidence of coronary ischemia.
Postoperative computed tomography imaging revealed a small type II endoleak into the pseudoaneurysm sac (Supplemental Figure 1). Before the operation, the team acknowledged the potential for type II endoleak due to retrograde flow from the open SVG. Preoperative embolism of the SVG graft was considered; however, the team did not proceed because there was no way to safely embolize the SVG. Half of type II endoleaks resolve spontaneously and persistent type II endoleaks are not associated with decreased survival, so the team decided that the risk of complications from an unsuccessful embolization outweighed the potential complications of a type II endoleak.2 Zone 0 TEVARs are especially challenging due to various anatomical factors, such as aortic arch angulation, supra-aortic head vessel branching, and high blood flow.3 The difficult anatomy of the aortic arch, combined with a lack of specific devices designed for zone 0 TEVAR, limit this procedure from becoming more standard fashion. Ongoing investigation of ascending TEVAR endograft technology must still be fully evaluated; however, this case shows that they can be a useful tool in managing postoperative ascending aorta complications.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Plichta R.P.Hughes G.C.Thoracic endovascular aortic repair for the ascending aorta: experience and pitfalls J Visualized Surg 452018 article 5.10.21037/jovs.2018.03.01PMC 599444829963381 · doi ↗ · pubmed ↗
- 2Lo R.C.Buck D.B.Herrmann J.Risk factors and consequences of persistent type II endoleaks J Vascular Surg 634201689590110.1016/j.jvs.2015.10.088PMC 480861326796291 · doi ↗ · pubmed ↗
- 3Roselli E.E.Atkins M.D.Brinkman W.ARISE: First-in-human evaluation of a novel stent graft to treat ascending aortic dissection J Endovasc Ther 304202355056010.1177/1526602822109501835587698 · doi ↗ · pubmed ↗