Lipomatous Metaplasia in a Warthin Tumor: A Rare Histopathological Finding
Asiye Üzümcü, Melek Büyük, Beyza Nur Baysal, Neslihan Berker, Mine Güllüoğlu

TL;DR
This paper reports a rare case of a Warthin tumor with lipomatous metaplasia, highlighting its potential to be misdiagnosed as a lipomatous lesion.
Contribution
The paper contributes a rare histopathological case of lipomatous metaplasia within a Warthin tumor.
Findings
Lipomatous metaplasia in a Warthin tumor can resemble lipomatous lesions.
This feature is a potential diagnostic pitfall, especially in hypocellular samples.
Abstract
We present a case of Warthin tumor (WT) exhibiting lipomatous metaplasia. This rare histopathological feature can mimic lipomatous lesions, particularly in hypocellular samples, and should be recognized as a potential diagnostic pitfall. Recognition of this feature is important to avoid diagnostic errors.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
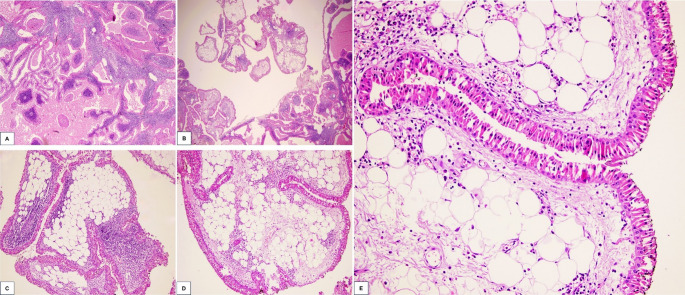 Figure 1
Figure 1- —Istanbul University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTumors and Oncological Cases · Vascular Malformations and Hemangiomas · Sarcoma Diagnosis and Treatment
Introduction
WT is the second most common benign salivary gland lesion, typically affecting middle-aged males and showing an increased incidence among smokers [1]. Although metaplastic changes can occur in WT, squamous metaplasia is the most frequently observed type, whereas mucinous metaplasia is considered rare [2].
Case Report
A 63-year-old male patient presented with a one-year history of a mass located inferior to the right ear. Ultrasonography of parotid glands revealed lobulated solid lesions with cystic degenerative changes, measuring 3.4 × 3 cm on the right and 4.5 × 2.1 cm on the left. Fine-needle aspiration biopsies (FNAB) of both parotid masses were consistent with WT. The patient subsequently underwent right superficial parotidectomy.
On macroscopic examination, the parotid gland measured 8.5 × 6 × 4 cm and contained a nodular, multilobulated, brown-colored mass measuring 4 × 3 × 2 cm, exhibiting hemorrhagic and cystic areas. Histopathological evaluation confirmed the diagnosis of WT, characterized by cystic spaces lined with bilayered oncocytic epithelium and accompanying lymphoid stroma (Fig. 1A). Notably, a 0.4 cm focus of mature adipocyte proliferation, consistent with lipomatous metaplasia, was identified within the tumor (Fig. 1B-E). The possibility of entrapped adipose tissue was considered; however, this was ruled out because the adipose focus was located within the tumor rather than at its periphery. Additionally, the adipose focus was surrounded by bilayered oncocytic epithelium and associated with lymphoid stroma, supporting its intratumoral origin.
Fig. 1. Histologic features of Warthin tumor with lipomatous metaplasia. Warthin tumor shows cystic spaces lined by bilayered oncocytic epithelium and prominent lymphoid stroma (A) (H&E, ×100). Foci of mature adipocyte proliferation within the tumor stroma, consistent with lipomatous metaplasia (B–E) (H&E, ×40, ×200, ×200, ×400, respectively)
Conclusion
Metaplastic changes in WT are uncommon, with reported incidence rates ranging from 0 to 7.6% in the literature [2]. Squamous metaplasia is the most frequently described subtype and is thought to be associated with prior FNAB [3]. To the best of our knowledge, the lipomatous metaplasia observed in this case represents the first example reported in the literature. The presence of adipocytes in FNAB or core biopsy of salivary glands may lead a diagnostic challenge, potentially resulting in non-diagnostic findings or misinterpretation as a lipomatous neoplasm. Therefore, clinicians and pathologists should be aware that lipomatous metaplasia can occur in WT.