Mucosal polyposis syndrome mimicking a rectal tumour
Wei Ming Ong, Dhaval Joshi, Suat Chin Ng

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
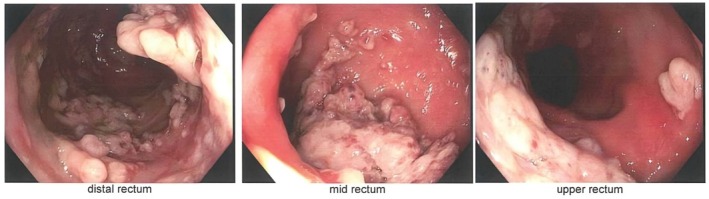 Figure 1
Figure 1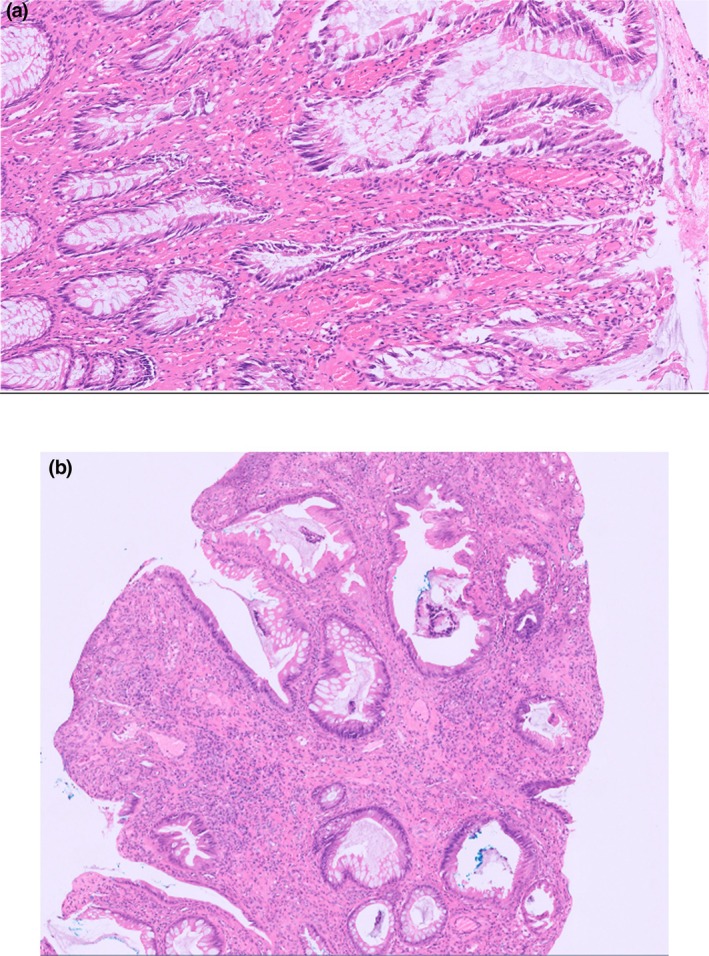 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic factors in colorectal cancer · Gastrointestinal Tumor Research and Treatment · Aortic Thrombus and Embolism
19‐year‐old male presented with a 2.5‐year history of per rectal bleeding associated with defecation on the background of chronic constipation.
Per rectal examination revealed a moderately gaping anus with a small degree of full‐thickness rectal prolapse on bearing down and a villous‐like lesion palpated above the anorectal junction. An urgent colonoscopy showed multiple carpet‐like lesions extending from the dentate line to the rectosigmoid junction (Fig. 1). Initial biopsies identified these as inflammatory polyps, with no evidence of adenomatous or malignant changes, and no features suggestive of an underlying inflammatory bowel disease.
A repeat endoscopy with large biopsies of the lesion was taken once more due to concern of a more sinister pathology. Histology demonstrated an ulcerated polypoid inflamed granulation tissue with features of mucosal prolapse (Fig. 2). He subsequently underwent a laparoscopic ventral rectopexy to correct the prolapse.
Mucosal prolapse syndrome (MPS) is an umbrella term for a broad range of conditions that stem from prolapsing mucosa.1 The most common entity of MPS is solitary rectal ulcer syndrome (SRUS) but other less‐known entities include proctitis cystica profunda (PCP) and inflammatory cloacogenic polyp.2 The incidence of MPS is estimated to be 1 in 100 000 and predominantly affects young adults.1, 3 The theorized pathogenesis of SRUS is due to excessive straining during bowel evacuation, leading to increased intra‐rectal pressures. The anterior wall of the rectal mucosa forcibly prolapses through the anal canal, which is paradoxically closed due to contraction of the puborectalis muscle. Recurrent trauma to rectal mucosa leads to inflammation and oedema, with the subsequent onset of ischaemia and regeneration resulting in the formation of either ulceration or mucosal polyposis.4
Clinical features of MPS include bleeding, tenesmus, constipation, passive mucus discharge, and anal itching. Endoscopic appearances of MPS vary from a shallow ulcerating lesion on a bed of erythematous mucosa to multiple ulcerative lesions or polypoid lesions.5 These polyps can mimic haemorrhoids, solitary rectal ulcer, villous adenoma, inflammatory bowel disease, or anorectal carcinoma. The macroscopic appearance of SRUS can be classified into ulcerative (55%), polypoid (24%) and flat (21%).6 In our patient, he had multiple polypoidal lesions throughout the lower rectum that appeared malignant at first glance.
Careful histopathological examination of the polyps is important in the diagnosis of mucosal prolapse syndrome due to its varied histological appearance and its ability to mimic other pathological lesions. Common features of MPS include glandular cystic dilation, ulceration, glandular architectural aberrations, thickening and disruption of the muscularis mucosae, and muscularisation of the lamina propria, resulting in characteristic fibromuscular obliteration of the lamina propria with disorientation of muscle fibres.7 The lamina propria may be oedematous and often shows increased numbers of fibroblasts.8
Treatment of MPS requires a multi‐disciplinary effort and may involve a surgical approach to correcting mucosal prolapse.
MPS is a mimicry for various pathological lesions. A meticulous history and examination, paired with a thorough endoscopic and histological examination of the biopsy specimens, are necessary to achieve a diagnosis.
Author contributions
Wei Ming Ong: writer, methodology, editing. Dhaval Joshi: editing. Suat Chin Ng: conceptualisation, supervision, editing.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brosens LA , Montgomery EA , Bhagavan BS , Offerhaus GJ , Giardiello FM . Mucosal prolapse syndrome presenting as rectal polyposis. J. Clin. Pathol. 2009; 62: 1034–1036.19861563 10.1136/jcp.2009.067801 PMC 2853932 · doi ↗ · pubmed ↗
- 2Tendler DA , Aboudola S , Zacks JF , O'Brien MJ , Kelly CP . Prolapsing mucosal polyps: an underrecognized form of colonic polyp: a clinicopathological study of 15 cases. Am. J. Gastroenterol. 2002; 97: 370–376.11866275 10.1111/j.1572-0241.2002.05472.x · doi ↗ · pubmed ↗
- 3Wong YP , Kabincong C , Jabar MF , Tan GC . Rectal polyposis in mucosal prolapse syndrome. Diagnostics (Basel) 2022; 12: 966.35454014 10.3390/diagnostics 12040966 PMC 9029702 · doi ↗ · pubmed ↗
- 4Zhu QC , Shen RR , Qin HL , Wang Y . Solitary rectal ulcer syndrome: clinical features, pathophysiology, diagnosis and treatment strategies. World J. Gastroenterol. 2014; 20: 738–744.24574747 10.3748/wjg.v 20.i 3.738PMC 3921483 · doi ↗ · pubmed ↗
- 5Sharara AI , Azar C , Amr SS , Haddad M , Eloubeidi MA . Solitary rectal ulcer syndrome: endoscopic spectrum and review of the literature. Gastrointest. Endosc. 2005; 62: 755–762.16246692 10.1016/j.gie.2005.07.016 · doi ↗ · pubmed ↗
- 6Chiang JM , Changchien CR , Chen JR . Solitary rectal ulcer syndrome: an endoscopic and histological presentation and literature review. Int. J. Colorectal Dis. 2006; 21: 348–356.16133006 10.1007/s 00384-005-0020-6 · doi ↗ · pubmed ↗
- 7Singh B , Mortensen NJ , Warren BF . Histopathological mimicry in mucosal prolapse. Histopathology 2007; 50: 97–102.17204024 10.1111/j.1365-2559.2006.02552.x · doi ↗ · pubmed ↗
- 8Ball CG , Dupre MP , Falck V , Hui S , Kirkpatrick AW , Gao ZH . Sessile serrated polyp mimicry in patients with solitary rectal ulcer syndrome: is there evidence of preneoplastic change? Arch. Pathol. Lab. Med. 2005; 129: 1037–1040.16048395 10.5858/2005-129-1037-SSPMIP · doi ↗ · pubmed ↗