A Survey on the Perceptions of Puerto Rican Cardiologists on the Use of Smartwatches and Implantable Loop Recorders
Roberto J Lapetina Arroyo, Ángel S Pagán Jiménez, Diego Calo, Gabriel Horruitiner, Jose E. Lopez Ventosa, Hilton Franqui

TL;DR
This study explores how Puerto Rican cardiologists view smartwatches and implantable loop recorders for monitoring heart rhythm disorders like atrial fibrillation.
Contribution
It provides insights into cardiologists' perceptions and preferences for wearable and implantable cardiac monitoring devices in Puerto Rico.
Findings
82% of cardiologists identified device cost as a limitation for smartwatch use in cardiac monitoring.
62.5% of cardiologists preferred implantable loop recorders over smartwatches for high-risk atrial fibrillation patients.
Non-subspecialized cardiologists were more likely to perceive device accuracy as a limitation for smartwatch use (p = 0.0234).
Abstract
A variety of portable monitoring devices have become available and have proven to be of use in the monitoring of atrial fibrillation (AF). Implantable loop recorders (ILRs) have been shown to have great sensitivity in recording arrhythmia events in long-term arrhythmia monitoring. Recently, smartwatches have gained prominence as an unobtrusive alternative for heart rhythm monitoring. The purpose of this study was to gain a better understanding of the perception of Puerto Rican cardiologists on the use of these devices in the management of AF, particularly when compared to more established long-term devices like ILRs. We administered a survey questionnaire to cardiologists currently practicing in Puerto Rico. Demographic information was collected through participant self-reporting. Participants were defined into subgroups as follows: having a cardiac subspecialty, being associated with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
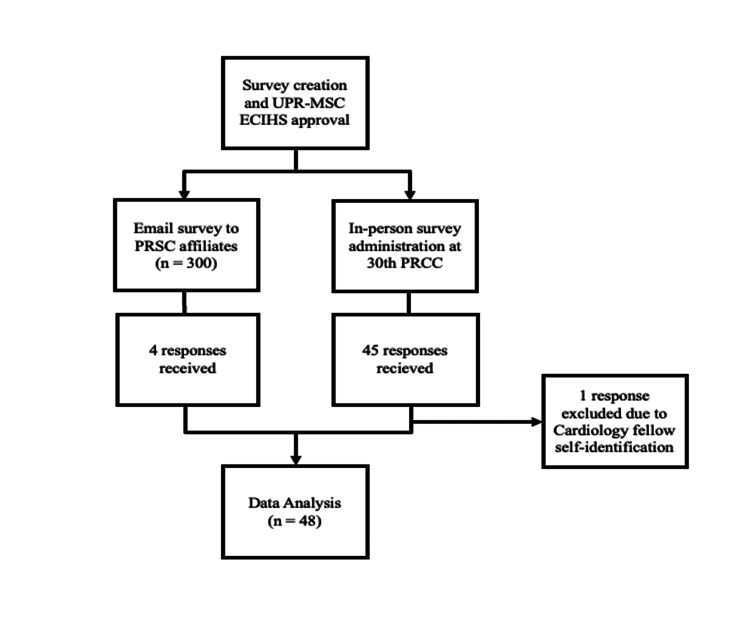 Figure 1
Figure 1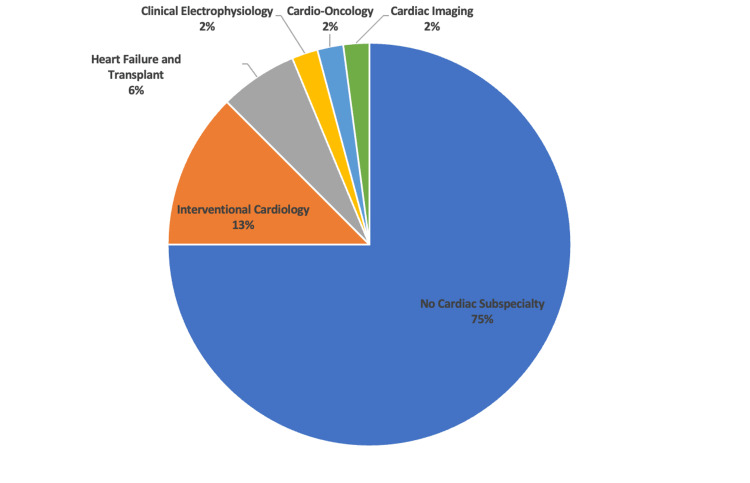 Figure 2
Figure 2| Category | Variable | Value |
| Age | Mean ± SD | 55.6 ± 12.4 |
| Range | 31 to 81 | |
| Sex | Male (n) | 44 |
| Female (n) | 4 | |
| Medical practice setting | Hospital (n) | 10 |
| Private Office (n) | 38 | |
| Years in practice | Mean ± SD | 21.7 ± 12.2 |
| Range | 1 to 44 | |
| Academia affiliation | Yes (n) | 19 |
| No (n) | 29 | |
| Cardiologists with subspecialty | Total with Subspecialty (n) | 12 |
| Interventional Cardiology (n) | 6 | |
| Heart Failure and Transplant (n) | 3 | |
| Clinical Electrophysiology (n) | 1 | |
| Cardio-Oncology (n) | 1 | |
| Cardiac Imaging (n) | 1 |
| Strongly Agree | Agree | Neither Agree nor Disagree | Disagree | Strongly Disagree | |
| Smartwatches can accurately detect Afib | n = 16 [33.3%] | N = 23 [47.8%] | N = 6 [12.5%] | N = 3 [6.3%] | N = 0 [0%] |
| ILRs can accurately detect Afib | N = 29 [60.4%] | N = 16 [33.3%] | N = 3 [6.3%] | N = 0 [0%] | N = 0 [0%] |
| Accuracy of Afib detection of a smartwatch is equal to that of ILRs | N = 1 [2.1%] | N = 15 [31.3%] | N = 18 [37.5%] | N = 14 [29.2%] | N = 0 [0%] |
| Smartwatches are reliable alternatives for cardiac rhythm monitoring | N = 9 [18.8%] | N = 26 [54.2%] | N = 8 [16.7%] | N = 4 [8.3%] | N = 1 [2.1%] |
| ILRs are reliable alternatives for cardiac rhythm monitoring | N = 16 [33.3%] | N = 26 [54.2%] | N = 2 [4.2%] | N = 3 [6.3%] | N = 1 [2.1%] |
| Cardiac rhythm information yielded by smartwatches should be incorporated in guideline-directed anticoagulation therapy for the management of Afib | N = 7 [14.6%] | N = 23 [47.9%] | N = 14 [29.2%] | N = 3 [6.3%] | N = 1 [2.1%] |
| Smartwatches are reliable for detecting paroxysmal Afib in at-risk patients | N = 10 [20.8%] | N = 26 [54.2%] | N = 9 [18.8%] | N = 2 [4.2%] | N = 1 [2.1%] |
| Main benefit of smartwatches is the detection of unapparent paroxysmal Afib | N = 14 [29.2%] | N = 28 [58.3%] | N = 3 [6.3%] | N = 3 [6.3%] | N = 0 [0%] |
| Smartwatches are an unobtrusive alternative for most patient's lives | N = 19 [39.6%] | N = 24 [50.0%] | N = 2 [4.2%] | N = 2 [4.2%] | N = 1 [2.1%] |
| Smartwatches are convenient because most Afib patients already use one | N = 7 [14.6%] | N = 14 [29.2%] | N = 14 [29.2%] | N = 13 [29.2%] | N = 0 [0%] |
| Implantable Loop Recorder [ILR] | Smartwatch | Neither | Would recommend any without preference | |
| Which wearable rhythm monitoring device would you prefer to use in a patient with suspected paroxysmal Afib [recurrent, self-resolving episodes lasting < 7 days]? | N = 19 [39.6%] | N = 23 [48.0%] | N = 6 [12.5%] | N =0 [0%] |
| Which wearable rhythm monitoring device would you prefer to use in a patient with suspected persistent Afib [continuous for > 7 days]? | N = 14 [29.2%] | N = 25 [52.1%] | N = 9 [18.8%] | N = 0 [0%] |
| Which wearable rhythm monitoring device would you prefer in low-risk atrial fibrillation patients [CHAD2DS2-VASc < 1] on appropriate anticoagulation regimens? | N = 1 [2.1%] | N = 28 [58.3%] | N = 13 [27.1%] | N = 6 [12.5%] |
| Which wearable rhythm monitoring device would you prefer in moderate risk atrial fibrillation patients [CHAD2DS2-VASc = 1] on appropriate anticoagulation regimens? | N = 11 [23.0%] | N = 21 [43.8%] | N = 12 [25.0%] | N = 4 [8.3%] |
| Which wearable rhythm monitoring device would you prefer in high-risk atrial fibrillation patients [CHAD2DS2-VASc > 2] on appropriate anticoagulation regimens? | N = 16 [33.3%] | N = 14 [29.2%] | N = 13 [27.1%] | N = 5 [10.4%] |
| Which wearable rhythm monitoring device would you prefer for cardiac rhythm monitoring in patients with a history of stroke? | N = 30 [62.5%] | N = 10 [28.3%] | N = 6 [12.5%] | N = 2 [4.2%] |
| Strongly Agree | Agree | Neither Agree nor Disagree | Disagree | Strongly Disagree | |
| Accuracy of recorded data is a limiting factor | N = 7 [14.6%] | N = 20 [41.7%] | N = 15 [31.3%] | N = 5 [10.4%] | N = 1 [2.1%] |
| Cost of the device is a limiting factor | N = 20 [41.2%] | N = 19 [40.0%] | N = 8 [16.7%] | N = 1 [2.1%] | N = 0 [0%] |
| Sensitivity of recorded data is a limiting factor | N = 7 [14.6%] | N = 18 [37.5%] | N = 14 [29.2%] | N = 8 [16.7%] | N = 1 [2.1%] |
| Patient’s age is a limiting factor | N = 14 [29.2%] | N = 16 [33.3%] | N = 13 [27.1%] | N = 4 [8.3%] | N = 1 [2.1%] |
| Patient’s technological knowledge is a limiting factor | N = 21 [43.8%] | N = 18 [37.5%] | N = 5 [10.4%] | N = 4 [8.3%] | N = 0 [0%] |
| Patient’s adherence to usage is a limiting factor | N = 12 [25.0%] | N = 23 [47.9%] | N = 7 [14.6%] | N = 6 [12.5%] | N = 0 [0%] |
| Attitude Item | Subspecialized vs. Nonsubspecialized | Academia Affiliation vs. No Affiliation | ≤20 vs. >20 Years of Practice | <55 vs. ≥55 Years of Age |
| Identified as Limiting Factors | ||||
| Accuracy of recorded data | 0.0323 | 0.9378 | 0.4519 | 0.895 |
| Cost of the device | 0.5797 | 0.2561 | 0.4709 | 0.4806 |
| Sensitivity of recorded data | 0.5147 | 0.4023 | 0.5119 | 0.2407 |
| Patient’s age | 0.9001 | 0.9474 | 0.6864 | 0.8283 |
| Patient’s technological knowledge | 0.8138 | 0.7079 | 0.7102 | 0.7540 |
| Patient’s adherence to usage | 0.1334 | 0.7949 | 0.7451 | 0.6883 |
| Identified as Potential Benefits | ||||
| Smartwatches are reliable in detecting paroxysmal Afib in at-risk patients | 0.5799 | 0.6179 | 0.4272 | 0.4168 |
| Main benefit is detection of unapparent paroxysmal Afib | 0.8621 | 0.4511 | 0.4336 | 0.2383 |
| Smartwatches are unobtrusive in most patients’ lives | 0.9613 | 0.9534 | 0.6595 | 0.9174 |
| Smartwatches are convenient since most Afib patients already use one | 0.7420 | 0.5918 | 0.1012 | 0.3424 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac pacing and defibrillation studies · Cardiovascular Syncope and Autonomic Disorders · ECG Monitoring and Analysis
Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia, affecting over 33 million people worldwide [1]. With its incidence increasing with age, it affects around 1% of patients younger than 60 years and up to 8% of those 80 years or older [2]. AF is a supraventricular tachyarrhythmia characterized by uncoordinated aberrant atrial activation leading to decline of atrial mechanical function and thus, impairing physiologic cardiac function and increasing stroke risk [2]. Data from a 2001 study showed that AF has proven to have a significant economic burden with suggested United States hospitalization costs for non-valvular AF of 235 million for pharmacotherapy [3]. A more recent study found that patients with AF had significantly higher annual healthcare spending when compared with individuals without AF [4]. Currently, with the rise in the population age and the comorbid conditions, these numbers have gotten significantly higher. For instance, in 2016 alone, AF constituted $28.4 billion of the yearly US healthcare spending [5].
According to the American Heart Association/American College of Cardiology/Heart Rhythm Society guidelines on AF management, AF can be divided into four subtypes depending on their clinical forms: paroxysmal, persistent, long-standing persistent, and permanent [6]. Paroxysmal AF terminates spontaneously or with intervention within seven days of onset. Persistent AF fails to self-terminate within seven days of onset and often requires pharmacologic or electrical cardioversion to restore sinus rhythm. Long-standing persistent AF is a persistent AF that has lasted for more than 12 months. Permanent AF refers to an AF for which a joint patient-physician decision has been made not to pursue further attempts to restore or maintain sinus rhythm [6]. AF has a wide spectrum of clinical presentations which ranges from totally asymptomatic patients to those presenting with palpitations, dyspnea, fatigue, lightheadedness, and chest pain. More serious presentations can include stroke, heart failure, or hemodynamic instability [2]. These symptoms are highly non-specific and cannot be used to diagnose AF.
The diagnostic gold standard for AF is a 12-lead electrocardiogram [2]. The 12-lead ECG or a Holter ECG monitor might be too short for AF detection. Continuous AF ECG monitoring and implantable loop recorders (ILRs) are commonly being used due to their efficiency and accuracy at detecting AF. Smartwatches have gained attention as a possible noninvasive alternative for cardiac rhythm monitoring, leading the United States Food and Drug Administration to clear the device’s accuracy in detecting AF for pre-diagnostic purposes. At present, the FDA has recommended the use of various smartwatch algorithms (e.g., Apple, Samsung, Fitbit and Withings) for screening with required confirmation by 12-lead ECG prior to medical decision-making [7].
The use of smartwatches in the monitoring for AF is still a debated topic and few studies have sought to determine cardiologists’ opinions regarding the subject. Given the relatively novel nature of smartwatches as heart rhythm monitoring devices, it is important to gauge professional opinions, as this can better shed light on how guideline recommendations are used in clinical practice. Moreover, the data generated by this study can potentially be helpful to the medical industry in order to further optimize the function of their devices. The purpose of this study was to create data on the perception of Puerto Rican cardiologists on the use of smartwatches in the management of AF. In doing this, we sought to better characterize how cardiologists in Puerto Rico are adapting to the evolving landscape of modern cardiology. Through our survey study, we sought to compare smartwatches with more established long-term cardiac rhythm monitoring in the form of ILRs, to further understand how smartwatches' performance in AF is perceived. The rationale behind this decision was that both ILRs and smartwatches are relatively unobtrusive and potentially long-term monitoring devices. In addition, we explored the influence of various demographic (i.e., age and sex) and professional factors (ie, practice setting, association with academia, presence of subspecialty and comfort with AF management) on Puerto Rican cardiologists’ perception of the use of smartwatches for AF monitoring.
Materials and methods
In this cross-sectional study, a total of 48 eligible participants were recruited via email affiliation to the Puerto Rico Society of Cardiology (PRSC) and in-person attendance at the 30th annual Puerto Rico Congress of Cardiology (PRCC). Written consent and detailed instructions were included before initiating the survey questionnaire. This study was approved by the University of Puerto Rico-Medical Sciences Campus Institutional Review Board; protocol #2210058817.
Survey development
A digital questionnaire was developed by the researchers in collaboration with the University of Puerto Rico-Medical Sciences Campus Endowment Center for Investigation on Health Services (UPR-MSC ECIHS). The survey questionnaire encompassed six fields: Sociodemographic Information, physician’s experience with Afib and monitoring devices, perception about wearable devices, physician’s recommendations of wearable devices in different clinical scenarios, perceived potential of wearable devices, and considerations regarding smartwatch recommendations. The survey consisted of 34 independent items and six follow-up questions. Of these, 12 were multiple-choice questions, 16 were based on a 5-point Agreement Likert scale, and 12 were open-ended questions meant to be answered with a single number or word. Demographic information requested included: age, sex, medical practice setting, affiliation with academia, cardiology subspecialty, and years of practice. The utilized survey questionnaire is included in the Appendices section.
Survey distribution and administration
We opted for a survey that was initially sent via email to 300 addresses corresponding to cardiologists affiliated with the PRSC of which four complete responses were received. Given the inadequate number of responses received, the survey was subsequently presented in person to physicians who attended the 30th PRCC. Once the purpose of the survey study was explained to PRCC-affiliated physicians and informed consent was obtained, the agreeing participants were allowed to complete the survey independently. Participants considered for the study self-identified in the survey as cardiologists. One of the respondents self-identified as a cardiology fellow and was subsequently excluded from the study analysis. We ensured anonymity for the survey responders, and the statistician who conducted the analysis was completely blinded to any participant identifiers. Following survey distribution and removal of ineligible respondents, 48 participants were included in the statistical analysis. Figure 1 summarizes the recruitment process for this study.
Visual depiction of the survey questionnaire step-by-step administration process. PRSC: Puerto Rico Society of Cardiologists; PRCC: Puerto Rico Cardiology Congress.
Statistical analysis
After administration of the survey, the data was statistically analyzed by the UPR-MSC ECIHS. Descriptive statistics were first used to present a profile of the participants’ demographic and professional data, their exposure to AF patients, and their perceptions of wearable devices for cardiac monitoring. All participants completed the survey tool in its totality and appropriately answered all the questions provided. Attitudes were evaluated through Likert scales, and the non-parametric approach was chosen for their assessment. Subgroup analyses were performed based on respondent groups that varied by demographic and professional characteristics and had comparable sample sizes. The unadjusted relationship of these variables with having a self-reported cardiology subspecialty was gauged through the two-sample Wilcoxon-Mann-Whitney rank-sum test. The same approach was repeated for the other relevant variables for the characterizations of cardiologists; age of 55 or older, and more than 20 years of practice. Corrections for multiple comparisons were not performed as the number of comparisons was limited and directly related to the research question. For all tests, a p-value of 0.05 or less (p-value < 0.05) was considered an indicator of a significant difference. Statistical analysis was performed using Stata v14.2 (StataCorp, Texas, USA).
Results
A total of 49 Puerto Rican cardiologists responded to the survey tool. After removing a case found to be a fellowship trainee, the sample was composed of 48 participants. The demographic profile is shown in Table 1. The average age of respondents was 55.6 ± 12.4, while the ages ranged from 31 to 81. Forty-four respondents were male, while only four were female. A total of 38 respondents reported primarily working in their private office setting, while only 10 reported working primarily in a hospital setting. The average years practicing of all respondents was 21.7 ± 12.2, ranging from 1 to 44 years of practice. Nineteen respondents reported being affiliated with academia, while 29 were not affiliated with academia. A total of 12 respondents reported having an additional subspecialty, most of them being interventional cardiology (n = 6), followed by heart failure and transplant (n = 3). Figure 2 illustrates the distribution of cardiac sub-specialties based on survey-reported answers.
Distribution of cardiology sub-specialty based on participant self-reporting
The respondents’ perceptions regarding wearable devices, such as smartwatches and ILRs, are shown in Table 2. Several questions regarding wearable devices’ accuracy and reliability for detection of AF and cardiac rhythm monitoring were included in the questionnaire. Questions about possible benefits of smartwatches/ILRs in detecting paroxysmal and/or unapparent AF, convenience and unobtrusiveness were also included. The study participants successfully responded to all survey tool questions. Cardiologist attitudes were evaluated through Likert scale gradation. A high reported agreement is seen between participants on prompts referring to smartwatch accuracy in detecting AF and ILR accuracy in detecting AF, as well as both smartwatch accuracy and ILR accuracy. Notably, 81.1% of responding cardiologists agreed with the statement that smartwatches can accurately detect AF, whilst 93.7% of respondents agreed with the statement that ILRs can accurately detect AF. 87.5% of respondents agreed with the statement that ILRs are reliable alternatives for cardiac rhythm monitoring compared with 73% of respondents agreeing with the same statement when considering smartwatch use. Only 33.4% of participants agreed with the statement that smartwatches are equally as accurate as ILRs in the detection of AF. The majority of respondents to this question opted to answer Neither Agree nor Disagree (37.5%).
Some hypothetical scenarios were included in the questionnaire that asked respondents to choose between smartwatches, ILRs, neither of them, or if they would recommend any without a particular preference. The results are shown in Table 3. The hypothetical scenarios include preference of device in a patient with suspected paroxysmal AF (recurrent, self-resolving episodes lasting < 7 days) and in a patient with suspected persistent AF (continuous for > 7 days). Other hypothetical scenarios included preference of device for rhythm monitoring in a patient with an appropriate anticoagulation regimen with low-risk AF (defined as CHAD2DS2-VASc < 1), moderate-risk AF (CHAD2DS2-VASc = 1), high-risk AF (CHAD2DS2-VASc > 2), and in patients with a previous history of stroke. A greater proportion of Puerto Rican cardiologists would recommend monitoring with a smartwatch (48.0%) over an ILR (39.6%) for patients with paroxysmal AF. This trend was again repeated in hypothetical cases of persistent AF (52.1% favored smartwatches vs 29.2% favored ILRs). Smartwatches were also favored over ILRs in cases of low and moderate thromboembolic risk AF. ILRs were favored, however, in patients with suspected AF and a prior history of stroke (62.5% favored ILRs and 28.3% favored smartwatches). Cardiologists' preferences were more equally distributed when considering rhythm monitoring strategies in patients at high-risk of cardioembolic phenomena (33.3 % favored ILRs vs 29.2% favored smartwatches vs 27.1% favored neither). The findings reported might suggest a tendency to prefer ILRs in higher risk AF clinical scenarios (i.e., patients with higher CHAD2DS2-VASc scores or personal history of stroke).
Table 4 shows results about possible limiting factors that respondents might consider for the recommendation of smartwatches for monitoring AF. Limiting factors asked in the questionnaire included accuracy and sensitivity of recorded data, cost of device and patient’s age, technological knowledge, and adherence to use of device. The answers were evaluated through Likert scales. Notably, 56.3% of responding cardiologists identified the accuracy of smartwatches as a limiting factor to their use, with 31.3% favoring Neither Agree nor Disagree for this statement. Patient's technical knowledge and device cost seemed to be the most commonly perceived limiting factors for smartwatch use, with 81.2% and 81.3% of participants agreeing respectively. However, a greater proportion of participants favored Strongly Agree when considering patient's technical knowledge as a risk factor to smartwatch use (43.8%). Patient age and the sensitivity of recorded data were less commonly identified as limiting factors to smartwatch use (62.5% and 52.1%, respectively).
The two-sample Wilcoxon-Mann-Whitney rank-sum test p-value results for the four subgroup analyses are shown in Table 5. Values were assigned to each Likert scale gradation such that Strongly Agreed = 1, Agreed = 2, Neither Agree or Disagree = 3, Disagree = 4 and Strongly Disagree = 5. A subgroup median value was calculated from all the obtained responses and submitted to the non-parametric two-sample rank sum test in order to determine if there was a statistically significant difference between median values (p50). The only statistically significant difference between medians observed was between subspecialized and non-subspecialized cardiologists when considering if the accuracy of recorded data was a limiting factor to smartwatch use (p-value = 0.0323). The median value for the Likert scale answers for non-subspecialized cardiologists was 2 and 3 for specialized cardiologists, such that non-subspecialized cardiologists agreed with the statement that accuracy is a limiting factor to smartwatch use for cardiac monitoring more frequently. No other statistically significant differences were reported between subgroup means (p-value > 0.05).
Discussion
The Puerto Rican Society of Cardiology estimates its membership to be close to 325 cardiologists [8], of which close to 15% (N=48) are represented in this survey study. There is limited data on the demographic characteristics of Puerto Rican cardiologists. However, a recent study on the demographic characteristics of cardiologists in the United States evidenced a male preponderance of cardiologists [9], like what was observed in this study. The sample obtained in this survey study serves to attest to a relative underrepresentation of female cardiologists in Puerto Rico.
Moreover, the mean age of academic cardiologists in the continental United States has been estimated at 53.5 years for male cardiologists and 48.3 years for female cardiologists [10]. The mean age of the cardiologists who responded to this study was slightly older (55.6 ± 12.4). This discrepancy could reflect the existence of an older physician workforce in Puerto Rico. Although not its primary endpoint, this study has served to begin defining the baseline demographic characteristics of Puerto Rican cardiologists through participant self-reporting. Further studies are needed to better categorize the demographic characteristics of Puerto Rican cardiologists.
The general attitude of Puerto Rican cardiologists towards smartwatch use in AF monitoring was found to be positive. 81% of respondents attested that smartwatches can accurately detect AF. 73% of respondents agreed that smartwatches are reliable alternatives for most patients. Prior survey studies have suggested that physicians from various specialties have shown a considerable degree of confidence in smartwatches, as irregular pulse notifications often led to further diagnostic testing and interventions [11]. Of the 31 cardiologists surveyed in the aforementioned study, 41.9% had recommended smartwatch use to patients [11]. A survey study evaluating patient attitudes toward smartwatches in cardiac monitoring found that 68.9% of surveyed patients expressed an interest in smartwatch cardiac monitoring [12]. Additionally, 90% of interviewed patients said they would seek medical attention based on aberrant device readings [12].
The main benefit of smartwatch monitoring as perceived by Puerto Rican cardiologists appeared to be related to their continuous and relatively comfortable rhythm monitoring capacities. 89.6% of respondents agreed with the statement that there are unobtrusive rhythm monitoring alternatives for most patients. Moreover, 87.5% of responding cardiologists agreed with the statement that the main benefit of smartwatches lies in their capacity to reliably detect AF in at-risk patients. Although the impact AF burden has on thromboembolic events remains a contested topic, paroxysmal AF has been shown to increase the yearly risk of stroke and systemic embolization events. The Atrial Fibrillation Clopidogrel Trial with Irbesartan for Prevention of Vascular Events (ACTIVE W) has suggested a yearly stroke risk of 2% for patients with paroxysmal AF [13] while the Stroke Prevention in Atrial Fibrillation Study (SPAF) has suggested yearly stroke risks of 3.2% for patients with intermittent AF [14]. Thus, the detection of paroxysmal AF remains an important issue in stroke prevention and highlights the potential of smartwatch use in AF management.
When considering limitations of smartwatch use, the most frequently perceived factor by Puerto Rican cardiologists was device expense, with 82% of responding cardiologists identifying cost as a limiting factor to use. Smartwatches for cardiac monitoring are not currently covered by any major healthcare plan in Puerto Rico. Any patient interested in this form of rhythm monitoring must therefore pay out-of-pocket for the device. Evidently, this poses a barrier to healthcare access that may limit smartwatch cardiac monitoring to patients of higher socioeconomic status.
Patients’ technical knowledge was also frequently identified as a limiting factor to smartwatch use, with 81.3% of respondents agreeing with the statement. Moreover, 63.3% of responding cardiologists agreed that age is a limiting factor to smartwatch use. This fact is likely related to a supposition that older patients could be less technologically adept than younger patients. A survey on patient attitudes toward smart technology in cardiac rhythm monitoring found that 71% of its respondents identified the complexity of the technology as a limiting factor to its use [12]. Complexity was identified as a barrier to use particularly amongst older patients [12]. Conversely, younger patients (< 65 years) with underlying AF were more likely to be interested in smart device monitoring than older patients [12].
Although the majority of responding cardiologists responded favorably to the use of smartwatches in the detection of AF, 53% of respondents identified accuracy as a limiting factor to smartwatch use. Moreover, Wilcoxon-Mann-Whitney testing of subgroups only showed statistically significant differences between median values of the subgroup comparing subspecialized and non-subspecialized cardiologists (p = 0.0323; 3 and 2 respectively). Note that non-subspecialized cardiologists were found to identify the accuracy of smartwatches as a limiting factor more frequently than subspecialized cardiologists. This finding could be explained by exposure to novel technologies through additional training following a general cardiology fellowship. This difference could also be explained by increased professional exposure to smartwatch devices given the nature of electrophysiology practice or increased referrals from other medical specialties for arrhythmia detection or monitoring. Additionally, differential answering of this question could reflect differences in practice patterns. For example, one study found that electrophysiologists were more likely to employ long-term electrocardiogram monitoring when compared to non-electrophysiologist cardiologists [15]. Past survey studies have also found that patients may be apprehensive of smartwatch accuracy, with only 52% of patients trusting smartwatch accuracy [12]. Despite these findings, recent studies [16,17] have identified smartwatches as reliable alternatives with relatively high accuracy. A recent meta-analysis of 18 heterogeneous studies has found a pooled Positive Predictive Value and Negative Predictive Value of 85% and 100% respectively [18]. This could suggest that Puerto Rican cardiologists may underestimate the accuracy of smartwatches in arrhythmia detection and monitoring due to relative device novelty. Efforts through clinical training and continued medical education may be warranted to raise awareness on the usefulness of smartwatches for AF management.
When comparing smartwatches to ILRs, Puerto Rican cardiologists appeared to favor smartwatch use more strongly in lower risk patients (i.e., patients with lower CHA2DS2-VASc scores) than in higher risk patients (i.e., patients with higher CHA2DS2-VASc scores and history of strokes). This finding is likely explained by a belief that higher risk patients merit more invasive rhythm monitoring modalities. Such presumed attitudes may be reflective of recent professional guidelines where ILRs are recommended for secondary thromboembolic prevention in patients with inconclusive non-invasive monitoring [19]. However, smartwatch performance has been tested against more established methods of cardiac monitoring. One study compared the performance of the Garmin smartwatch to simultaneous Holter monitoring and reported a sensitivity of 97.3% and specificity of 88.6% [20]. These high sensitivity values could help establish smartwatches as reliable screening tools for the monitoring of AF. In patients with persistent AF, smartwatches have also been shown to accurately assess heart rates compared to Holter rates when < 110 bpm [21]. Note however, that there is limited data comparing the relative accuracies of smartwatches with ILRs for AF monitoring. Future prospective cohort studies can be aimed at determining how these two specific modalities compare in AF detection.
The performed survey study has various limitations. Firstly, of the estimated 300 members of the Puerto Rican Society of Cardiology, only 48 (15%) answered the survey study. A larger sample size would have allowed for a more representative sample with which to make more precise assumptions about Puerto Rican cardiologist's perception. Low response rate and possible response bias limit the generalizability of this study. Moreover, given the self-enrolling nature that is innate to survey studies, the cardiologists who chose to answer the survey could have stronger opinions toward smartwatches than those who chose not to answer the survey. The information analyzed was based on physician self-reporting and estimation. Additionally, four responses were obtained via email and 44 were obtained via voluntary in-person administration of the survey. There could have been differential responses based on the setting in which the survey was administered. These two population subsets were not individually analyzed. However, all attendees of the PRSC Conference are assumed to be members and may still constitute the originally intended study population. Moreover, we opted for a convenience sampling method which could have introduced bias into the methodology of our study. In-person completion of the survey may have also introduced bias from the Hawthorne effects, although participants were allowed to independently complete the survey and answers were collected anonymously. Statistical analyses were not adjusted for baseline demographic characteristics, but multivariable analysis allowed for gauging how these demographic factors impacted participants' answers. The administered survey was not pre-tested but was validated by the UPR-MSC ECIHS. Finally, only one of the cardiologists who responded to the survey study self-identified as a Clinical Electrophysiologist. Greater representation of this subspecialty would have been ideal given their expertise in cardiac rhythm monitoring.
Conclusions
This survey study has helped begin to define the baseline demographic characteristics of cardiologists in Puerto Rico. There may be a notable underrepresentation of the female sex amongst cardiologists in Puerto Rico. Given high agreement rates on Likert Scale questionnaires, there is a tendency towards favorable attitudes regarding the use of smartwatches in atrial fibrillation monitoring amongst Puerto Rican cardiologists. Notably, study's generalizability is limited given low response rates. The main perceived benefit of these devices is their capacity to provide continuous cardiac monitoring in a relatively unobtrusive manner. The most frequently identified limitation for smartwatch use in cardiac rhythm monitoring was the cost of the device. Patient’s technical knowledge was also frequently identified as a barrier to smartwatch use. There was a tendency to prefer ILR use over smartwatch use in high-risk patients based on Likert Scale questionnaire answers. The only significant difference in the distribution of respondent attitude questions was observed regarding the accuracy of smartwatches within the subspecialized vs non-subspecialized respondent cardiologists. Subspecialized cardiologists identified device frequency as a barrier to use less frequently than non-subspecialized cardiologists. This discrepancy may be explained by possible exposure to novel technologies through additional training. The findings of this study highlight the need for continued education of cardiology professionals regarding novel cardiac monitoring technologies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stroke and thromboembolism prevention in atrial fibrillation Heart Jame S Barnes G 101710620203153399010.1136/heartjnl-2019-314898 PMC 7881355 · doi ↗ · pubmed ↗
- 2Atrial fibrillation: diagnosis and treatment Am Fam Physician Gutierrez C Blanchard DG 6168832011 https://www.aafp.org/pubs/afp/issues/2011/0101/p 61.html 21888129 · pubmed ↗
- 3Assessing the direct costs of treating nonvalvular atrial fibrillation in the United States Value Health Coyne KS Paramore C Grandy S Mercader M Reynolds M Zimetbaum P 348356920061696155310.1111/j.1524-4733.2006.00124.x · doi ↗ · pubmed ↗
- 4Healthcare expenditure on atrial fibrillation in the United States: the Medical Expenditure Panel Survey 2016 to 2021 JACC Adv See C Grubman S Shah N Hu JR Nanna M Freeman JV Murugiah K 101716420254028637210.1016/j.jacadv.2025.101716 PMC 12103078 · doi ↗ · pubmed ↗
- 5Atrial fibrillation: JACC Council perspectives J Am Coll Cardiol Chung MK Refaat M Shen WK 168917137520203227303510.1016/j.jacc.2020.02.025 · doi ↗ · pubmed ↗
- 6AHA/ACC/HHS strategies to enhance application of clinical practice guidelines in patients with cardiovascular disease and comorbid conditions: from the American Heart Association, American College of Cardiology, and US Department of Health and Human Services Circulation Arnett DK Goodman RA Halperin JL Anderson JL Parekh AK Zoghbi WA 1662166713020142521246610.1161/CIR.0000000000000128 PMC 10966981 · doi ↗ · pubmed ↗
- 7Wearable digital health technologies for monitoring in cardiovascular medicine N Engl J Med Spatz ES Ginsburg GS Rumsfeld JS Turakhia MP 34635639020243826564610.1056/NEJ Mra 2301903 · doi ↗ · pubmed ↗
- 8Sobre nosotros: Conoce la Sociedad 3 2024 Jordan Jordan EE 2024 https://www.cardiologiapr.org/quienes-somos/