Low Visual Acuity Among Children in Public Schools in the Northeast of Brazil: A Cross-Sectional Study
Lucas Neves de Oliveira, Matheus Gomes Reis Costa, Isadora Oliveira Santiago Pereira, Isabele Carolina Tokumoto, Joao Lucas de Magalhães Leal Moreira, Matheus Carneiro Leal Freitas, Clarissa Silva Sampaio, Mateus Neves de Oliveira, Jose Bessa Junior

TL;DR
A study in Brazil found that nearly 30% of public school children in the Northeast had low visual acuity, with few using glasses, highlighting the need for better eye care access.
Contribution
This study provides new prevalence data on low visual acuity in Brazilian public schoolchildren and identifies associated factors like gender and screen use.
Findings
Low visual acuity was found in 29.3% of 358 children.
Only 7.6% of children with low visual acuity used glasses.
Factors associated with low visual acuity included female gender and white ethnicity.
Abstract
Objective This study describes the prevalence of low visual acuity (LVA) in public school students from a city in the interior of the Northeast region of Brazil. Methods This was an observational, cross-sectional, exploratory study. The sample consisted of schoolchildren from the second to the fourth grade of five public schools in Feira de Santana, Bahia, Brazil. Data collection was carried out in the schools themselves, with a sociodemographic and clinical questionnaire applied and visual acuity (VA) measured using the Snellen “E” optotype chart. LVA was defined as uncorrected VA < 20/25 in at least one eye. Results The sample consisted of 358 children, with a median age of nine (IQR 8-10) years, of which 189 (52.9%) were female, and 169 (47.2%) were male. A total of 248 (69.3%) individuals had never been to an ophthalmologist. LVA was found in 105 (29.3%) schoolchildren, and of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
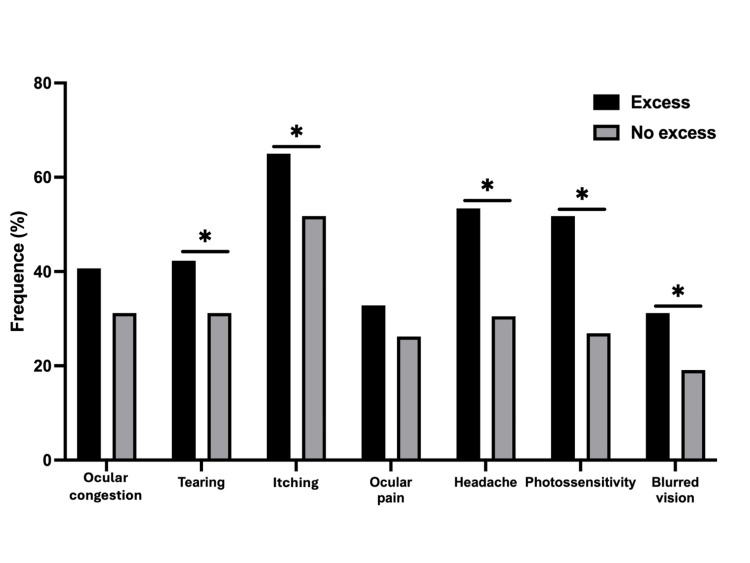 Figure 1
Figure 1| Baseline characteristics | n (%) |
| Gender | |
| Male | 169 (47.2) |
| Female | 189 (52.8) |
| Grade | |
| 2nd | 136 (38) |
| 3rd | 119 (33.2) |
| 4th | 103 (28.8) |
| Race (self-reported) | |
| Black | 106 (29.6) |
| Brown | 205 (57.3) |
| White | 39 (10.9) |
| Yellow | 4 (1.1) |
| Indigenous | 4 (1.1) |
| Family income | |
| ≥3 minimum wage | 13 (3) |
| Between 1 and 3 minimum wages | 104 (29.1) |
| ≤1 minimum wage | 241 (67.3) |
| Residence | |
| Urban area | 331 (92.5) |
| Rural area | 27 (7.5) |
| Prematurity | |
| No | 323 (90.2) |
| 32 to 36 weeks | 30 (8.4) |
| 28 to 31 weeks | 4 (1.1) |
| ≤28 weeks | 1 (0.3) |
| Systemic disease | |
| Total | 52 (14.5) |
| Respiratory diseases | 28 (7.8) |
| Rhinitis/sinusitis | 14 (3.9) |
| Asthma | 13 (3.6) |
| Previous consultation with an ophthalmologist | |
| No | 248 (69.3) |
| Yes | 110 (30.7) |
| Use of glasses | |
| Previous or current | |
| No | 328 (91.6) |
| Yes | 30 (8.4) |
| Current | |
| No | 348 (97.2) |
| Yes | 10 (2.8) |
| VA classification | Uncorrected VA | Current glasses users |
| n (%) | n (%) | |
| Normal vision (≥20/25), both eyes | 253 (70.7) | 2 (0.8) |
| Normal vision (≥20/25), one eye only | 29 (8.1) | 1 (3.4) |
| Mild visual impairment (<20/25 and ≥20/63), better eye | 56 (15.6) | 3 (5.3) |
| Moderate visual impairment (<20/63 and ≥20/160), better eye | 14 (3.9) | 2 (14.3) |
| Severe/profound visual impairment (<20/160 and ≥20/1000), better eye | 6 (1.7) | 2 (33.3) |
| Total | 358 (100) | 10 (2.8) |
| Variables | OR | 95% CI | p-value |
| Female | 2.12 | 1.32-3.41 | 0.002 |
| Age > 11 years | 2.47 | 0.85-7.24 | 0.098 |
| White race | 2.57 | 1.31-5.05 | 0.006 |
| Family income > 1 minimum wage | 1.25 | 0.77-2.02 | 0.362 |
| Prematurity | 1.12 | 0.53-2.37 | 0.774 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsImpact of Light on Environment and Health · Ophthalmology and Visual Impairment Studies
Introduction
Vision, among the five senses, is the most dominant and the primary means of integrating the individual with the external environment, with a large part of knowledge being acquired visually [1]. Visual problems impair learning and social interactions, compromising intellectual, academic, and professional development, as well as communication and socialization skills [2].
School-aged children are particularly affected by vision impairment. Initially, visual problems may not be perceived by the family, mainly due to the absence of signs or complaints. Over time, significant visual effort becomes evident in the teaching-learning process [3]. If persistent, these problems affect the child’s academic performance and socialization [4].
According to the World Health Organization, there are approximately 1.4 million children with visual impairment worldwide, with 90% living in developing countries. Each year, 500,000 children become blind, and about 80% of childhood blindness causes are preventable or treatable [1]. It is estimated that the prevalence of childhood blindness in Brazil is 4/10,000 children [5]. Concerning reversible blindness, the leading cause of childhood blindness, uncorrected refractive errors are the primary cause of low vision in school-aged children [1].
In Brazil, there is limited data on the prevalence of visual impairment among schoolchildren, and to our knowledge, no data are available for Bahia. Additionally, many studies are outdated, and most were conducted in the South and Southeast regions. A study conducted in Sorocaba, São Paulo, showed a prevalence of low visual acuity (LVA) of 13.1% in public school children [6]. In Londrina, Paraná, the prevalence of LVA was demonstrated in 17.1% of public school students [7]. In Patos de Minas, Minas Gerais, the prevalence of visual impairment in schoolchildren was 20.9% [8].
Early diagnosis of visual disorders has been suggested as a strategy to prevent future problems, including amblyopia, and alterations in neuropsychomotor and social development [9]. From a public health perspective, routine visual acuity (VA) assessment is essential for promoting eye health, contributing to reducing high levels of school dropout and poor academic performance [6,10].
Given the importance of early diagnosis, the scarcity of data in national literature, especially in the Northeast, and the absence of studies in Bahia, the aim of this study was to evaluate the prevalence of LVA in public school children in Feira de Santana, Bahia. An initial version of this article was previously published on a preprint server [11].
Materials and methods
Study population
We conducted a cross-sectional study between August 2022 and May 2023. The study participants were elementary school students from the second to the fourth grade, regularly enrolled in five municipal public schools located in Feira de Santana, Bahia, Brazil. To ensure a representative and randomized sample, we first obtained a list of all municipal public schools from the Municipal Health Department. Using a random number generator, we randomly selected five schools located in socioeconomically diverse areas of the city.
This observational study was approved by the Research Ethics Committee of the State University of Feira de Santana on May 1, 2022, under protocol no. 56993722.5.0000.0053, position statement 5.380.168. Written informed consent was obtained from the parents or guardians of the children.
Data collection
Data were collected at the schools by medical students from the Visual Disorders Combat League (LCDV) of the State University of Feira de Santana (UEFS), adequately trained by ophthalmologists at an eye hospital. Initially, a sociodemographic and clinical questionnaire was administered to parents/guardians, including reports of recurring ophthalmic signs/symptoms and excessive screen use.
VA was assessed using the Snellen "E" optotype chart, positioned 6 m away at a height of 1.5 m. All children were first evaluated without optical correction; for those who already used glasses, the test was repeated with their habitual correction [7,12-14].
Definitions and classifications
VA was classified as normal vision (VA ≥ 20/25 or 0.8), mild visual impairment (VA < 20/25 or 0.8 and ≥ 20/63 or 0.3), moderate visual impairment (VA < 20/63 or 0.3 and ≥ 20/160 or 0.125), and severe/profound visual impairment (VA < 20/160 or 0.125 and ≥ 20/1000 or 0.02) [14,15]. LVA was defined as uncorrected VA < 20/25 in at least one eye [6-8,16].
Excessive screen use was defined as greater than four hours per day, based on the parent-reported single-question assessment. Screens included are cell phones, tablets, computers, and televisions.
Statistical analysis
Data are presented as absolute values, frequencies, medians, and interquartile ranges (IQRs). Categorical variables were compared using the chi-square test, and the odds ratio (OR) was used as a measure of association for categorical variables. A p-value < 0.05 was considered statistically significant, and a 95% confidence interval (CI) was presented as a measure of precision. Statistical analyses were performed using GraphPad Prism version 10.2.2 (GraphPad Software Inc., San Diego, CA).
Results
Of the initial 361 children enrolled, 358 were included in the final analysis. One was excluded due to a developmental disorder, and two refused to participate. The median age was nine (IQR 8-10) years, and 189 (52.8%) were female. A total of 311 (86.9%) self-identified as Black/Brown, and 241 (67.3%) had a family income ≤ 1 minimum wage. A total of 248 (69.3%) children had never visited an ophthalmologist.
Thirty (8.4%) children reported previous or current use of glasses. Of these, 10 (33%) were current users, and the other 20 (67%) had stopped using them. The sample characteristics are detailed in Table 1.
Prevalence of LVA
LVA (uncorrected VA < 20/25 in at least one eye) was found in 105 (29.3%) students. Of these, 7.6% (8/105) were current glasses users, and after correcting VA with glasses, six still had visual impairment in at least one eye. The distribution of VA is detailed in Table 2.
In the univariate analysis, the variables associated with LVA were female gender (OR 2.12; 95% CI 1.32-3.41, p = 0.002) and white race (OR 2.57; 95% CI 1.31-5.05, p = 0.006). Age, family income, and prematurity were not associated (Table 3).
Vision and excessive screen use
In the analysis of these aspects, our sample was reduced to 330 students due to incomplete data in this aspect for 28 subjects.
Excessive screen use was found in 189 (57.3%) children. LVA was observed in 60 (31.7%) students with excessive screen use and in 36 (25.5%) without excessive screen use (OR 1.35; 95% CI 0.83-2.19, p = 0.222).
Tearing was reported in 40.2% of children with excessive screen use versus 28.4% in the no-excess group (OR 1.62; 95% CI 1.02-2.56; p = 0.040). Itching was significantly more common in the excessive group (56.6% vs. 41.2%; OR 1.73; 95% CI 1.11-2.71; p = 0.015), as were headache (52.4% vs. 29.4%; OR 2.62; 95% CI 1.65-4.14; p < 0.001), photosensitivity (58.7% vs. 30.4%; OR 2.92; 95% CI 1.83-4.66; p < 0.001), and blurred vision (41.3% vs. 26.5%; OR 1.92; 95% CI 1.14-3.22; p = 0.014). However, no statistically significant associations were found for ocular congestion (OR 1.52; 95% CI 0.96-2.40; p = 0.076) or ocular pain (OR 1.37; 95% CI 0.85-2.22; p = 0.199), despite a higher prevalence in the excessive screen use group. These findings are summarized in Figure 1.
*Visual signs/symptoms in schoolers with or without excessive screen use (n = 330)p < 0.05
Discussion
The prevalence of LVA in public school children in Feira de Santana, Bahia, was 29.3%. In national literature, the prevalence of LVA in schoolchildren ranged from 9% to 20.87% [6-8,12,14,16]. Our study found a higher prevalence of LVA than previous literature data. We believe several probable factors may explain this significant difference: (1) specific local socioeconomic challenges in public schools in Feira de Santana, Bahia, limiting access to eye care; (2) more sensitive screening methods used in our study, identifying more cases; and (3) differences in sample characteristics compared to previous studies, including age, race, and gender.
The prevalence of current glasses use in this study was 2.8%. In previous studies in Brazil, the prevalence ranged from 2.4% to 4.5% [6,7,12,14,16]. Regarding current glasses use in children with LVA, our study revealed a prevalence of 7.6%, while previous national studies showed a prevalence ranging from 10.52% to 40% [6,8,12,14].
In addition to the higher prevalence of LVA in the studied population, a lower prevalence of current glasses use was demonstrated in children with low vision. It is noteworthy that approximately 70% of the students had never had an ophthalmological consultation. The Brazilian Society of Pediatric Ophthalmology recommends a complete routine ophthalmological consultation from six to twelve months of age and another consultation from three to five years of age, with the frequency of subsequent consultations being determined by the ophthalmologist, usually on an annual basis [17]. The findings reinforce the importance of conducting visual screening actions through active search in our region, as well as creating strategies to facilitate access to ophthalmological consultations and glasses.
The early detection and treatment of visual impairment in infants aim to ensure normal physical and cognitive development. Motor development and communication ability are impaired in infants with visual impairment because gestures and social behaviors are learned through visual feedback [1,5]. There is an additional risk of developing amblyopia, characterized by low vision due to abnormal development of the visual cortex during childhood, which can affect one or both eyes [9,18]. Amblyopia should ideally be treated by the age of seven to eight. Some studies indicate benefit in treatment at older ages, but there is consensus that early correction provides the best prognosis [19].
From a public health perspective, population investigation by ophthalmologists is unfeasible and costly, making routine visual screening by adequately trained non-medical personnel essential [5,20].
A low-cost strategy capable of enabling large-scale visual screening is training teachers to apply the VA test using the Snellen chart. Other authors have recommended and validated this strategy [3,6,20,21]. Based on these premises, the Visual Disorders Combat League was created in 2021 by medical students from the State University of Feira de Santana. Grounded on the university triad and focusing on extension, one of the league's objectives is to promote eye health for children lacking ophthalmological care in Feira de Santana/Bahia, and the surrounding region.
Factors associated with LVA in this study were female gender and white race. This association with female gender has been evidenced in other research [6]. No national studies associating ethnicity and LVA were found, but research in the United States showed that children who self-identified as black had worse VA [22,23]. Foreign literature also reports an association between family income and LVA [23,24], a relationship not demonstrated in this study. Further national studies are needed to better elucidate these factors.
LVA was found more frequently in subjects with excessive screen use (31.7% vs. 26.5%) compared to those without excessive use, although we did not find a statistically significant difference. However, we demonstrated an association between excessive screen use and some ophthalmological symptoms. There are still few studies on this topic in the literature, as the issue of screens is relatively recent, and the true impact on eye health is still unknown [25].
A recent meta-analysis revealed that excessive smartphone use can increase the chance of ocular symptoms such as blurred vision, as well as myopia, asthenopia, and ocular surface diseases [26]. Besides the neuropsychomotor and social benefits, restricting prolonged screen use seems to positively impact eye health, making parental involvement indispensable in monitoring and regulating excess [26-28].
This study has some limitations. In 2021, it was estimated that Feira de Santana had 16,364 children enrolled in the second to fourth grade in municipal schools [29]. Due to logistical difficulties in screening and team size limitations, we had a relatively small (n = 358) and non-probabilistic sample size. Additionally, the study's unicentric nature and the subjective method of defining screen time limit our external validity.
Despite these limitations, our study has important strengths. To our knowledge, this is the first study to assess the prevalence of LVA among public school children in our region. By focusing on a population that is often underrepresented in national data - children from public schools in socioeconomically vulnerable areas - we offer valuable insights that can help inform public health strategies. These findings highlight the need for early screening, access to eye care, and preventive measures within schools to reduce the risk of undiagnosed visual problems and prevent long-term impacts, such as amblyopia, that may become irreversible if not addressed in time.
Conclusions
LVA was identified in approximately 30% of public school children in the interior of Bahia, yet fewer than 10% of these children were currently using glasses. Alarmingly, around 70% had never undergone an ophthalmologic evaluation. Excessive screen use emerged as a significant concern, with potential harmful effects on children’s eye health.
Our study highlights the urgent need for active visual screening programs in schools, particularly in socioeconomically vulnerable regions, to detect visual problems early and prevent long-term consequences such as amblyopia. Additionally, the findings emphasize the importance of implementing community-level strategies to improve access to ophthalmologic care and provide affordable corrective lenses. By addressing these gaps, we can help ensure that children not only achieve better visual outcomes but also have improved educational and developmental opportunities.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World report on vision World Health Organization Geneva, Switzerland World Health Organization 2019 https://www.who.int/publications/i/item/world-report-on-vision
- 2Oral language assessment of children with visual impairments: an integrative literature review Audiol Commun Res Carvalho PHS Bagarollo MF Montilha RCI 6282023
- 3Vision screening for correctable visual acuity deficits in school-age children and adolescents Cochrane Database Syst Rev Evans JR Morjaria P Powell C 02201810.1002/14651858.CD 005023.pub 3PMC 649119429446439 · doi ↗ · pubmed ↗
- 4Language and communication development in preschool children with visual impairment: a systematic review S Afr J Commun Disord Mosca R Kritzinger A van der Linde J 062201510.4102/sajcd.v 62i 1.119PMC 584305126809155 · doi ↗ · pubmed ↗
- 5Guidelines for attention to ocular health in childhood: early detection and intervention for visual impairment prevention Brazil Ministry of Health Brasília, Brazil Brazil Ministry of Health 2013 https://bvsms.saude.gov.br/bvs/publicacoes/diretrizes_atencao_saude_ocular_infancia.pdf
- 6Prevalence of low visual acuity in public school's students from Brazil Rev Saude Publica Gianini RJ Masi Ed Coelho EC Oréfice FR Moraes RA 2012083820041512237510.1590/s 0034-89102004000200008 · doi ↗ · pubmed ↗
- 7Reduced visual acuity prevalence in first grade school children of elementary state public and private schools of Londrina Arq Bras Oftalmol Lopes GJA Casella AMB ChuíCA 659664652000
- 8Early detection and resolution of visual impairment in students from the city of Patos de Minas Rev Med Minas Gerais Figueiredo SO Roque ILF Guimarães IISM 5252015