Polytobacco usage and mental health among Malaysian secondary school-going adolescents: Findings from the national school-based study
Kuang Hock Lim, Yoon Ling Cheong, Jia Hui Lim, Chee Cheong Kee, Sumarni Mohd Ghazali, Yong Kang Cheah, Pei Pei Heng, Ali Aman Marine, Mohd Hazilas Mat Hashim, Wei Wen Goh, Hui Li Lim

TL;DR
This study examines how using multiple tobacco products affects mental health in Malaysian teenagers, finding that polytobacco users experience higher stress and depression.
Contribution
The study identifies a significant association between polytobacco use and mental health issues in adolescents using national survey data.
Findings
Polytobacco users had 1.64 times higher odds of stress symptoms compared to non-users.
Polytobacco users had 1.75 times higher odds of depression symptoms compared to non-users.
7.3% of adolescents were polytobacco users, showing elevated stress and depression levels.
Abstract
The emergence of novel tobacco products has led to an increase in the consumption of diverse tobacco items among adolescents. The smoking habits of adolescents adversely affect their physical and emotional health. This study aimed to ascertain the prevalence of polytobacco use among Malaysian teenagers and to identify the mental health issues associated with dual or polytobacco use. This is a secondary dataset analysis of cross-sectional data from 27479 secondary school adolescents who participated in the 2017 Malaysian Adolescent School Health survey. The primary outcome of our study pertained to self-reported mental health characteristics (stress and depressive symptoms). The research used multivariable logistic regression analysis to assess the associations between the use of tobacco products and mental wellness. Of the respondents, 79.9% were non-tobacco users, 9.2% were single…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
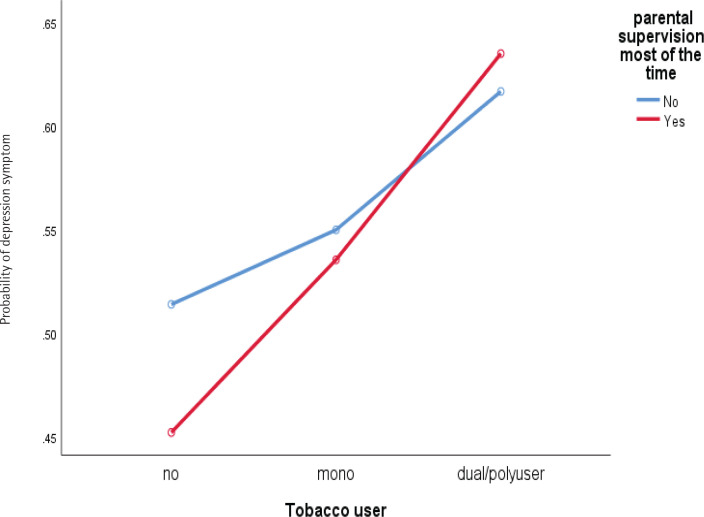 Figure 1
Figure 1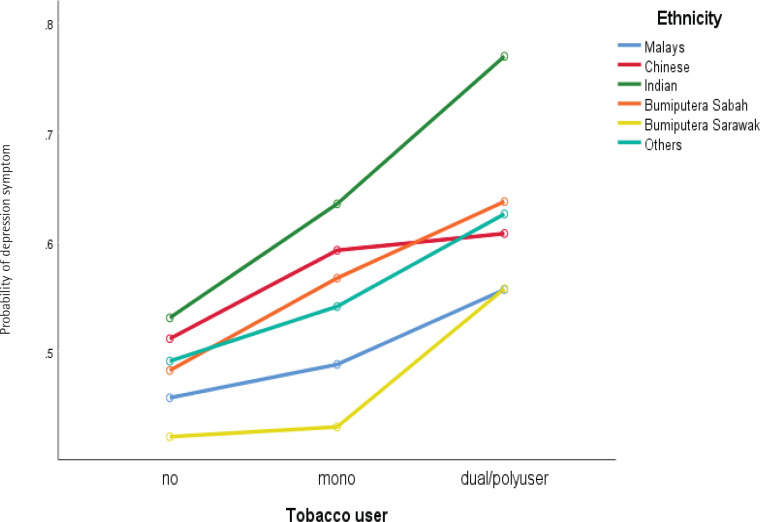 Figure 2
Figure 2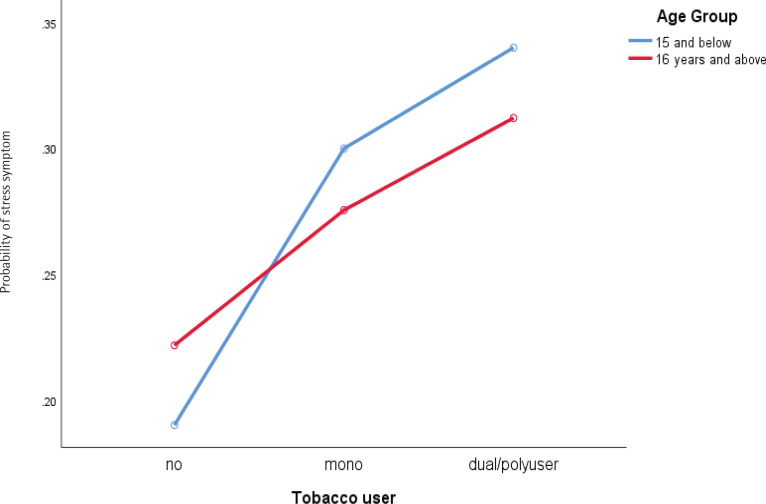 Figure 3
Figure 3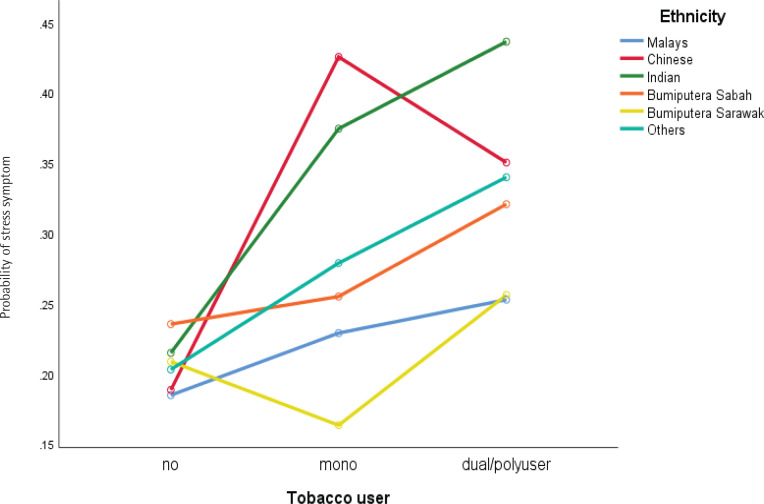 Figure 4
Figure 4|
|
|
|
|
|
|---|---|---|---|---|
|
| ||||
| Male | 1064953 | 13135 | 49.6 | 46.5–52.7 |
| Female | 1081492 | 14362 | 50.4 | 47.3–53.5 |
|
| ||||
| Urban | 1210741 | 15899 | 56.4 | 52.8–60.0 |
| Rural | 935705 | 11598 | 46.6 | 40.0–47.2 |
|
| ||||
| Malay | 1354538 | 18713 | 63.1 | 57.7–68.2 |
| Chinese | 358504 | 4100 | 16.7 | 13.4–20.6 |
| Indian | 149227 | 1428 | 7.0 | 5.2–9.3 |
| Bumiputra Sabah | 149354 | 1781 | 7.0 | 4.3–11.1 |
| Bumiputra Sarawak | 96823 | 924 | 4.5 | 2.6–7.6 |
| Other | 37997 | 554 | 1.8 | 1.3–2.5 |
| 13–15 | 1302499 | 16952 | 60.7 | 56.8–64.5 |
| 16–17 | 843946 | 10545 | 39.3 | 35.6–43.2 |
|
| ||||
| Married | 1834475 | 23544 | 87.4 | 86.7–88.0 |
| Divorce/separated | 264521 | 3387 | 12.6 | 12.0–13.3 |
|
| ||||
| Yes | 542467 | 6735 | 25.3 | 24.1–26.6 |
| No | 1600544 | 20722 | 74.7 | 73.4–75.9 |
|
| ||||
| Yes | 253449 | 3034 | 11.8 | 10.8–12.9 |
| No | 1888965 | 24416 | 88.2 | 87.1–89.2 |
|
| ||||
| Yes | 533138 | 6584 | 24.9 | 23.6–26.2 |
| No | 1609941 | 20877 | 75.1 | 72.8–76.4 |
|
| ||||
| Yes | 346882 | 4436 | 16.2 | 15.2–17.2 |
| No | 1795518 | 23022 | 83.8 | 82.8–84.8 |
|
| ||||
| Yes | 924222 | 11681 | 43.2 | 41.8–44.7 |
| No | 1214101 | 15727 | 56.8 | 55.3–58.2 |
|
| ||||
| Yes | 2058223 | 25424 | 96.4 | 96.8–95.9 |
| No | 77103 | 942 | 3.6 | 3.2–4.1 |
|
| ||||
| No | 1674730 | 21699 | 78.9 | 77.7–80.0 |
| Mono | 194349 | 2458 | 9.2 | 8.6–9.7 |
| Dual/poly | 254742 | 3066 | 12.0 | 11.1–12.9 |
|
| ||||
| Yes | 900560 | 11385 | 42.0 | 40.5–43.6 |
| No | 1242418 | 16070 | 58.0 | 56.4–59.5 |
|
| ||||
| Yes | 282898 | 3713 | 13.2 | 12.5–13.9 |
| No | 1860778 | 23473 | 86.8 | 86.1–87.5 |
|
|
| ||||||||
|---|---|---|---|---|---|---|---|---|---|
|
|
| ||||||||
|
|
|
|
|
|
|
|
|
| |
|
| |||||||||
| Male | 194089 | 2331 | 18.8 | 17.7–19.9 | 838700 | 10443 | 81.2 | 80.1–82.3 | 0.003 |
| Female | 219976 | 2921 | 20.9 | 19.8–22.0 | 833211 | 11103 | 79.1 | 78.2–80.2 | |
|
| |||||||||
| Urban | 247451 | 3218 | 20.9 | 19.7–22.2 | 937639 | 12366 | 79.1 | 77.8–80.3 | 0.006 |
| Rural | 166614 | 2034 | 18.5 | 17.4–19.6 | 734272 | 9180 | 81.5 | 80.4–82.6 | |
|
| |||||||||
| Malay | 242325 | 3402 | 18.4 | 17.4–19.4 | 1074653 | 14856 | 81.6 | 80.6–82.6 | <0.001 |
| Chinese | 71821 | 795 | 20.4 | 18.5–22.5 | 279875 | 3226 | 79.6 | 77.5–81.5 | |
| Indian | 37635 | 341 | 26.1 | 22.6–29.9 | 106747 | 1045 | 73.9 | 70.1–77.4 | |
| Bumiputra Sabah | 34841 | 414 | 24.4 | 21.3–27.5 | 108023 | 1297 | 75.6 | 72.5–78.5 | |
| Bumiputra Sarawak | 19211 | 183 | 20.4 | 17.1–24.1 | 75041 | 716 | 79.6 | 75.9–82.9 | |
| Other | 8230 | 117 | 23.0 | 18.6–28.1 | 27570 | 406 | 77.0 | 71.9–81.4 | |
| 13–15 | 240436 | 3121 | 19.2 | 17.9–20.1 | 1026004 | 13407 | 81.0 | 79.9–82.1 | 0.016 |
| 16–17 | 173629 | 2131 | 21.2 | 19.9–22.6 | 645907 | 8139 | 78.8 | 77.4–80.1 | |
|
| |||||||||
| Married | 347353 | 4392 | 19.5 | 18.6–20.4 | 1436656 | 18575 | 80.5 | 79.6–81.4 | 0.006 |
| Divorce/separated | 56207 | 725 | 22.0 | 20.2–23.8 | 199745 | 2557 | 78.0 | 76.2–79.8 | |
|
| |||||||||
| Yes | 147306 | 1816 | 28.0 | 25.4–29.7 | 378823 | 4734 | 72.0 | 70.3–73.5 | <0.001 |
| No | 266194 | 3428 | 17.1 | 16.2–18.0 | 1290732 | 16784 | 82.9 | 82.0–83.8 | |
|
| |||||||||
| Yes | 82086 | 1007 | 33.6 | 31.3–36.1 | 162072 | 1931 | 66.4 | 63.9–68.7 | <0.001 |
| No | 330556 | 4231 | 18.0 | 17.1–18.9 | 1507644 | 19587 | 82.0 | 81.1–82.4 | |
|
| |||||||||
| Yes | 143550 | 1764 | 27.8 | 26.2–29.4 | 372590 | 4630 | 72.8 | 70.6–73.8 | <0.001 |
| No | 269685 | 3480 | 17.2 | 16.4–18.1 | 1297299 | 16892 | 82.8 | 81.9–83.6 | |
|
| |||||||||
| Yes | 113802 | 1459 | 34.1 | 32.0–36.2 | 220279 | 2843 | 65.9 | 63.8–68.0 | <0.001 |
| No | 299597 | 3786 | 17.1 | 16.3–18.0 | 1448935 | 18676 | 82.9 | 82.0–83.7 | |
|
| |||||||||
| Yes | 241255 | 3112 | 26.9 | 25.6–28.2 | 657208 | 8270 | 73.1 | 71.8–74.4 | <0.001 |
| No | 171063 | 2121 | 14.5 | 13.7–15.4 | 1008503 | 13211 | 85.5 | 84.6–86.3 | |
|
| |||||||||
| Yes | 391134 | 4941 | 19.5 | 18.7–20.4 | 1610249 | 20829 | 80.5 | 79.6–81.3 | |
| No | 20916 | 283 | 28.2 | 24.5–32.1 | 53378 | 626 | 71.8 | 67.9–75.5 | |
|
| |||||||||
| Yes | 54228 | 637 | 19.8 | 17.9–21.9 | 219178 | 2968 | 80.2 | 78.1–82.1 | 0.993 |
| No | 359292 | 4608 | 19.8 | 19.0–20.7 | 1451294 | 18555 | 80.2 | 79.3–81.0 | |
|
| |||||||||
| No | 301089 | 3890 | 18.4 | 17.5–19.4 | 1333040 | 17328 | 81.6 | 80.6–82.5 | <0.001 |
| Mono | 40167 | 519 | 21.5 | 19.3–23.9 | 146602 | 1858 | 78.5 | 76.1–80.7 | |
| Dual/poly | 68521 | 788 | 28.1 | 25.8–30.5 | 175537 | 2156 | 70.9 | 69.5–74.2 | |
|
| |||||||||
| Yes | 197752 | 2447 | 22.6 | 21.4–23.9 | 675927 | 8632 | 77.4 | 76.1–78.6 | <0.001 |
| No | 171063 | 2798 | 17.8 | 16.9–18.8 | 993888 | 12886 | 82.2 | 81.2–83.1 | |
|
|
| ||||||||
|---|---|---|---|---|---|---|---|---|---|
|
|
| ||||||||
|
|
|
|
|
|
|
|
|
| |
|
| |||||||||
| Male | 333015 | 4010 | 32.2 | 30.6–33.8 | 701615 | 8783 | 67.8 | 66.2–69.4 | 0.233 |
| Female | 352643 | 4615 | 33.4 | 32.0–34.8 | 703833 | 9437 | 66.6 | 65.2–68.0 | |
|
| |||||||||
| Malay | 395731 | 5547 | 30.0 | 28.7–31.3 | 923856 | 12731 | 70.0 | 68.7–71.3 | <0.001 |
| Chinese | 124375 | 1378 | 35.3 | 32.8–38.6 | 227530 | 2647 | 64.7 | 62.0–67.2 | |
| Indian | 67888 | 597 | 47.2 | 42.2–52.2 | 75944 | 787 | 52.8 | 47.8–57.8 | |
| Bumiputra Sabah | 56203 | 637 | 38.8 | 35.0–42.8 | 88548 | 1089 | 61.2 | 57.2–65.0 | |
| Bumiputra Sarawak | 28286 | 269 | 29.9 | 26.3–33.8 | 66317 | 633 | 70.1 | 66.2–73.7 | |
| Other | 13180 | 197 | 36.2 | 29.7–43.2 | 23251 | 333 | 63.8 | 56.8–70.3 | |
| 13–15 | 412135 | 5317 | 32.5 | 31.1–34.0 | 855645 | 11237 | 67.5 | 66.0–68.9 | 0.557 |
| 16–17 | 273524 | 3308 | 33.2 | 31.4–35.1 | 549803 | 6983 | 66.8 | 64.9–68.6 | |
|
| |||||||||
| Married | 564903 | 7142 | 31.6 | 30.5–32.7 | 1223229 | 15871 | 68.4 | 67.3–69.5 | <0.001 |
| Divorce/separated | 99149 | 1222 | 38.6 | 36.2–41.1 | 157445 | 2057 | 61.4 | 58.9–63.8 | |
|
| |||||||||
| Yes | 234551 | 2856 | 44.5 | 42.5–46.6 | 292105 | 3700 | 55.5 | 53.4–57.5 | <0.001 |
| No | 449947 | 5752 | 28.8 | 27.7–29.9 | 1111662 | 14502 | 71.2 | 70.1–72.3 | |
|
| |||||||||
| Yes | 234055 | 2821 | 45.4 | 43.3–47.5 | 281967 | 3579 | 54.6 | 52.5–56.7 | <0.001 |
| No | 450384 | 5789 | 28.8 | 27.6–29.7 | 1121790 | 14624 | 71.4 | 70.3–72.4 | |
|
| |||||||||
| Yes | 133484 | 1594 | 54.3 | 51.6–57.0 | 112153 | 1347 | 45.7 | 43.0–48.0 | <0.001 |
| No | 550250 | 7009 | 29.9 | 28.8–31.0 | 1291568 | 16852 | 70.1 | 69.0–71.2 | |
|
| |||||||||
| Yes | 176318 | 2213 | 52.7 | 50.2–55.2 | 158514 | 2088 | 47.3 | 44.8–49.8 | <0.001 |
| No | 506808 | 6391 | 28.9 | 27.9–30.0 | 1245696 | 16117 | 71.1 | 70.0–72.1 | |
|
| |||||||||
| Yes | 380703 | 4788 | 42.3 | 40.7–43.9 | 519523 | 6612 | 57.7 | 56.1–59.3 | <0.001 |
| No | 301959 | 3802 | 25.5 | 24.3–26.8 | 881282 | 11561 | 74.5 | 73.2–75.7 | |
|
| |||||||||
| Yes | 38399 | 479 | 51.3 | 46.6–56.5 | 36120 | 433 | 48.5 | 43.5–53.4 | <0.001 |
| No | 643301 | 8095 | 32.1 | 31.0–33.2 | 1363026 | 17718 | 67.9 | 66.8–69.0 | |
|
| |||||||||
| Yes | 258986 | 3316 | 28.0 | 26.7–29.3 | 666098 | 8946 | 72.0 | 70.7–73.3 | 0.015 |
| No | 723733 | 5299 | 36.6 | 35.1–38.1 | 737632 | 9252 | 63.4 | 61.9–64.9 | |
|
| |||||||||
| No | 494108 | 6349 | 30.2 | 29.1–31.3 | 1141676 | 14884 | 69.8 | 68.7–70.9 | <0.001 |
| Mono | 67105 | 854 | 35.6 | 32.8–38.4 | 121469 | 1539 | 64.4 | 61.6–67.2 | |
| Dual/poly | 115014 | 1311 | 46.8 | 43.4–50.2 | 130709 | 1651 | 53.2 | 49.8–56.6 | |
|
| |||||||||
| Yes | 315753 | 3889 | 36.0 | 34.4–37.6 | 561332 | 7218 | 64.0 | 62.4–65.6 | <0.001 |
| No | 368566 | 4721 | 30.4 | 29.2–31.7 | 842456 | 10981 | 69.6 | 68.3–70.8 | |
|
|
|
| ||
|---|---|---|---|---|
|
|
|
|
| |
|
| ||||
| Male ® | 1 | 1 | ||
| Female | 1.33 | 1.21–1.45 | 1.24 | 1.13–1.35 |
|
| ||||
| Urban | 1.19 | 1.07–1.33 | 1.06 | 0.96–1.17 |
| Rural ® | 1 | 1 | ||
|
| ||||
| Malay ® | 1 | 1 | ||
| Chinese | 1.23 | 1.05–1.44 | 1.45 | 1.27–1.66 |
| Indian | 1.25 | 1.02–1.54 | 1.81 | 1.52–2.17 |
| Bumiputra Sabah | 1.32 | 1.13–1.55 | 1.33 | 1.13–1.57 |
| Bumiputra Sarawak | 1.06 | 0.85–1.35 | 0.85 | 0.70–1.04 |
| Other | 1.20 | 0.90–1.59 | 1.23 | 0.91–1.66 |
| 13–15 ® | 1 | |||
| 16–17 | 1.27 | 1.14–1.41 | ||
|
| ||||
| Married ® | 1 | 1 | ||
| Divorce/separated | 1.03 | 0.92–1.15 | 1.24 | 1.11–1.37 |
|
| ||||
| Yes | 1.30 | 1.15–1.44 | 1.22 | 1.10–1.36 |
| No ® | 1 | 1 | ||
|
| ||||
| Yes | 1.22 | 1.10–1.35 | 1.25 | 1.14–1.37 |
| No ® | 1 | 1 | ||
|
| ||||
| Yes | 1.25 | 1.10–1.42 | 1.40 | 1.24–1.59 |
| No ® | 1 | 1 | ||
|
| ||||
| Yes | 1.70 | 1.56–1.86 | 1.67 | 1.53–1.81 |
| No ® | 1 | 1 | ||
|
| ||||
| Yes | 1.80 | 1.60–2.01 | 1.81 | 1.61–2.03 |
| No ® | 1 | 1 | ||
|
| ||||
| Yes ® | 1 | 1 | ||
| No | 1.29 | 1.04–1.60 | 2.00 | 1.31–3.04 |
|
| ||||
| No ® | 1 | 1 | ||
| Mono | 1.10 | 0.94–1.29 | 1.18 | 1.03–1.36 |
| Dual/poly | 1.37 | 1.20–1.57 | 1.59 | 1.38–1.83 |
|
| ||||
| Yes | 1.18 | 1.07–1.30 | 1.14 | 1.06–1.23 |
| No ® | 1 | 1 | ||
|
| ||||
| Yes ® | 1 | |||
| No | 1.18 | 1.06–1.32 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsObesity, Physical Activity, Diet · School Health and Nursing Education · Smoking Behavior and Cessation
INTRODUCTION
The introduction of novel tobacco products, such as electronic cigarettes (ECs), has significantly transformed the global landscape of teenage tobacco consumption over the past decade. This shift has led to a notable rise in dual (use of two types of tobacco products) or polytobacco product use (use of three or more tobacco products), with ECs playing a central role in this trend^1,2^. The use of multiple tobacco products – referred to as poly use – is increasingly recognized as a significant public health concern^3,4^. Compared to conventional cigarettes, alternative tobacco products like e-cigarettes may pose a lower risk of exposing others to harmful substances. However, these products are often used in social settings, driven by appealing flavors, peer influence, and prevailing trends^5^.
Many adolescents are drawn to various tobacco products under the misconception that they are less harmful or can assist with smoking cessation^6^. For instance, a 2020 study found that 5.4% of Minnesota students had used multiple tobacco products in the past 30 days, most commonly combining ECs and conventional cigarettes (28.3%), followed by ECs and cigars (19.9%) and a mix of ECs, cigars, and cigarettes (10.2%)^7^. Similarly, the 2019 Korea Youth Risk Behavior Web-based Survey (KYRBWS) revealed that 53.1% of Korean adolescent smokers used a single tobacco product, while 24.8% used two, and 22.1% used more than two. Between 2016 and 2018, although conventional cigarette use among adolescent males remained steady, polytobacco use increased from 2.94% to 3.32%, and the proportion of smokers using multiple products rose from 30.4% to 35.4%^8^.
In Malaysia, Lim et al.^9^ found that 6.5% of school-going adolescents were dual or polytobacco users. Of these, 53.7% used both cigarettes and e-cigarettes, while 23.7% used cigarettes, e-cigarettes, and shisha^9^. The prevalence of dual/poly use was notably higher among males, older adolescents, Malays, natives of Sabah and Sarawak, those with lower perceived harm of tobacco use, individuals lacking tobacco education in school, and those exposed to secondhand smoke at home, outdoors, or in school.
The growing prevalence of dual tobacco use among adolescents is concerning, as it is associated with a heightened risk of nicotine dependence compared to single-product use. Young people are especially vulnerable to nicotine addiction, and those engaging in dual or poly use often display more intense dependence symptoms – such as cravings and urges – than exclusive users of conventional cigarettes^10,11^. Additionally, dual/poly users are more likely to engage in other risky behaviors, including the use of alcohol, cannabis, and other illicit substances^12^.
Tobacco use is also strongly linked to mental health challenges, particularly neuropsychiatric conditions such as depression^13^. Smoking can exacerbate depressive symptoms through stress, chronic health conditions, and the biological impact of nicotine^13^. Research shows that smoking is associated with increased anxiety and the onset of depressive symptoms in both adults^14,15^ and adolescents^16^. This finding is especially troubling during adolescence – a critical developmental stage – since behaviors formed during this period often persist into adulthood. Notably, around 75% of adolescents experiencing significant stress and depressive symptoms are likely to face depression later in life^17^.
Given this context, there is an urgent need for research on the effects of dual/poly tobacco use in Malaysia. Such research would equip policymakers with crucial evidence to formulate targeted youth smoking prevention strategies and provide healthcare professionals with local data to support health promotion efforts. Furthermore, it would enhance the global understanding of tobacco-related issues by contributing insights from a developing country facing health challenges for decades.
This study aims to examine dual and polytobacco use among adolescents in Malaysia and its association with mental health outcomes, particularly stress and depression. Based on existing literature, we hypothesize that both single and dual/polytobacco use have significant impacts on adolescent mental health. The study seeks to generate meaningful data on adolescent behavior and well-being by exploring these associations, potentially shaping future public health policies and interventions.
METHODS
Sample and study design
This is a secondary dataset analyses of the data from the National Health and Morbidity Survey 2017: Adolescent Health Survey (NHMS 2017: AHS). This study employed a cross-sectional and multistage sampling technique to get a representative sample of adolescents aged 13–17 years attending secondary schools in Malaysia. The initial phase entailed the stratification of Malaysian states, which was succeeded by additional stratification within each state according to urban and rural classifications. The Ministry of Education and Rural and Regional Development supplied the sampling frame utilizing 2016 school enrolment data. The primary sampling unit consisted of 212 secondary schools in Malaysia, chosen using systematic random sampling^18^. The secondary sampling unit was a selection of 4 to 10 classes from each chosen school using proportionate size sampling. All students from the selected class were invited to participate in the study. The sample size was calculated using a variance of interest of 3%, a margin of error of 3%, and a 95% confidence interval, using a design effect of 2 from the 2012 GSHS-Malaysia study. A non-response rate of 25% was projected, necessitating a sample size of 30496 respondents. Only 27497 were included in the analysis. Yielding a 90.1% response rate. The remaining 2999 (9.9%) were not included due to respondents refusing to participate in the study, being absent during the interview, or providing incomplete answers.
Active consent was used for data collection from the chosen respondents. A letter outlining the study’s aims, responder confidentiality, and the consent form was dispatched to parents/guardians via the school administration. Participation was permitted solely for respondents who submitted the completed consent form. Data were gathered in certain school zones without the involvement of school personnel before the survey session. The research assistants, who were instructed on the study’s aims, collected the data. Participation was optional, and participants were notified that their data would be utilized exclusively for research purposes. The study team assisted respondents with clarification on particular items in the questionnaire. The study protocol received permission from the Ministry of Health and the Ministry of Education in Malaysia, and ethical clearance was obtained from the Medical Research and Ethical Committee (NMRR-16-698-30042).
Instrument
The questionnaire was adopted from the Malaysia Global School Health Survey 2012, which had been validated in prior research. The dependent variables, depression and stress symptoms were evaluated using the validated Malay version of the DASS 21 questionnaire. Seven items were used to measure anxiety and depression symptoms, respectively. The instrument has shown high reliability among Malaysian youth (Cronbach’s alpha of 0.90 for stress and 0.917 for measuring depression symptoms), respectively^19^. Respondents were asked to rate how frequently they experienced certain feelings over the past week, e.g. stress (I tended to overreact to situations) and depression (I found it difficult to get motivated to do things), with response options ranging from ‘never’ (0) to ‘almost always’ (3). The scores were then multiplied by 2. Respondents who scored between 0 and 13 were classified as not experiencing stress symptoms, whilst those who scored 10 or higher were categorized as having depressive symptoms during the last seven days^20^.
Variables
The independent variables are current tobacco status, which was measured by asking, ‘During the last 30 days: 1) Did you smoke cigarettes?; 2) Did you use traditional hand-rolled cigarettes?; 3) Did you use roll-your-own cigarette paper?; 4) Did you use a cigar?; 5) Did you use pipe smoking?; 6) Did you use an e-cigarette or vape?; 7) Did you use chewing tobacco?; and 8) Did you use snuff?’. The respondents who responded ‘no’ to all of the items were classified as ‘tobacco non-users’ those who answered ‘yes’ to any single item were categorized as ‘mono tobacco users’, and the respondents who answered ‘yes’ to any two or more items were classified as ‘dual/poly users of a tobacco product’.
Covariates
Gender, ethnicity (Malay, Chinese, Indian, Bumiputra Sabah, Bumiputra Sarawak, and others), age group (13–15 years, 16–17 years), parental/guardian marital status (married, divorced), history of physical attack at least once during last 12 months (yes, no), involvement in physical fights at least once during previous 12 months (yes, no), the experience of physical abuse at least once during last 12 months (yes, no), the experience of verbal abuse at least once during previous 12 months (yes, no), experience of bullying at least once during last 12 months (yes, no), exposure to secondhand smoke (SHS) in the past week (yes, no), parental supervision most of the time (yes, no), and have close friend(s) (yes, no).
Statistical analysis
The data underwent two rounds of cleaning to ensure quality: first by a research team member in the field, and then by the research management team at the institutional level. We randomly selected 10% of the data and compared it with the hard copy records to verify consistency. Frequency analysis was performed on each variable to identify missing or outlier values. The data were weighted according to the selection probabilities, considering the inverse probability of selecting each school, the inverse of selecting each classroom, and non-response adjustment factors at both the school and student levels, calculated by classroom. Descriptive statistics were used to summarize the sociodemographic characteristics of the participants. A chi-squared analysis examined the relationship between exposure and the dependent variable (exposure to SHS)^16^. The multivariable logistic regression models were fitted with all independent variables with a p≤0.25 in bivariate analyses. The main effect’s adjusted odds ratio (AOR) and 95% confidence interval (CI) were calculated. The model was also assessed for potential two-way (multiplicative) interactions between the independent variable (no, mono, and dual/poly tobacco use, with all the covariates). All statistical analyses were performed using the SPSS statistics program version 2018, with the complex samples module, applying a two-tailed test at a 95% significance level.
RESULTS
Males comprised about 50% of the sample, and over 60% of those surveyed were aged 13–15 years, and Malay. Nearly 20% of respondents were current tobacco users, more than half of the respondents were schooled in urban areas, 87.4% of respondents were from intact families, >95% of respondents had close friends, and only 13% of respondents reported supervision by the parents/guardian most of the time (Table 1).
The study found that 19.8% (95 % CI: 19.0–20.7) of respondents reported stress symptoms during the last seven days. A significantly higher proportion (1.52-fold) of stress symptoms exposure was observed among current dual/poly tobacco users (28.1%; 95% CI: 25.8–30.5 vs 18.4%; 95% CI: 17.5–19.4) than tobacco non-users. Female respondents of Indian and Chinese descent reported higher stress symptoms compared to their counterparts (male and Malay). In addition, respondents who were schooling in rural areas reported lower stress symptoms in the last week than those schooling in urban areas. Furthermore, those who had been bullied once, physically abused, or physically attacked at least once, reported higher significant levels of stress symptoms compared to those who had never been bullied/physically abused/physically attacked (Table 2).
Table 3 shows that nearly one-third of the respondents reported having depression symptoms during the last week (32.8%; 95% CI: 31.7–33.9). Almost half (46.8%) of the dual/poly tobacco users reported depression symptoms compared to mono-users and non-users of tobacco products (p<0.001). The other covariates, except the age group, also showed significant levels of depression symptoms.
Multivariable analysis was used to obtain the odds of dual/poly users of tobacco products (Table 4). The study showed that the odds of stress (AOR=1.37; 95% CI: 1.20–1.57) and depression (AOR=1.59; 95% CI: 1.38–1.83) symptoms were significantly higher among polytobacco users. There is no significant difference between stress symptoms between mono-users and non-users of tobacco products. However, dual users of tobacco products showed higher levels of stress and depression symptoms compared to mono-user and non-tobacco users.
Significant two-way interaction was found for stress symptoms between ethnicity and dual/poly use (Figure 1), and the age group of respondents and dual/poly use of tobacco product (Figure 2), whilst ethnicity and dual/poly user supervision most of the time by parents/guardians and dual/poly user for depression symptoms, Figures 3 and 4 (see also Supplementary file).
Interaction between tobacco users and parental supervision most of the time with depression symptom among school-going adolescents who participated in the National Health and Morbidity Survey: Adolescent Health Survey (NHMS: AHS) 2017
Interaction between tobacco users and ethnic groups with depression symptoms among school-going adolescents who participated in the National Health and Morbidity Survey: Adolescent Health Survey (NHMS: AHS) 2017
Interaction between tobacco users and age groups with stress symptoms among school-going adolescents who participated in the National Health and Morbidity Survey: Adolescent Health Survey (NHMS: AHS) 2017
Interaction between tobacco users and ethnic groups with stress symptoms among school-going adolescents who participated in the National Health and Morbidity Survey: Adolescent Health Survey (NHMS: AHS) 2017
DISCUSSION
This study investigated the association between dual/poly tobacco use and stress and depression symptoms among secondary school adolescents in Malaysia. The findings suggest that individuals who use one, two, or multiple types of tobacco are more prone to mental health issues than non-smokers, with polytobacco use being primarily linked to a greater frequency of mental health concerns. Dual/poly users of tobacco products showed higher significant stress and depression symptoms during the last seven days compared to non-users of tobacco. This finding is consistent with the finding of Buheit et al.^15^ who reported that the use of tobacco products increased stress levels by 69% among the general population in Denmark. This finding might because nicotine dependence is higher among dual/poly tobacco users than among single tobacco users and non-users^21^. Given that nicotine dependence is linked to psychological distress^22^, the findings of this study may be explained by the deprivation reversal model, whereby nicotine abstinence is stressful, and nicotine exposure seems to increase stress levels and exacerbate mood disturbances by inducing changes in neural pathways and neurotransmitter systems that are implicated in mood regulation^23,24^.
The proportion of individuals experiencing depressive symptoms was significantly higher among dual or polytobacco users (46.8%; 95% CI: 43.4–50.2) compared to those who used only one type of tobacco product (35.6%; 95% CI: 32.8–38.4), and non-users (30.2%; 95% CI: 29.1–31.3). A clear dose-response relationship was observed, indicating that the number of tobacco products used was positively associated with both the prevalence and odds of depressive symptoms. These findings are consistent with Kwon et al.^16^ who reported a similar trend among Korean youth, where depression symptoms increased from 24.3% in non-users to 49.9% in polytobacco users. The adjusted odds ratios for depression also increased with the number of products used, from 1.58 for single-product users to 1.81 for dual users and 2.18 for polytobacco users.
This pattern aligns with earlier research by Pasco et al.^24^, which found an increased risk of major depressive disorder among smokers (age-adjusted OR=1.46; 95% CI: 1.03–2.07), with the odds more than doubling for heavy smokers (>20 cigarettes/day). Similarly, Needham^25^, in a longitudinal study of 10828 US adolescents, reported that higher initial cigarette use was associated with more significant increases in depressive symptoms over time. Both male and female adolescents with higher levels of initial substance use consistently reported elevated depressive symptoms across all measured time points. The systematic review of Fluharty et al.^14^ identified 51 studies linking tobacco use to depression symptoms, further supporting our findings. Kwon et al.^16^ further emphasized that polytobacco users were particularly susceptible to increased depressive symptoms. Additionally, a recent review of substance use and mental health among adolescents in the US and Canada found that smokers were 1.65 times more likely to experience depression and 2.21 times more likely to suffer from anxiety compared to non-smokers^26^. Consistent findings were also reported by Guo and Yan^27^ based on data from the National Health and Nutrition Examination Survey (2005–2018) in the United Kingdom, where smokers had the highest likelihood of experiencing depression (OR=1.94; p<0.01). A significant positive correlation was also found between daily smoking and depression (OR=1.66, p for trend <0.01)^27^. These results are further supported by the Population Assessment of Tobacco and Health (PATH) Study, which analyzed data from 13617 US youth aged 12–17 years and found that tobacco users were significantly more likely to report internalizing problems, including depressive symptoms (AOR=1.6; 95% CI: 1.4–1.8)^28^. As the number of tobacco products used increased, the severity of these mental health issues also worsened. The higher likelihood of depression among mono-users and polytobacco users may be explained by both biological and environmental factors. First, neurobiological research shows that nicotine exposure affects the dopamine system, both acutely and chronically, which can lead to long-term abnormalities in dopamine transport and lower dopamine levels, increasing the risk of depression^29^. Second, frequent tobacco use can be indicative of a stressful home or work environment. Chronic stress has been shown to exacerbate depression by impairing neuroplasticity and producing abnormal levels of neurotrophic factors^30^. Structural brain changes, such as loss of dendritic spines and synapses and reduced dendritic branching, have been linked to long-term stress and depression^31^. Smoking is also associated with various long-term medical disorders, such as asthma, which may predispose adolescents to develop depressive symptoms^32^.
This study found a significant interaction between age groups and tobacco users, where adolescents aged 13–15 years showed lower stress levels compared to their counterparts aged 16–17 years. Still, younger adolescents who used mono and dual/poly tobacco products showed higher stress levels. The finding of higher stress levels is in line with the literature, which states that adolescents aged ≥15 years face more new challenges in early adolescence^33^. Still, the use of tobacco products changes this situation. We postulate that this may be because adolescents aged 13–15 years are more addicted to nicotine since adolescents who start smoking at a younger age tend to be more addicted to tobacco products^34^; apart from that, this may also be due to their difficulty in obtaining tobacco products like their counterparts aged 16–17 years^35^, which may contribute to the stress levels faced by them given the level of addiction they face.
Our study also found that adolescents whose are always supervised by parents/guardians and who were dual/polytobacco users showed higher levels of depression. This finding may be due to respondents who were dual/polytobacco users knowing that their parents disapprove of their behavior and regular supervision makes them feel more anxious and afraid that their parents/guardians will understand their behavior causes anxiety and contributes to the depression symptoms experienced. However, our postulation should be investigated and refined in future studies^36^ (Wang et al.^16^). In addition, a significant interaction was found to occur on the dependent variable (stress and depression symptoms) due to respondents of Chinese descent showing high levels of stress and depression symptoms when using single tobacco products. Still, the levels of stress and depression symptoms decreased among adolescents who use dual/polytobacco products. In contrast, respondents from other ethnicities who use dual/polytobacco products showed increased stress and depression symptoms. These findings require an in-depth culturally qualitative study among adolescents who are single or dual/polytobacco users to be conducted in future studies. In all cases, reverse causality cannot be ruled out.
Limitations
This study has several limitations. We used secondary data obtained through a cross-sectional design and self-reporting, which may lead to inaccuracies, as students could conceal their smoking behaviors and fail to report them accurately. As the data on tobacco use were self-reported, this may cause recall or response bias. Additionally, it is unclear whether polytobacco use is associated with all mental health-related variables, and cross-sectional studies are limited in their ability to establish causal relationships. The analysis is also limited by the inability to fully control residual confounding factors (such as underlying mental health problems). In addition, this study lacks biochemical validation to confirm smoking status, which means there may have been under-reporting of tobacco use.
Additionally, since the data were collected in 2017, they may not accurately reflect the current trends in dual/polytobacco use among youth in Malaysia^16^. Furthermore, the residual confounding was not controlled for and, lastly, the findings only apply to Malaysian school-going adolescents, and generalization cannot be applied to youth in other countries. However, a prior study in Malaysia found consistency between self-reported tobacco use and exhaled carbon monoxide levels when respondents’ anonymity and confidentiality were assured. Despite these limitations, the study highlights the association between increased dual/ polytobacco use and mental health issues among adolescents in Malaysia, where school-based health education on adolescent smoking is currently being implemented^16^.
CONCLUSIONS
Dual and polytobacco use was linked to mental health risks during adolescence. Dual and polytobacco users are exposed to higher levels of nicotine, which may lead to the use of other tobacco products, creating a cycle of increased nicotine consumption and further mental health risks. This behavior may also serve as a gateway to more serious drug use^37^. Understanding the broader implications of polytobacco use in adolescents is essential for addressing these issues.
Supplementary Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bhatnagar A, Whitsel LP, Blaha MJ, et al. New and emerging tobacco products and the nicotine endgame: the role of robust regulation and comprehensive tobacco control and prevention: A presidential advisory from the American Heart Association. Circulation. 2019;139(19):e 937-e 958. doi:10.1161/CIR.000000000000066930862181 · doi ↗ · pubmed ↗
- 2Njie GJ, Kirksey Jones C, Jacques N, et al. Changes in tobacco product use among students aged 13 to 15 years in 34 countries, Global Youth Tobacco Survey, 2012-2020. Prev Chronic Dis. 2023;20:E 68. doi:10.5888/pcd 20.22041037535901 PMC 10763619 · doi ↗ · pubmed ↗
- 3Sugiyama T, Tabuchi T. Use of multiple tobacco and tobacco-like products including heated tobacco and e-cigarettes in Japan: a cross-sectional assessment of the 2017 JASTIS study. Int J Environ Res Public Health. 2020;17(6):2161. doi:10.3390/ijerph 1706216132213924 PMC 7143444 · doi ↗ · pubmed ↗
- 4Ma C, Xi B, Li Z, et al. Prevalence and trends in tobacco use among adolescents aged 13-15 years in 143 countries, 1999-2018: findings from the Global Youth Tobacco Surveys. Lancet Child Adolesc Health. 2021;5(4):245-255. doi:10.1016/S 2352-4642(20)30390-433545071 · doi ↗ · pubmed ↗
- 5King BA. Flavors are a major driver of the youth e-cigarette epidemic. Am J Public Health. 2020;110(6):773-774. doi:10.2105/AJPH.2020.30567032374696 PMC 7204467 · doi ↗ · pubmed ↗
- 6Jankowski M, Krzystanek M, Zejda JE, et al. E-cigarettes are more addictive than traditional cigarettes-a study in highly educated young people. Int J Environ Res Public Health. 2019;16(13):2279. doi:10.3390/ijerph 1613227931252671 PMC 6651627 · doi ↗ · pubmed ↗
- 7Helgertz SR. Teens and tobacco in Minnesota: highlights from the 2020 Youth Tobacco Survey. Minnesota Department of Health. 2021. Accessed January 10, 2025. https://www.health.state.mn.us/communities/tobacco/data/docs/2020 mytsreport.pdf
- 8Lee ES, Paek YJ. Prevalence and correlates of the dual use of conventional and electronic cigarettes among Korean adolescents: 2016-2018 Korean Youth Risk Behavior Survey. J Korean Soc Res Nicotine Tob. 2020;11(2):64-74. doi:10.25055/JKSRNT.2020.11.2.64 · doi ↗