Prevalence of Toxoplasma gondii Infection Among Blood Donors: A Systematic Review and Meta-Analysis
Maria Kantzanou, Evangelos Kostares, Georgia Kostare, Evangelia Papagiannopoulou, Michael Kostares, Athanasios Tsakris

TL;DR
This study reviews global data to estimate how common Toxoplasma gondii infection is among blood donors, using both serological and molecular methods.
Contribution
The study provides the first comprehensive meta-analysis of T. gondii prevalence in blood donors using both serological and molecular diagnostic methods.
Findings
The pooled serological prevalence of T. gondii infection among blood donors was 35.7%.
Molecular detection methods found a much lower prevalence of 1.9%.
High heterogeneity across studies suggests regional and methodological variability in T. gondii detection.
Abstract
Our study aims to thoroughly evaluate the prevalence of Toxoplasma gondii infection among blood donors, utilizing robust methodologies to inform public health policies and improve transfusion safety measures. An extensive literature search was executed across databases such as Medline, Scopus, and Cochrane Central, identifying observational studies reporting T. gondii seroreactivity and detection prevalence in blood donors across various regions. Heterogeneity was assessed visually via forest plots and statistically using Cochran’s Q test (with p-values) and the I² statistic with 95% CIs. The meta-analysis estimated pooled prevalence rates with a 95% CI and included rigorous quality assessments, outlier, and influential analyses to verify the findings’ validity. Thirty-eight studies, published between 1998 and 2024, were incorporated into our review, revealing a T. gondii reactivity…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
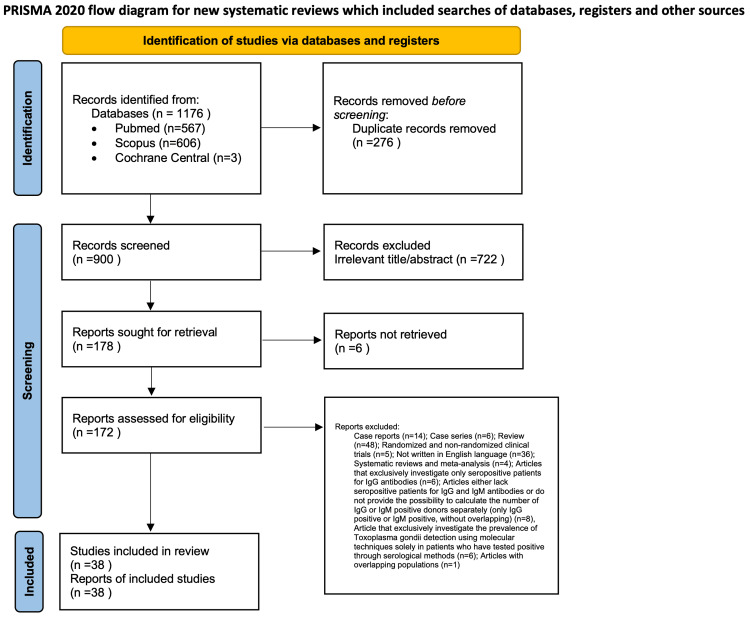 Figure 1
Figure 1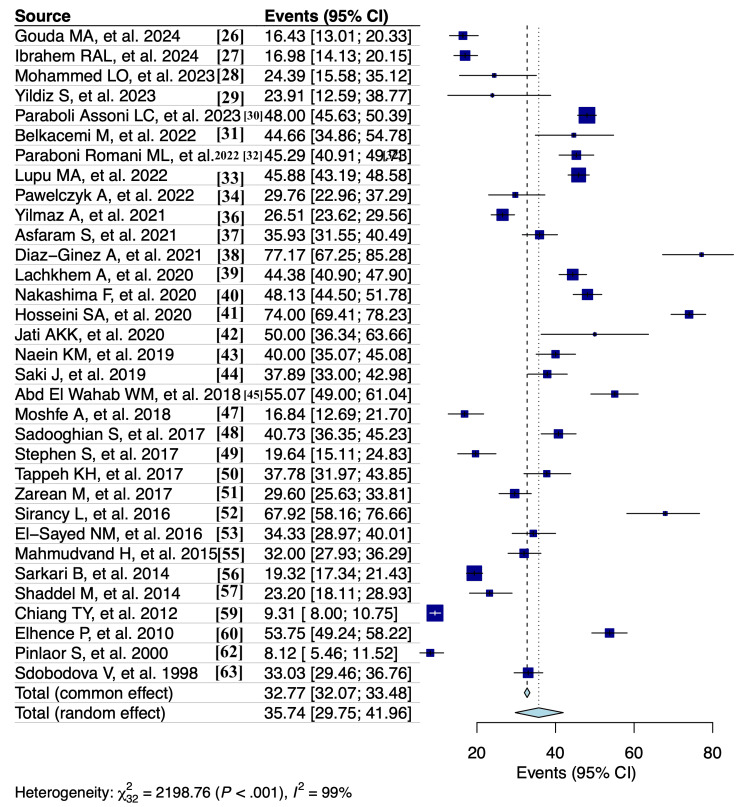 Figure 2
Figure 2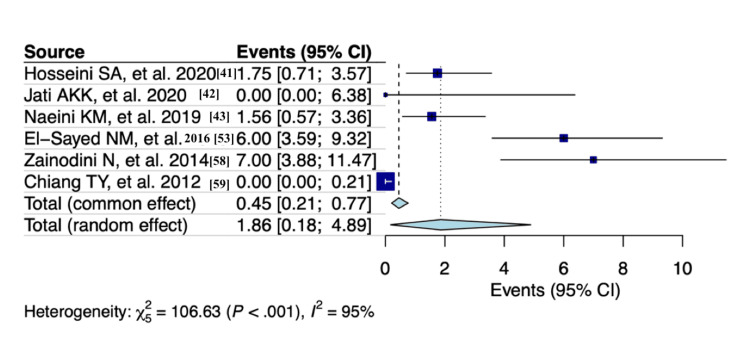 Figure 3
Figure 3| PECOS criteria | |
| Population (P) |
Blood donors. With the aim of collecting information from a wide range of participants in various places and times, the study focuses on determining the prevalence of |
| Exposure (E) |
The exposure under investigation is the presence of |
| Comparison (C) |
Since our goal was to measure the prevalence of |
| Outcomes (O) |
The prevalence rate of |
| Study types (S) | Our inclusion criteria encompassed solely observational studies, including cohort, case-control, and cross-sectional studies. |
| Criteria | Inclusion | Exclusion |
| Study types | Observational studies, including cohort, case-control, and cross-sectional studies | Case reports, case series with ≤20 participants, review articles, randomized clinical trials, nonrandomized clinical trials, animal studies, letters to the editor, books, expert opinions, conference abstracts, and studies without full-text availability |
| Language | English | Non-English articles |
| Publication date | No restrictions | None |
| Study design | Articles that examined specifically the prevalence rates of | Articles that exclusively investigate the prevalence of |
| Population overlap | Most recent or comprehensive publication used if populations overlap | Publications with overlapping populations |
| Authors | Year | Study design | Continent of origin | Country | Study period | Total patients | Proportion of males (%) | Mean age (years) | IgG positive | IgM positive | IgG and IgM positive | Seropositive patients | Molecularly diagnosed patients |
|
Gouda et al. [ | 2024 | Cross-sectional | Africa | Egypt | 2023 | 420 | 97.1 | 32.4 | 46 | 22 | 1 | 69 | NA |
|
Ibrahem et al. [ | 2024 | Cross-sectional | Africa | Egypt | 2023 | 630 | 96.7 | 31.9 | 68 | 37 | 2 | 107 | NA |
|
Mohammed et al. [ | 2023 | Cross-sectional | Asia | Iraq | 2019-2020 | 82 | 54.9 | 36.2 | 20 | 0 | 0 | 20 | NA |
|
Yildiz et al. [ | 2023 | Cross-sectional | Asia | Turkey | NA | 46 | 95.7 | NA | 10 | 0 | 1 | 11 | NA |
|
Assoni et al. [ | 2023 | Cross-sectional | South America | Brazil | NA | 1,729 | 65.1 | 34.5 | 797 | 3 | 30 | 830 | NA |
|
Belkacemi et al. [ | 2022 | Cross-sectional | Africa | Algeria | 2018 | 103 | 42.7 | 31 | 46 | 0 | 0 | 46 | NA |
|
Paraboni et al. [ | 2022 | Cross-sectional | South America | Brazil | 2020-2021 | 510 | 52.2 | 36.6 | 223 | 0 | 8 | 231 | NA |
|
Lupu et al. [ | 2022 | Cross-sectional | Europe | Romania | 2018 | 1347 | 56.1 | 33.6 | NA | NA | NA | 618 | NA |
|
Pawełczyk et al. [ | 2022 | Cross-sectional | Europe | Poland | 2013-2016 | 168 | 65.5 | NA | 49 | 0 | 1 | 50 | 29 |
|
Stopić et al. [ | 2022 | Cross-sectional | Europe | Serbia | 2017-2018 | 1,095 | 50.6 | NA | 224 | NA | 0 | NA | NA |
|
Yilmaz et al. [ | 2021 | Cross-sectional | Asia | Turkey | 2015 | 879 | 90 | 34 | 213 | 8 | 12 | 233 | NA |
|
Asfaram et al. [ | 2021 | Cross-sectional | Asia | Iran | 2017 | 462 | 97.2 | 39.3 | 150 | 7 | 9 | 166 | NA |
|
Díaz-Ginéz and Silva-Díaz [ | 2021 | Cross-sectional | South America | Peru | 2019 | 92 | 76.1 | NA | 71 | 0 | 0 | 71 | NA |
|
Lachkhem et al. [ | 2020 | Cross-sectional | Africa | Tunisia | 2017-2018 | 800 | 79.5 | 35 | 352 | 0 | 3 | 355 | NA |
|
Nakashima et al. [ | 2020 | Cross-sectional | South America | Brazil | NA | 750 | 67.5 | NA | 335 | 5 | 21 | 361 | NA |
|
Hosseini et al. [ | 2020 | Cross-sectional | Asia | Iran | 2014 | 400 | 95.3 | 35.5 | 287 | 2 | 7 | 296 | 7 |
|
Jati et al. [ | 2020 | Cross-sectional | Asia | Malaysia | 2017-2018 | 56 | 59 | NA | 24 | 0 | 2 | 26 | 0 |
|
Manouchehri Naeini et al. [ | 2019 | Cross-sectional | Asia | Iran | 2017 | 385 | 94.8 | 37.2 | 146 | 4 | 6 | 156 | 6 |
|
Saki et al. [ | 2019 | Cross-sectional | Asia | Iran | 2015 | 380 | NA | NA | 131 | 2 | 11 | 144 | NA |
|
Abd El Wahab et al. [ | 2018 | Cross-sectional | Africa | Egypt | 2016 | 276 | 78.3 | 29.7 | 135 | 2 | 15 | 152 | NA |
|
Kalantari et al. [ | 2018 | Cross-sectional | Asia | Iran | 2016-2017 | 500 | 97.6 | NA | 313 | NA | 3 | NA | NA |
|
Moshfe et al. [ | 2018 | Cross-sectional | Asia | Iran | 2015 | 285 | 96.8 | 37 | 46 | 0 | 2 | 48 | NA |
|
Sadooghian et al. [ | 2017 | Cross-sectional | Asia | Iran | 2014-2015 | 491 | 93.9 | 36.3 | 184 | 8 | 8 | 200 | NA |
|
Stephen et al. [ | 2017 | Cross-sectional | Asia | India | 2016 | 275 | 93.1 | 34.8 | 53 | 0 | 1 | 54 | NA |
|
Tappeh et al. [ | 2017 | Cross-sectional | Asia | Iran | 2013 | 270 | 96.7 | 34 | 102 | 0 | 0 | 102 | NA |
|
Zarean et al. [ | 2017 | Cross-sectional | Asia | Iran | 2013 | 500 | 89.6 | 29.7 | 125 | 16 | 7 | 148 | NA |
|
Siransy et al. [ | 2016 | Cross-sectional | Africa | Côte d'Ivoire | 2014 | 106 | 86.8 | NA | 60 | 4 | 8 | 72 | NA |
|
El-Sayed et al. [ | 2016 | Cross-sectional | Africa | Egypt | 2014-2015 | 300 | 100 | 22.8 | 93 | 2 | 8 | 103 | 18 |
|
Alvarado-Esquivel et al. [ | 2016 | Cross-sectional | North America | Mexico | 2015 | 408 | 81.9 | 31.8 | 43 | NA | 12 | NA | NA |
|
Mahmoudvand et al. [ | 2015 | Cross-sectional | Asia | Iran | 2014 | 500 | 91 | 28.9 | 144 | 11 | 5 | 160 | NA |
|
Sarkari et al. [ | 2014 | Cross-sectional | Asia | Iran | 2012-2013 | 1,480 | 94.3 | 39.1 | 182 | 81 | 23 | 286 | NA |
|
Shaddel et al. [ | 2014 | Cross-sectional | Asia | Iran | 2013 | 250 | NA | NA | 57 | NA | 1 | 58 | NA |
|
Zainodini et al. [ | 2014 | Cross-sectional | Asia | Iran | NA | 200 | NA | NA | NA | NA | NA | NA | 14 |
|
Chiang et al. [ | 2012 | Cross-sectional | Asia | Taiwan | 2010 | 1,783 | 63.2 | 38.1 | 161 | 0 | 5 | 166 | 0 |
|
Elhence et al. [ | 2010 | Cross-sectional | Asia | India | NA | 493 | 94.3 | NA | 240 | 9 | 16 | 265 | NA |
|
Alvarado-Esquivel et al. [ | 2007 | Cross-sectional | North America | Mexico | 2006 | 432 | 86.6 | 30.4 | 24 | NA | 8 | NA | NA |
|
Pinlaor et al. [ | 2000 | Cross-sectional | Asia | Thailand | 1997 | 345 | 67 | 31.4 | NA | NA | NA | 28 | NA |
|
Svobodová and Literák [ | 1998 | Cross-sectional | Europe | Czechia | 1992-1993 | 663 | 83.9 | NA | 203 | 6 | 10 | 219 | NA |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsToxoplasma gondii Research Studies · Travel-related health issues · Heme Oxygenase-1 and Carbon Monoxide
Introduction and background
*Toxoplasma gondii *is an intracellular parasitic protozoan and is classified under the phylum Apicomplexa and the subclass Coccidia. This microorganism exists in three main infectious stages: the oocyst, the tachyzoite, and the tissue cyst. Human infection with *T. gondii *can occur through various means, including foodborne transmission, animal-to-human transmission, congenital infection, organ transplantation, and blood transfusion [1-3].
One of the main sources of *T. gondii *transmission includes the consumption of undercooked or raw meat from infected animals, such as pork, lamb, and venison, which may harbor tissue cysts, and the ingestion of shellfish like oysters, clams, and mussels that can be contaminated with oocysts from polluted water. It is important to note that direct contact with animals does not typically result in transmission. Transmission can occur through the consumption of undercooked or raw meat containing tissue cysts or the ingestion of food or water contaminated with oocysts shed by infected cats. While direct contact with infected animals is not a significant route of transmission, handling contaminated surfaces or consuming unwashed produce can pose a risk. To minimize the risk of infection, proper food preparation, thorough washing of fruits and vegetables, good hygiene practices, and avoidance of potentially contaminated water sources are essential [1,4].
Transplant patients receiving organs from donors who are already positive for *T. gondii *antibodies, while the recipients are negative, are at risk of contracting the disease. The typical mode of toxoplasmosis development in bone marrow, hematopoietic stem cell, liver transplant patients, and those with AIDS is the reactivation of latent infections in the recipient. During gestation, if a pregnant woman acquires *T. gondii *for the first time, the parasite can reach the fetal circulation by infecting the placenta, posing a risk to the developing baby [1,4,5]. Furthermore, *T. gondii *can be transmitted through blood or white blood cells from both individuals with normal immune function and those with compromised immune systems. Infections in laboratory staff have occurred through accidental contact with contaminated needles or exposure to biological materials, such as tissues or fluids from infected animals, during laboratory procedures [1,5,6].
In the United States, approximately 11% of individuals are estimated to have contracted *T. gondii *[7]. Studies conducted in various regions worldwide have revealed infection rates exceeding 60% in certain populations for T. gondii. Recently, a comprehensive meta-analysis conducted by Wang et al. [8], which encompassed 74 studies (including 25,898 HIV-infected individuals), determined the prevalence of T. gondii reactivity to be 35.8% (95% CI: 30.8-40.7%). Infection rates tend to be highest in regions characterized by hot, humid climates and lower altitudes, as these environmental conditions favor the survival of oocysts [1]. While often asymptomatic in immunocompetent individuals, toxoplasmosis can cause severe disease in immunocompromised patients, including transplant recipients and individuals living with HIV [1,9].
Blood donors represent a subgroup for *T. gondii *surveillance because their donations are intended for transfusion into recipients who may be immunosuppressed, such as neonates, cancer patients, or organ transplant recipients. Even when asymptomatic, seropositive donors can harbor latent parasites, and rare but documented cases of transfusion-transmitted toxoplasmosis raise concerns about blood safety [9].
There is an abundance of variation in the prevalence of *T. gondii *reactivity and detection among blood donors, according to scientific literature. Our systematic review and meta-analysis seek to close this information gap by offering a thorough evaluation of the prevalence of Toxoplasma species in this particular group. Our research intends to provide important insights to the scientific community by revealing the full magnitude of this hidden reactivity within the blood donor population by combining data from other investigations.
Review
Materials and methods
Search Strategy
A comprehensive search of the literature was done in compliance with the Cochrane Handbook for Systematic Reviews of Interventions. This systematic review was organized and reported in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines [10]. The PRISMA checklist, available in Appendix A, was utilized to facilitate the systematic review process. A comprehensive literature search was conducted, covering works from their inception up to January 9, 2025, using the Medline/PMC Central (via PubMed), Scopus, and Cochrane Central databases, as shown in Figure 1. Two reviewers independently carried out the search, using a combination of keywords such as “toxoplasmosis”, “toxoplasma gondii”, “blood donors”, “blood transfusion”, “blood bank”, “blood donation”, “prevalence”, “incidence”, and “rate”. The detailed search strategy for each database is provided in Appendix B. To ensure no relevant studies were missed, we also thoroughly reviewed the reference lists of the identified studies. We used Zotero reference management software (version 6.0.18) to organize and manage the collected research meticulously [11]. Duplicate references were carefully removed to ensure the dataset’s integrity. Two independent reviewers then scrutinized the remaining articles individually. The study selection process was conducted in two phases: first, titles and abstracts were screened to exclude studies that did not meet the predefined inclusion criteria, followed by a thorough evaluation of the full texts of the remaining papers. Any disagreements were resolved by consensus among team members, ensuring consistency in decision-making. This systematic approach ensured the compilation of a comprehensive and reliable set of studies for analysis.
Flowchart depicting the systematic search results from the relevant studies’ identification and selectionPRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses
Criteria for Study Selection and Data Extraction
Following an exhaustive and meticulous search across multiple databases, we meticulously defined our eligibility criteria using the PECOS framework. This rigorous process was undertaken to ensure maximum clarity, precision, and thoroughness in our systematic review and meta-analysis, which centers on the prevalence of T. gondii reactivity and detection among blood donors. By adhering to this structured approach, we aimed to achieve a comprehensive and reliable synthesis of the available data. In Table 1, the PECOS framework is presented.
Table 2 provides a clear framework for the selection of studies by outlining the specific inclusion and exclusion criteria for the systematic review and meta-analysis.
A concise summary of the inclusion and exclusion criteria is presented below. Eligible studies were observational in design (cross-sectional, cohort, or case-control) and specifically investigated the prevalence of *T. gondii *reactivity or detection among blood donors using serological (e.g., IgG and IgM) and/or molecular (e.g., PCR) diagnostic methods applied to the full study population. Studies were excluded if they lacked primary data (e.g., reviews and case reports), focused on nonrepresentative subgroups (e.g., only seropositive individuals), had overlapping populations without new data, or did not provide sufficient detail to extract or calculate relevant prevalence measures.
Data Extraction
From each included study, we collected the following details: the authors’ names, year of publication, type of study design, continent and country of origin, duration of the study, total number of blood units, percentage of male participants, average age, number of patients with *T. gondii *reactivity, and the diagnostic procedures used.
Quality Assessment
Using the Quality Assessment Tools from the National Heart, Lung, and Blood Institute (NHLBI), two researchers independently evaluated the quality of their research. This was accomplished by using the NHLBI Observational Cohort and Cross-Sectional Studies Quality Assessment Tool, specifically. Every research study was carefully examined to find any possible methodological or survey implementation problems that would jeopardize the study’s internal validity. In order to complete the assessment, participants had to answer 14 questions with the following options: “yes,” “no,” “cannot determine” (for example, because of ambiguous or inconsistent data), “not reported” (for example, when data was missing), or “not applicable” (for example, when a question was not pertinent to the study in question). According to reference [17], these evaluations produced three different study quality levels: “low,” “moderate,” and “high” risk of bias (Appendix C).
Statistical Analysis
We conducted a thorough statistical analysis for the meta-analysis using the metafor package [18,19]. The overall prevalence and its 95% CIs were estimated using the DerSimonian and Laird random effects model. To address variance instability, the Freeman-Tukey double arcsine transformation was applied for outcomes such as IgM antibodies, combined IgG/IgM antibodies, and molecular diagnostic results [20]. Conversely, the logit transformation was used to evaluate the serological diagnostic techniques and the prevalence of IgG antibodies [21].
Heterogeneity: Heterogeneity among the studies was evaluated both visually, through forest plot inspection, and statistically, using Cochran’s Q statistic along with its p-value. Additionally, the Higgins I² statistic, accompanied by its 95% CI, was employed to quantify the extent of true heterogeneity in effect sizes. The I² values were interpreted as follows: 0-40% indicated not important heterogeneity, 30-60% indicated moderate heterogeneity, 50-90% indicated substantial heterogeneity, and 75-100% indicated considerable heterogeneity.
Sensitivity analysis: To identify and assess potentially influential outliers, we screened for externally studentized residuals with absolute z-values greater than two and performed leave-one-out diagnostics [22]. Unless otherwise noted, statistical significance was set at p = 0.05 (two-tailed).
Publication bias: We assessed publication bias using Egger’s test [23], Begg’s test [24], and funnel plots, which are standard methods for comparing data. These tests operate on the assumption that studies with positive results are more likely to be published than those with negative results. However, in a meta-analysis of proportions, there's no clear agreement on what defines a positive result [25]. Therefore, we evaluated publication bias in this meta-analysis qualitatively.
All analyses were conducted using the RStudio program (version 2022.12.0+353) [18].
Results
Results and Characteristics of the Included Studies
From 1,176 articles initially identified, 38 studies were finally included in this analysis. All articles were published from 1998 to 2024 (conducted from 1992 to 2023). All of them were of cross-sectional design. Most of the studies were carried out in Asia (Iran, Turkey, Malaysia, India, Taiwan, Thailand, and Iraq), followed by Africa (Tunisia, Egypt, Algeria, and Côte d'Ivoire), Europe (Serbia, Czechia, Poland, and Romania), North America (Mexico), and South America (Brazil and Peru). Thirty-seven studies encompassing 19,691 participants were included to investigate the prevalence of *T. gondii *reactivity through serological diagnostic procedures, such as ELISA, direct agglutination assay, and electrochemiluminescence immunoassay. Collective analysis revealed that males made up an average of 80.9% of participants, with a mean age ranging from 22.8 to 39.3 years and a median age of 34 years. Seven studies, involving 3,292 participants, explored the prevalence of *T. gondii *detection using molecular diagnostic techniques such as real-time and conventional PCR. In these studies, males accounted for an average of 74.5% of participants, with a mean age range of 22.8 to 38.1 years and a median age of 34 years. All studies were assessed as being of moderate quality. The descriptive characteristics of them are reported in Table 3.
Prevalence of T. gondii Reactivity and Detection Among Blood Donors
A random effects model analysis revealed a prevalence of *T. gondii *reactivity among blood donors, determined using serological diagnostic methods, at 35.7% (95% CI: 29.8-42%), accompanied by substantial heterogeneity between studies (I² = 99%, p < 0.001) (Figure 2). The influence diagnostics and the forest plot illustrating the results of the leave-one-out analysis are presented in Appendix D and Appendix E. According to them, no study was identified as influential.
Forest plot showing Toxoplasma gondii seroprevalence among blood donors using a random effects model (serological diagnostic methods)
When specifically looking at the prevalence of different types of antibodies, the estimates were as follows: 32% (95% CI: 26-38.2%) for IgG antibodies (I² = 99%, p < 0.001) (Appendix F), 0.8% (95% CI: 0.3-1.3%) for IgM antibodies (I² = 92%, p < 0.001) (Appendix G), and 1.2% (95% CI: 0.8-1.6%) for both IgG and IgM antibodies combined (I² = 81%, p < 0.001) (Appendix H). The influence diagnostics and the forest plot illustrating the results of the leave-one-out analysis are presented in Appendix I, Appendix J, Appendix K, Appendix L, Appendix M, and Appendix N. According to them, no study was identified as influential.
A random effects model analysis revealed a prevalence of *T. gondii *detection among blood donors, determined using molecular diagnostic methods, at 3.2% (95% CI: 0.4-8%), accompanied by substantial heterogeneity between studies (I² = 95%, p < 0.001). The influence diagnostics and the forest plot illustrating the results of the leave-one-out analysis are presented in Appendix O and Appendix P. According to them, the study conducted by Pawelczyk et al. (2022) [34] was identified as influential in this analysis. After the exclusion of the aforementioned study, the prevalence is estimated as 1.9% (95% CI: 0.2-4.9%) with substantial heterogeneity (I² = 95%, p < 0.001) (Figure 3).
Forest plot evaluating the calculated prevalence of Toxoplasma gondii detection among blood donors using random effects model (molecular diagnostic procedures)
Discussion
Our study highlights the prevalence of *T. gondii *reactivity and detection among blood donors, using a combination of serological and molecular diagnostic methods. While serological methods primarily measured the presence of *T. gondii *antibodies, molecular techniques provided an additional layer of detection by identifying the parasite’s DNA, thereby offering a comprehensive overview of *T. gondii *prevalence in this population.
Nonetheless, it is crucial to recognize that there is substantial heterogeneity among the research. There are multiple possible explanations for the substantial heterogeneity that was noted among the included studies. First, it is important to note that the current studies are observational and have been carried out under various circumstances, at various times, and in various locations. Consequently, variations in demographics and geographic areas under investigation likely contribute to the disparities in *T. gondii *reactivity and detection prevalence. Differences in prevalence and transmission severity are expected, as the disease is endemic in many regions.
Heterogeneity may also stem from differences in the age, sex, and health condition of blood donors, as well as variations in sample sizes, inclusion criteria, and diagnostic techniques. Disparities in the sensitivity, specificity, and accuracy of diagnostic methods (both molecular and serological) further contribute to these variations.
Our intention in presenting a pooled estimate is not to suggest uniformity across regions but to offer a global perspective that can inform broader public health strategies, especially in areas where local data are limited or unavailable. While local data are essential for tailoring interventions to specific regions, pooled estimates reveal overarching trends and provide a valuable benchmark for understanding the global burden of the disease.
It is crucial to consider these variables when analyzing prevalence estimates and addressing observed heterogeneity. Given the nature of this study, some variation in prevalence and incidence is anticipated. Therefore, in the context of proportional meta-analysis, a high I² does not necessarily imply inconsistency [25].
Foroutan-Rad et al. [64] conducted a meta-analysis that calculated the weighted overall prevalence of *T. gondii *antibodies to be 33% (95% CI: 28-39%) using serological methods. The seroprevalence of immunoglobulin IgM and both IgG and IgM antibodies was found to be 1.8% (95% CI: 1.1-2.4%) and 1.1% (95% CI: 0.3-1.8%), respectively. In another study, Wang et al. [65] calculated the prevalence of *T. gondii *infection in Chinese blood donors, reporting an overall IgG seroprevalence of 6.3% (95% CI: 4.6-8.1%). Lastly, the study conducted by Foroutan et al. [66] in 2024 found a moderate exposure rate to *T. gondii *among Iranian blood donors, with 32.9% seropositive for IgG, 1.4% for IgM, and 1.7% for both antibodies. Similar to the previous study, considerable heterogeneity was observed among the included studies.
Our findings align closely with those of previous meta-analyses, reaffirming the prevalence estimates of *T. gondii *reactivity among blood donors. While there is general agreement, minor variations were observed, which could be attributed to differences in the total number of studies included, study populations and geographical locations, database sources, different inclusion and exclusion criteria, quality assessments, analyses of outliers and influential analyses, inherent heterogeneity among the studies, and possible temporal changes in *T. gondii *reactivity prevalence. Besides this, one also has to consider the possible biases in sample selection for each study and different sensitivities and specificities of the diagnostic methods available that may further explain the prevalence differences observed between estimates.
In most cases, acute toxoplasmosis is self-limiting, and the majority of healthy adults without immunocompromisation or pregnancy do not necessitate treatment. Nevertheless, individuals with severe or prolonged symptoms and those showing signs of pneumonitis, myocarditis, meningoencephalitis, posterior uveitis, or polymyositis are advised to undergo treatment. The antimicrobial regimens employed for treating immunocompetent individuals are the same as those used for immunocompromised patients, which include either pyrimethamine combined with sulfadiazine and leucovorin or pyrimethamine combined with clindamycin and leucovorin [67,68].
Strengths and Limitations
The comprehensive methodology used for the literature search, study selection, inclusion/exclusion criteria, eligibility screening, quality assessment, and pooled analysis of prevalence data from 38 studies is a major strength of this investigation. However, caution is needed when interpreting the results due to significant, unidentified heterogeneity. The variability in outcomes across the included studies was expected, given the nature of this research [69,70]. Several factors likely contributed to this heterogeneity, including differences in diagnostic methods, sample sizes, inclusion criteria, and variations in age, sex, geographical location, contact with animals, soil exposure, dietary habits (such as consumption of unwashed vegetables or undercooked meat), income levels, and health status of blood donors, all of which may introduce bias in estimating the prevalence of T. gondii.
Additionally, a positive diagnostic result does not always indicate active infection, and variations in the sensitivity, specificity, and accuracy of diagnostic techniques (serological and molecular) can lead to discrepancies in detecting the parasite among blood donors. In this context, IgG and IgM results have distinct clinical and epidemiological implications. IgG antibodies reflect prior exposure and generally indicate long-term immunity; thus, a positive IgG result in a blood donor suggests past infection without necessarily indicating a current risk of transmission. Conversely, IgM antibodies are typically associated with recent or acute infection. However, the persistence of IgM for months or even years after infection complicates interpretation, as it may not reflect ongoing parasitemia. From a clinical perspective, IgM positivity may raise concern for potential transfusion-transmitted toxoplasmosis, especially if parasitemia is confirmed by molecular testing. From an epidemiological perspective, IgG prevalence indicates cumulative exposure within a population, while IgM prevalence can provide insight into recent transmission patterns. Therefore, separate reporting and interpretation of IgG and IgM are essential for accurate risk assessment and public health decision-making.
The regional heterogeneity in *T. gondii *reactivity and detection prevalence, testing practices, and study designs further limit the generalizability of the pooled international estimate to specific regions. While a global analysis offers a broad perspective, it may not fully reflect local epidemiological differences. Moreover, the persistence of IgM antibodies, which are typically indicative of acute infection but can remain in the bloodstream for extended periods, and the low sensitivity of PCR in blood complicate the accurate detection of T. gondii. These diagnostic limitations can affect the interpretation of prevalence rates in the included studies. Due to limited data (fewer than 10 studies reporting on variables such as male proportion, mean age, and comorbidities), these covariates were excluded from the analysis.
Additionally, passive antibodies from seropositive donors may transiently affect the immune status of recipients, potentially leading to misinterpretation of the recipient’s immunity. This meta-analysis was not registered in PROSPERO. Only observational studies published in English were included, resulting in further reporting bias. Given these considerations, it is important to acknowledge that, like any meta-analysis, our study is subject to potential biases, including selection bias, language bias, search bias, heterogeneity bias, confounding bias, and data extraction bias, all of which may influence the validity and generalizability of our findings.
Conclusions
Our systematic review and meta-analysis on the prevalence of *T. gondii *reactivity and detection among blood donors highlight a significant public health issue. Enhanced screening protocols are crucial to protect vulnerable transfusion recipients. Rather than focusing solely on prevention, targeted screening can help detect active or recent infections and reduce transmission risk. Additionally, raising awareness about toxoplasmosis and promoting hygiene practices can contribute to risk reduction. These findings highlight the need for risk mitigation strategies and further localized research to improve transfusion safety.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Toxoplasmosis Stat Pearls [Internet] Madireddy S Mangat R Treasure Island (FL)Stat Pearls Publishing 2025 https://pubmed.ncbi.nlm.nih.gov/33085433/33085433 · pubmed ↗
- 2Toxoplasmosis Lancet Montoya JG Liesenfeld O 1965197636320041519425810.1016/S 0140-6736(04)16412-X · doi ↗ · pubmed ↗
- 3About toxoplasmosishttps://www.cdc.gov/toxoplasmosis/about/?CDC_A Aref_Val=https://www.cdc.gov/parasites/toxoplasmosis/gen_info/faqs.html
- 4Management of Toxoplasma gondii infection during pregnancy Clin Infect Dis Montoya JG Remington JS 5545664720081862463010.1086/590149 · doi ↗ · pubmed ↗
- 5Toxoplasma gondii: transmission, diagnosis and prevention Clin Microbiol Infect Hill D Dubey JP 634640820021239028110.1046/j.1469-0691.2002.00485.x · doi ↗ · pubmed ↗
- 6Toxoplasmosis Handb Clin Neurol Halonen SK Weiss LM 12514511420132382990410.1016/B 978-0-444-53490-3.00008-XPMC 4157368 · doi ↗ · pubmed ↗
- 7People at increased risk for toxoplasmosishttps://www.cdc.gov/toxoplasmosis/risk-factors/?CDC_A Aref_Val=https://www.cdc.gov/parasites/toxoplasmosis/epi.html
- 8Prevalence and burden of Toxoplasma gondii infection in HIV-infected people: a systematic review and meta-analysis Lancet HIV Wang ZD Wang SC Liu HH 1771884201710.1016/S 2352-3018(17)30005-X 28159548 · doi ↗ · pubmed ↗