Radiation dosimetry and fasting-dependent hepatobiliary clearance of the VAChT-specific PET radioligand 18F-VAT in humans
Scott A. Norris, Noah L. Goldman, Mahdjoub Hamdi, Stephen M. Moerlein, Richard Laforest, Morvarid Karimi, Joel S. Perlmutter, Zhude Tu

TL;DR
This study examines how the PET radioligand 18F-VAT is distributed and cleared in the human body, focusing on the impact of fasting on radiation exposure.
Contribution
The study provides new human dosimetry data for 18F-VAT and shows how fasting affects gallbladder radiation exposure.
Findings
18F-VAT accumulates mainly in the brain, hepatobiliary system, small intestine, bone, and urinary bladder.
Fasting significantly affects gallbladder radiation exposure, with partial fasting allowing higher safe doses.
Human dosimetry data differ from pre-clinical models due to gallbladder retention not observed in rats.
Abstract
The vesicular acetylcholine transporter ligand (-)-(1-((2R,3R)-8-(2-[(18)F]fluoro-ethoxy)-3-hydroxy-1,2,3,4-tetrahydronaphthalen-2-yl)piperidin-4-yl)(4-fluorophenyl)-methanone (18F -VAT) enables positron emission tomography PET quantification of cholinergic dysfunction in neurologic and psychiatric disorders. Determining its bio-distribution and dose exposure in humans is essential for clinical implementation, particularly given hepatobiliary clearance observed in pre-clinical models. Based on pre-clinical data, eight healthy subjects (4 males, 4 females) received 385–533 MBq 18F-VAT immediately followed by three sequential whole-body PET/CT scans. PET data were collected under three different fasting conditions relative to administration of Ensure®Plus oral supplement and PET image acquisition: (1) complete fasting (n = 3), (2) oral partial fasting (n = 3), or (3) non-fasting (n = 2).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
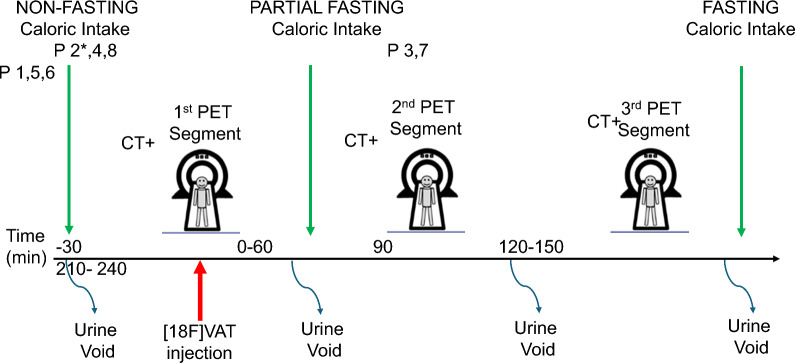 Figure 1
Figure 1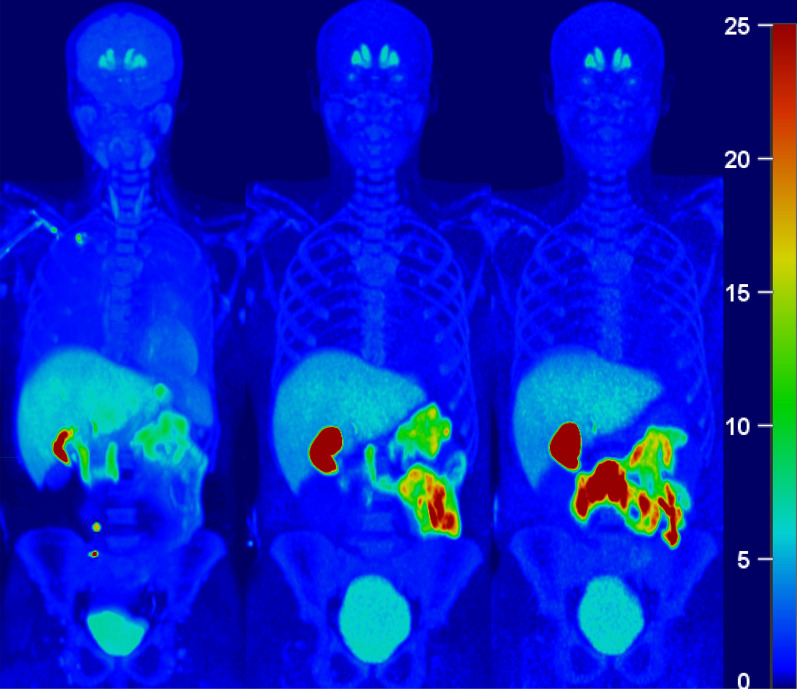 Figure 2
Figure 2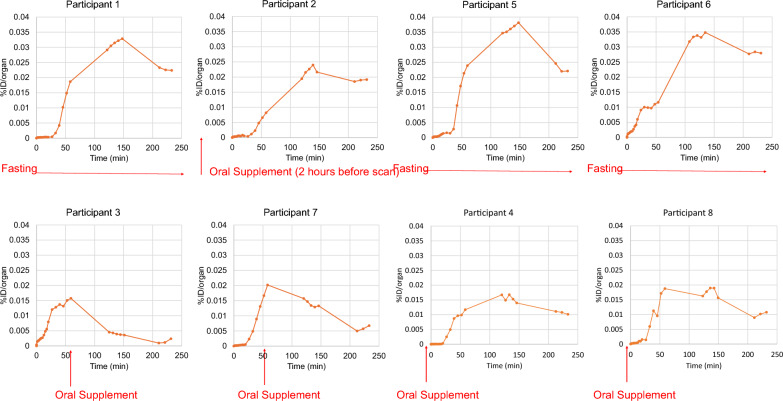 Figure 3
Figure 3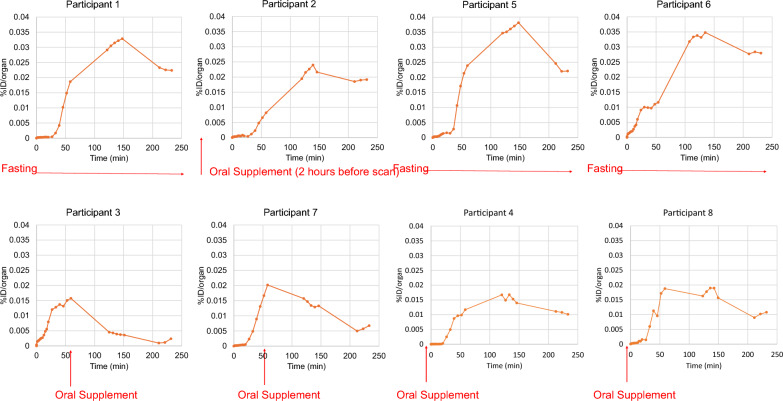 Figure 4
Figure 4- —http://dx.doi.org/10.13039/100000002National Institutes of Health
- —http://dx.doi.org/10.13039/100013928Dysphonia International
- —http://dx.doi.org/10.13039/100007338Foundation for Barnes-Jewish Hospital
- —http://dx.doi.org/10.13039/100006309American Parkinson Disease Association
- —http://dx.doi.org/10.13039/100018866Paula and Rodger Riney Foundation
- —Jo Oertli Fund
- —Murphy Fund
- —N. Grant Williams
- —American Parkinson Disease Association Advanced Center at Washington University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNicotinic Acetylcholine Receptors Study · Cholinesterase and Neurodegenerative Diseases · Neuroscience and Neuropharmacology Research
Background
Acetylcholine, a key neurotransmitter in the central nervous system, is synthesized in nerve terminals by choline acetyltransferase (ChAT) and transported into synaptic vesicles via the vesicular acetylcholine transporter (VAChT) protein [1]. Both ChAT and VAChT are highly expressed in cholinergic neurons [2] that are implicated in various neurologic and psychiatric disorders [3–5]. Imaging techniques like single-photon emission computed tomography (SPECT) [6] and positron emission tomography (PET) [7, 8] using cholinergic radiotracers can quantify the regional distribution of cholinergic neurons in the human brain. The PET ligand vesicular acetylcholine transporter ((-)-(1-(-8-(2-fluoroethoxy)-3-hydroxy-1,2,3,4-tetrahydronaphthalen-2-yl)piperidin-4-yl)(4-fluorophenyl)-methanone) (^18^F-VAT), a high-affinity VAChT ligand, shows substantial promise for assessing VAChT density and function [9–13] (Jin et al., 2018) [14].
Accurate assessment of ^18^F-VAT radiation dosimetry in humans is important for safe and effective use in research and potential clinical settings. Prior studies have used rat bio-distribution data to predict human dosimetry [12]. However, this may be inadequate because ^18^F-VAT uptake is highest in the hepatobiliary system, and rats lack a gallbladder, which is crucial for hepatobiliary tracer clearance in humans. Other studies obtained dosimetry estimation of ^18^F-VAT in fasting, anesthetized non-human primates, revealing high localization in the liver consistent with hepatobiliary clearance [15]. While prior non-human primate studies may better predict human dosimetry than rat studies, no studies have directly addressed the safety profile or effects of fasting state on hepatobiliary clearance of the ^18^F-VAT radiotracer in humans. The primary objective of this study is to determine the maximum safe dose of ^18^F-VAT in humans; specifically accounting for the potential role that a fasting state may have on hepatobiliary clearance of this tracer. These data may allow clinical investigators to optimize ^18^F-VAT PET imaging protocols in humans, following federal regulations for dosimetry and supporting translational research. Such knowledge may specifically facilitate longitudinal studies that explore the role of VAChT in neurodegenerative disorders, and potentially pave the way for development of novel diagnostic tools and therapeutic interventions.
Methods
Study design and participants
The Washington University Institutional Review Board and Radioactive Drug Research Committee approved this study (#201501149) performed under FDA Investigational New Drug Application #125627. All participants provided written informed consent prior to inclusion. The dosimetry cohort included eight healthy volunteer participants (4 female, 4 male, age 23–67) who underwent whole-body PET/CT imaging. Inclusion criteria were any sex or race, age greater than 18 years, and ability to provide written informed consent. Criteria for exclusion consisted of any diagnosed neurological disease, active pregnancy (urine pregnancy test to exclude), actively breastfeeding, current exposure to clinical radiation therapy or a research PET scan within 12 months, any exposure to drugs that block dopamine receptors, CNS active medications that affect dopaminergic or cholinergic systems three days prior to study, history of addiction, active depression, psychotic illness, cognitive impairment (Montreal Cognitive Assessment < 26), history of unstable general medical condition, and weight over 300 pounds.
Radiopharmaceutical preparation
^18^F-VAT was prepared under cGMP conditions done in the Mallinckrodt Institute of Radiology Cyclotron Facility and Nuclear Pharmacy at Washington University School of Medicine as previously described [14, 16]. In brief, [^18^F]fluoroethyl tosylate was produced using an Eckert and Ziegler Modular-Lab system [12, 17, 18] and [^18^F]VAT was synthesized with the GE TRACERlab FX-N module as [^18^F]fluoroethyl tosylate reacted with the corresponding enantiomerically pure phenol precursor. The drug substance was purified by reverse phase HPLC, and the parenteral product was sterilized by membrane filtration and reformulated in 10% ethanol in 0.9% Sodium Chloride Injection, USP. The sterile, apyrogenic product met a battery of pre-release quality control tests, including radiochemical purity > 99%, injected mass of VAT < 5 μg, and specific activity > 111 GBq/μmol.
PET/CT data acquisition
The height and weight of each participant was recorded prior to scan. Given prior pre-clinical studies indicating hepatobiliary clearance of ^18^F-VAT, we designed the study to include ^18^F-VAT administration and multiple whole-body PET acquisitions (i.e., segment) in three different fasting states as described here: (1) “complete fasting”: after overnight fasting, ^18^F-VAT administration and three whole-body PET segments, (2) “partial fasting”: after overnight fasting, ^18^F-VAT administration plus one PET whole-body segment followed by Ensure® Plus oral supplementation and two PET segments, and (3) “non-fasting” after overnight fasting, Ensure® Plus oral supplementation immediately prior to ^18^F-VAT administration followed by three whole-body PET segments. For the complete fasting state, participants #1, #2, #4 and #5 were instructed to fast at midnight prior to the study day through the end of the PET scan. One participant (#2) consumed a small breakfast consisting of milk and cereal due to discomfort, approximately 2 h prior to PET scan- this participant is thus considered “partial fasting” henceforth. For the intended partial fasting state, participants #3 and #7 fasted at midnight prior to the study day, until they consumed oral Ensure® Plus between PET segments one and two (see below). In the non-fasting state, participants #4 and #8 fasted at midnight prior to study day, then consumed oral Ensure® Plus in the 30 min prior to ^18^F-VAT administration and all subsequent PET scans.
All participants voided their bladder before^18^F-VAT administration and the PET imaging session. A 22-gauge plastic catheter was inserted into the right antecubital vein to permit radiotracer administration. We used surgical tape to secure the head position of the awake participant. PET data were obtained using a Siemens Vision Biograph PET/CT (Siemens Healthineers, Knoxville TN, USA) with participants scanned in the supine position at rest for three independent whole-body dynamic PET segments. Prior to each individual PET segment, a topogram was obtained (35mAs, 120 kV) followed by low-dose spiral CT scan for attenuation correction (50mAs effective, 120 kV) covering from the top of the skull through the upper thighs. Immediately after the first attenuation CT scan, three dynamic PET segments were similarly obtained from the top of skull through the upper thighs beginning at initiation of a 20 s bolus IV injection of ^18^F-VAT (389–533 MBq, 10.5–14.4 mCi) followed by immediate saline flush of the intravenous catheter. The first PET segment (sequential whole body [WB] scans 1 to 17) began with the start of the bolus injection and lasted for approximately 60 min (time per whole body scan was 60 s [WB 1–5], 120 s [WB 6–10], and 360 s [WB 11–17], respectively). Participants #3 and #7, in the partial fasting group, consumed oral Ensure® Plus in the 30 min prior to the second PET segment. The second PET segment (WB 18–22) started 2 h post-injection, collecting 360 s per whole body scan. The third PET segment (WB 23–25) started 3.5 h post-injection, collecting 600 s per whole body scan. All participants exited the PET scanner between segments and were offered an opportunity to void their bladder. This procedure aimed to enhance comfort and reduce the risk of disrupting subsequent PET sequence due to a sudden urge to void. All participants were allowed to eat immediately following completion of the third and final PET segment. Figure 1 represents the study sequence across participants.Fig. 1. Timeline of study day events around PET data acquisition
PET/CT image reconstruction
For the purpose of image reconstruction, the low-dose CT performed before each PET segment provided attenuation correction and anatomical information. Whole-body PET scan images were reconstructed using the ordered subset expectation maximization (OSEM) algorithm with time of flight (TOF) and point spread function (PSF) resolution modeling (4 iterations and 5 subsets) with no post-reconstruction filtering. The reconstruction resolution was 1.65 × 1.65 × 3-mm and included corrections for scatter, randoms, and attenuation based on CT. We inspected images for evidence of motion, and alignment was manually corrected, if needed.
VOIs
Three-dimensional volumes of interest (VOIs) were manually traced using MIM® software (version 6.9.3) over source organs with measurable activity, defined as signal increase above background levels sufficient to allow visual recognition: brain, lungs, heart (wall and left ventricle), liver, gallbladder, spleen, small intestine, kidneys, urinary bladder, and the lumbar vertebrae (L1–L3). Organs with well-defined boundaries were contoured in their entirety (e.g., liver and kidneys). Organs with complex boundaries (e.g., small bowel) were sampled and activity scaled to the estimated mass of the organ. To address intra-scan motion, we analyzed the tracer distribution within identified VOIs across all acquired frames for each PET segment. If the VOIs did not accurately estimate tracer uptake in the targeted organ for all frames, a new VOI was delineated to better represent the biodistribution within the respective organ for affected frames.
Radiation dosimetry
Time-activity curves (TAC) were obtained for each source organ by calculating the total activity in the organ-specific VOIs and expressing them as the percentage of the total injected activity. Given the time-course of activity in a volume of tissue, residence times, or normalized cumulated activity, were then calculated with the trapezoid method, except for the bladder as described below. We elected to apply the trapezoid method to avoid overfitting data in context of unevenly and undersampled sampled data between PET segments, and as we observe narrow peaks in time activity curves for some VOIs. Specifically, given an activity A_0_ (injected dose) applied to a participant, and measured (not decay corrected) A(t) in an organ, the residence time τ is calculated by:
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\uptau =\frac{{\int }_{0}^{\infty }A\left(t\right)dt}{{A}_{0}}$$\end{document}Calculated residence time values were entered into the OLINDA/EXM 2.2 software package [19] for F-18 using the adult human male and female anthropomorphic models as done in prior work [20–23] to generate the organ radiation dose.
For the bladder, the cumulative activity was fitted by an uptake function of the form:
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\text{F}(\text{t}) =\text{ A}0*(1-1{\text{e}}^{\left(-\text{A}1\bullet \text{t}\right)})$$\end{document}where A0 and A1 were fitting parameters representing the filling fraction and filling constant. For dosimetry modeling, the urinary bladder was assumed to be voided every 2 h, consistent with the study protocol in which participants were instructed to void prior to each PET session. This assumption was implemented in the OLINDA bladder model to best reflect the conditions under which activity accumulation was observed and measured.
The time-integrated activity is calculated by:
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\ A = \mathop \smallint \limits_{0}^{\infty } A\left( t \right)dt$$\end{document}Results
Participant demographics and administered dose
Table 1 displays demographic and radiopharmaceutical dosing information for the four ^18^F-VAT participants.Table 1. Participant demographicsParticipantSexHandednessAge (yr)Height (m)Weight (kg)PET fasting groupInjected dose (MBq)1FemaleRight641.6388Complete fasting5182FemaleRight641.63103.3Partial fasting5253FemaleRight381.6558.2Partial fasting3894FemaleRight281.6596.2Non-fasting5075MaleRight271.7570.3Complete fasting5336MaleRight231.9194.8Complete fasting5337MaleRight501.7872.6Partial fasting5198MaleRight671.6372.6Non-fasting514Despite intent for complete fasting, this participant consumed a small breakfast of milk and cereal approximately 2-h before ^18^F-VAT administration and PET acquisition due to discomfort
Adverse events
There were no adverse or clinically detectable effects observed or reported following ^18^F-VAT administration in any participant. No participant reported injection site reactions or any other symptoms during the procedure, throughout the duration of the 4-h scan, or in telephone follow-up one day after the PET scan.
Human biodistribution
Figure 2 shows the whole-body PET data averaged for each of three segments in participant 4 fused onto the corresponding CT scan. This representative image demonstrates significant radioligand uptake in the muscle, liver, gallbladder, small intestine, urinary bladder, as well as brain (specifically in the caudate and putamen). High activity was observed in the liver at early time points whereas the gallbladder and small intestine had higher activity at later time points, compatible with hepatobiliary excretion. Minimal activity was observed in the kidneys despite accumulation in the urinary bladder.Fig. 2. Participant #6 maximum intensity coronal projection (MIP) of all PET frames in the A first, B second, and C third PET segments with decay-corrected standard uptake values (SUV) demonstrating high uptake in the muscle, liver, gallbladder, small intestine, urinary bladder, as well as brain
Time-activity curves
We calculated TACs in organs with measurable activity from the PET images. Figure 3 shows TACs compiled for a single representative non-fasting participant (#4).Fig. 3. Non-decay-corrected organ time-activity curves for participant 6. %ID = percentage injected dose
We observed a rapid accumulation and slow clearance of activity in muscle, lung, and brain, with initial fractions at ~ 18%, ~ 15%, and 4% of the injected dose, respectively. The liver and gallbladder reflected a delayed accumulation of ~ 25% and ~ 5%, of injected dose, respectively. For the liver, peak accumulation occurred at approximately 35 min after injection, followed by a slow clearance.
Effect of feeding on gall bladder accumulation
As shown in Fig. 4, for subjects in the fasting group (1. 5. 6), the gallbladder accumulated radioactivity throughout the course of PET image acquisition, demonstrating a 20% increase of combined TAC data of segments 2 and 3 compared to segment 1. This accumulation effect was reversed in the two participants in the partial fasting group (3 and 7), in which there was a 59% decrease of the integrated TAC of combined segments 2 and 3 compared to segment 1. For the non-fasting subjects (4 and 8), there was no substantial accumulation of radioactivity in the gallbladder, and the TAC for segments 1–3 were low and not substantially different.Fig. 4. Non-decay corrected gallbladder TACS for individual participants. Red text describes fasting versus non-fasting states, where the time of oral supplementation is indicated relative to PET data acquisition. Note trends of increasing TAC across PET segments in the fasting state (participants 1,5,6), reduction in TAC following oral supplementation when administered between PET segments 1&2 (participants 3,7) and reduced overall TAC when oral supplementation is administered prior to PET acquisition (participants 4 and 8). Participant #2 was intended to fast but had a small mean 2 h prior to PET acquisition
Time integrated activity
Time integrated activity was calculated for all organs (Tables 2, 3, 4, 5). The organ with the greatest time integrated activity time was the muscle tissue followed by liver, bone marrow and gallbladder, while the smallest were the kidneys. The low standard deviation on the time integrated activity for all organs suggests good reproducibility. Mean gallbladder time integrated activity differed significantly between the fasting group (74.1 MBqh) and the combined non-fasting (36.6 MBqh), and partial fasting (21.8 MBqh) groups (Kruskal–Wallis H 6.5, p = 0.03).Table 2. Time-integrated activity of female participants in MBqParticipant numberSite12^†§^3^†^4^‡^Brain56.938.731.424.6Lungs13.617.910.326Heart22.313.59.25.3Blood LV9.915.64.84Liver155.699.3214.2186Gallbladder72.755.112.333.5Spleen18.24.14.75.7Small Intestine37.23671.436.8Kidneys9.38.36.97.5Bladder6.713.228.138.8Bone Marrow6.737.95846.9Muscle273.4226.9125147.1Remainder665.8802.2436.4681.4Complete fasting^†^Partial fasting^‡^Non-fasting^§^intent was complete fasting, but participant elected to eat 2-h prior to 18F-VAT injection/PET acquisition due to general discomfortTable 3Time-integrated activity of male participants in MBqParticipant numberSite567^†^8^‡^Brain37.335.933.838.3Lungs29.312.715.226.5Heart12.28.715.810.5Blood LV138.24.58.8Liver183.6158.4300.9232.5Gallbladder81.387.431.439.8Spleen75.86.78.4Small Intestine45.233.158.479.1Kidneys10.47.66.55.9Bladder21.211.537.529.7Bone Marrow48.939.347.474.5Muscle279.6224.8446.1453.1Remainder616.5757.8352.2337.4Complete fasting^†^Partial fasting^‡^Non-fastingTable 4Time-integrated activity in MBq averaged across all participants and non-fasting groupSiteMean all participantsSDMean non-fastingSDBrain37.19.331.49.7Lungs18.97.326.20.3Heart12.25.27.93.6Blood LV8.64.26.43.4Liver191.359.9209.232.9Gallbladder51.726.836.64.5Spleen7.64.57.11.9Small Intestine49.617.857.929.9Kidneys7.81.56.71.1Bladder23.312.134.36.4Bone Marrow4519.360.719.5Muscle272122.3300.1216.4Remainder581.2181.8509.4243.2Table 5Time-integrated activity in MBq averaged across partial-fasting and fasting groupSiteMean partial-fastingSDMean fastingSDBrain32.61.742.29.9Lungs12.83.518.47.6Heart12.54.614.25.8Blood LV4.70.211.73.3Liver257.561.3149.235.6Gallbladder21.813.574.114Spleen5.71.48.86.4Small Intestine64.99.237.95.2Kidneys6.70.38.91.2Bladder32.86.613.26Bone Marrow52.77.533.218.3Muscle285.5227.1251.229.4Remainder394.359.6710.684.6
Dosimetry
Dosimetry data for individual participants, averaged across all participants, males, females, and the two non-fasting participants are presented in Tables 6, 7 and 8. These data reflect effective dose for human adults. The dose-limiting organ was the gallbladder with a mean dose across all participants of 201.0 ± 80.4 µSv/MBq followed by the liver at 64.3 ± 18.4 µSv/MBq. The critical organ mean dose was similar across males (213.0 µSv/MBq) and females (189.0 µSv/MBq). The mean effective dose was 17.5 ± 2.1 µSv/MBq (15.7 µSv/MBq for males and 19.4 µSv/MBq for females). In this most conservative calculation, an injected dose of 249 MBq (6.7 mCi) would yield a total effective dose of 4.36 mSv (0.436 rem) with the critical organ, the gallbladder, receiving the maximum allowed exposure of 50 mSv (5 rem). A peri-procedural oral caloric bolus between PET segments 1 and 2 reduced the overall radiation of the gallbladder to 107.6 µSv/MBq (398.1 mrem/mCi) averaged across two participants of different genders. A pre-procedural oral caloric bolus prior to PET session reduced the overall radiation of the gallbladder to 155.5 µSv/MBq (575.4 mrem/mCi) averaged across two participants of different genders. In this situation, up to 465 MBq (12.6 mCi) of [^18^F]VAT can be administered to human participants without exceeding a maximum dose to the gallbladder of 50 mSv (5 rem).Table 6. Radiation dosimetry (μSv/MBq) across all participantsParticipant numberSiteFemaleFemaleFemale^†^Female^‡^MaleMaleMale^†^Male^‡^12345678Adrenals27.921.427.525.121.120.123.522Brain22.416.217.112.113.513.112.414.1Breasts10.610.99.8110.6Esophagus15.914.916.315.613.212.613.213Eyes11.511.59.7210.38.59.017.518.05Gallbladder Wall29222186.1157276293129154Left colon19.218.617.717.314.914.814.415.7Small intestine38.136.9713934.429.140.751.5Stomach wall17.316.216.616.514.113.813.913.9right colon19.81918.918.619.820.117.518Rectum14.216.214.615.61212.411.812.3Heart wall42.934.228.719.326.12027.423.7Kidneys2722.82724.321.818.31918Liver57.939.396.170.954.548.481.566Lungs14.314.91518.815.510.812.715.3Ovaries15.116.315.315.7Pancreas23.821.225.923.417.116.717.718Prostate11.61211.611.4Salivary Glands11.812.110119.7510.38.629.18Red marrow22.421.224.82116.215.115.819.6Osteogenic cells16.516.216.815.613.713.412.915.3Spleen5719.826.125.522.819.922.226.5Testes8.779.437.948.13Thymus14.214.512.613.611.711.210.711Thyroid11.412.110.211.510.110.38.969.48Urinary Bladder wall13.625.927.529.117.815.232.921Uterus1516.916.416.4Total body15.214.815.21511.411.61111.3Effective dose19.918.32019.3161515.715.9Participant elected to eat 1 h prior to the first PET scan due to general discomfort while fasting†Participant received PO Ensure®Plus 8-oz bolus during the PET session (between scan 1 and 2)‡Participant received PO Ensure®Plus 8-oz bolus prior to the PET sessionTable 7Radiation dosimetry (μSv/MBq) across genderSiteAverage all participants (± SD)Gender MeanSDMaleSDFemaleSDAdrenals23.6321.71.425.53Brain15.13.413.30.7174.2Breasts10.50.5Esophagus14.31.5130.315.70.6Eyes9.51.58.30.610.80.9Gallbladder wall20180.421383.518988Left colon16.61.9150.518.20.9Small Intestine42.613.138.99.646.316.5Stomach Wall15.31.513.90.116.70.5Right Colon190.918.91.319.10.5Rectum13.61.712.10.315.20.9Heart wall27.87.824.33.331.39.9Kidneys22.33.719.31.725.32.1Liver64.318.462.614.666.123.9Lungs14.72.313.62.215.82.1Ovaries15.60.5Pancreas20.53.617.40.623.61.9Prostate11.70.3Salivary Glands10.31.29.50.711.20.9Red Marrow19.53.516.7222.41.7Osteogenic Cells15.11.513.8116.30.5Spleen27.512.222.92.732.116.8Testes8.60.7Thymus12.41.511.20.413.70.8Thyroid10.51.19.70.611.30.8Urinary Bladder Wall22.9721.77.8247.1Uterus16.20.8Total body13.2211.30.315.10.2Effective dose17.52.115.70.519.40.8Table 8Radiation dosimetry (μSv/MBq) across fasting conditionSiteNon-fastingSDFasting participantsSDPartial-fasting participantsSDparticipantsmeanmeanmeanAdrenals23.62.222.63.625.52.8Brain13.11.416.34.314.83.3BreastsEsophagus14.31.814.21.514.82.2Eyes9.21.610.11.68.61.6Gallbladder wall155.52.1270.533.9107.630.3Left colon16.51.116.92.416.12.3Small Intestine45.38.834.6455.921.4Stomach Wall15.21.815.41.715.31.9Right Colon18.30.419.70.518.21Rectum142.313.71.913.22Heart Wall21.53.130.89.928.10.9Kidneys21.24.522.53.6235.7Liver68.53.5508.288.810.3Lungs17.12.513.92.113.91.6OvariesPancreas20.73.819.73.421.85.8ProstateSalivary glands10.11.3111.19.31Red marrow20.3118.73.620.36.4Osteogenic cells15.50.2151.614.92.8Spleen260.729.918.124.22.8TestesThymus12.31.812.91.711.71.3Thyroid10.51.4110.99.60.9Urinary bladder wall25.15.718.15.530.23.8UterusTotal body13.22.613.3213.13Effective dose17.62.417.32.217.93
Discussion
We have described the regional distribution of ^18^F-VAT binding in eight healthy human volunteers with no evidence of neurologic or psychiatric disease. No adverse reaction was observed during whole-body PET scans of ^18^F-VAT to acquire data for human dosimetry assessment. Our data in healthy humans identifies the gallbladder as the critical organ, with its radiation burden varying depending on fasting status. When averaged across all participants in various fasting conditions the overall radiation burden to the gallbladder wall was 201.0 µSv/MBq (502 mrem/mCi); the second highest radiation dose is delivered to the liver which received an average of 64.3 µSv/MBq (188 mrem/mCi). Without accounting for fasting state, our organ dosimetry thus indicate that suitable doses of ^18^F-VAT can safely be administered to obtain PET imaging data where the calculated effective dose was 15.7 and 19.4 µSv/MBq for males and females, respectively. Specifically, the radiation exposure from a single dose of 249 MBq (6.7 mCi) or less avoids exceeding a gallbladder radiation dose of 50 mSv (5 rem). When comparing fasting, partial fasting, and non-fasting states, post-injection greater than pre-procedural oral caloric supplementation increases gallbladder clearance, thus reducing gallbladder wall radiation burden and allowing a higher administered dose to 465 MBq (12.6 mCi) without exceeding a gallbladder dose of 50 mSv (5 rem). These data indicate that oral caloric supplementation approximately 90 min after ^18^F-VAT injection can reduce the gallbladder wall radiation exposure, i.e., the critical organ, which is particularly important when higher radiotracer doses or multiple PET studies are desired in the same individual.
The observation of hepatobiliary clearance is consistent with a prior fasting non-human primate dosimetry study demonstrating that the critical organ is the liver [15]. This human cohort represents a 6.5-fold greater gallbladder wall radiation dose and longer residence time compared to that previously estimated from two non-human primates (mean 0.100 ± 0.048 h in humans versus 0.01 ± 0.0008 h in non-human primates). Despite this difference in gallbladder wall dosimetry, the liver dosimetry and residence time remained nearly equivalent across species. Discrepancies in the gallbladder dosimetry values across species may reflect variable hepatobiliary clearance rates secondary to dietary features, especially since all nonhuman primates were strictly fasted overnight and throughout 6 h PET procedures. Overall dietary lipid content, relative fasting state, etc., [24], or anesthesia may also influence hepatobiliary excretion of the radioligand in NHPs. Our observations that gallbladder radioactivity accumulation was reduced when ^18^F-VAT was given to non-fasting subjects, as well as by as much as 59% in following inter-PET segment oral caloric supplementation supports the conclusion that non-fasting state reduces the overall gallbladder wall residence time and radiation burden.
The effective dose (E) for ^18^F-VAT (averaged across genders) is 17.5 µSv/MBq (65 mrem/mCi), which does not appreciably limit ^18^F-VAT doses when performing PET studies of human participants. Injection of the maximum partial-fasting 465 MBq (12.6 mCi) dose of ^18^F-VAT would deliver a whole-body dose of only 8.1 mSv (0.81 mrem). This is well below the typical whole-body limit of 30 mSv (3 rem). The average E in these human studies and in prior PET studies of NHP was in good agreement (17.5 mSv/MBq and 14.1 mSv/MBq, respectively).
In the partial and non-fasters there was relatively elevated radiation dose to the small intestines, supporting the hypothesis that a normal physiologic response to oral fat intake, namely increased ejection of stored bile in the gallbladder is the mechanism for our findings. Together, our observations suggest that ^18^F-VAT clears through the hepatobiliary system at variable rates based on fasting state, and that oral ingestion following radiotracer injection reduces overall radiation dose to the gallbladder wall. These data suggest that ^18^F-VAT PET studies should be performed with oral supplementation following injection of the tracer (e.g., 20 ml of high-fat emulsion following ^18^F-VAT injection [25]) to reduce relative radioactive dose to the critical organ. While our data demonstrates a significant effect following oral supplementation 90 min after ^18^F-VAT injection, our study was not designed to identify the optimal post-injection timing of oral supplementation in reducing critical organ radiation.
Additional data in male Sprague Dawley Rats support the notion that the hepatobiliary system represents the highest ^18^F-VAT regional uptake [12]. However, since rats do not have a gallbladder [26] biodistribution studies in rats can be misleading for radiotracers in which the gallbladder is the critical organ in humans. An additional species differences relates to reduced relative renal ^18^F-VAT uptake in humans and non-human primates compared to rats. Thus, dosimetry studies conducted solely in rats remain inadequate when attempting to identify doses that comply with regulations for radiation exposure in humans.
The tissue dose from a radiotracer relates to both the radionuclide’s physical half-life (approximately 110 min for ^18^F) and biological half-life of the parent and radio-metabolites. Thus, organ radiation burden relates to the initial organ perfusion, retention until clearance and exposure from nearby organs. Highly perfused organs such as heart, lung, liver, kidney, and brain receive a larger fraction of the absorbed radiation and most radiotracer molecules undergo metabolism and are cleared by either the hepatobiliary (liver, gallbladder) or renal (kidneys, urinary bladder) systems. Similar to prior studies in the rat and non-human primate, we observe rapid renal uptake and clearance followed by cumulative urinary bladder radiation accumulation suggesting some urinary clearance [14]. Higher uptake in liver and gallbladder wall in non-human primates and humans suggests primary hepatobiliary clearance of ^18^F-VAT. This is not surprising since the hepatobiliary route is a common route of excretion for lipophilic compounds, supporting that administration of ^18^F-VAT to non-fasting participants may significantly reduce the critical dose burden to the gallbladder wall compared to fasting states, beyond urinary voiding between imaging segments that would reduce the absorbed dose to the urinary bladder.
Conclusion
Our data demonstrate that administration of approximately 249 MBq (6.7 mCi) ^18^F-VAT would produce a total human effective dose of < 4.4 mSv in the fasting state. Oral intake approximately 90 min following injection will limit radiation dose to the gallbladder wall, the critical organ where up to 465 MBq (12.6 mCi) may be injected to produce a similar total human effective dose of < 8.1 mSv in the non-fasting state. Our human dosimetry study indicates that ^18^F-VAT is a safe and promising VAChT radioligand, serving as an effective imaging tool for assessing cholinergic deficit and monitoring therapeutic effects in neurological and psychiatric disease. Administering oral caloric supplementation after ^18^F-VAT injection can reduce critical organ radiation exposure when higher radiotracer doses or multiple PET studies are desired in the same individual. Moreover, our method of reducing gallbladder dose through dietary means may have broad application to other brain PET radiopharmaceuticals, since CNS drugs are typically lipophilic in order to cross the blood–brain-barrier, and hence would also be expected to be excreted by the same hepatobiliary route followed by ^18^F-VAT.