Developmental delay increases risk for complications within 30 days of pediatric spinal fusion surgery
Haseeb E. Goheer, Zachary M. Johnson, Alexander R. Garcia, Brian Q. Truong, Alden H. Newcomb, Jonathan J. Carmouche

TL;DR
Children with developmental delays face higher risks of complications after spinal fusion surgery, according to a study using national surgical data.
Contribution
This study identifies developmental delay as an independent risk factor for postoperative complications in pediatric spinal fusion patients.
Findings
Developmental delay was associated with higher rates of surgical and medical complications.
Patients with developmental delay had a significantly increased risk of ICU stay and death.
The study provides evidence to improve preoperative risk assessment for pediatric spinal fusion.
Abstract
The aim of this study was to investigate whether developmental delay is a risk factor for postoperative complications following pediatric spinal fusion. The American College of Surgeons National Surgical Quality Improvement Program Pediatric database was queried to retrospectively identify patients who had undergone spinal fusions between 2016 and 2021. The study population was divided into two distinct groups 1) Patients with developmental delay 2) who have no delay. T-tests for continuous variables and chi-square tests for categorical variables were used to identify differences in perioperative characteristics between the two groups. Multivariable logistic regression analysis assessed the effect of preoperative developmental delay on post-operative surgical outcomes. A total of 32,621 pediatric spinal fusion patients were identified, of which 7,637 had developmental delay and 24,984…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
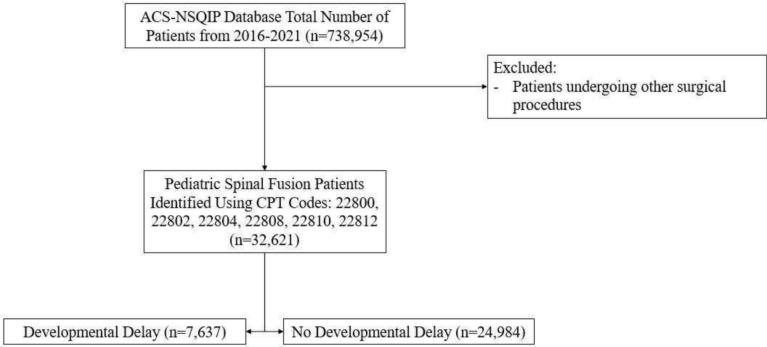 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsScoliosis diagnosis and treatment · Congenital Diaphragmatic Hernia Studies · Spinal Dysraphism and Malformations
Introduction
Spinal fusion is commonly indicated in the management of scoliosis [1, 2]. 2–3% or an estimated 6–9 million people in the United States (US) are affected by scoliosis [3] Of the 2–3% of the US population with scoliosis, more than 7500 pediatric patients will undergo surgical correction of their deformity [4]. These procedures can cost up to 180,000 per patient [5–7]. Previously published data in 2012 indicates that the costs associated with surgical correction of pediatric scoliosis are on the rise, with a national annual expenditure of $1.1 billion [6, 7]. Developmental delay is observed as a common comorbidity in pediatric patients undergoing spinal fusion [8]. Due to the heterogenous degrees of comorbidities associated with developmental delay, identifying its impact on surgical outcomes is important in risk stratifying patients and providing a more complete understanding of potential outcomes during the consent process.
Developmental delay has previously been identified as a risk factor in pediatric orthopaedic and spine procedures for postoperative complications, including infection, healthcare resource usage, and hospital readmission [9–11]. Previous investigations looking into pediatric patients undergoing treatment for open femoral shaft fractures and removal of hardware in orthopaedic procedures found developmental delay to be independently associated with increased risk of hospital readmission and increased risk of infection [10, 11]. Pediatric patients with developmental delay may present with additional challenges in relation to the complexity of their care such as requiring increased physician visits, emergency department visits, hospitalizations, and visits to other healthcare practitioners [12]. Although previous spine surgery research has shown the negative impact of intellectual disability and Down syndrome on surgical outcomes in pediatric spinal fusion, limited studies have investigated the connection between developmental delay and outcomes in pediatric spinal fusion procedures. A retrospective analysis of 23 pediatric patients with Down syndrome undergoing pediatric spinal fusion found that 52% experienced at least one postoperative complication, a higher rate than in children without developmental delay undergoing the same procedure ranging from 5 to 23% [9, 13–15]. The studies investigating how developmental delay impact pediatric spinal fusion outcomes have been limited by their smaller sample size or have been conducted at a single institution with non-representative samples of the national population [1, 9]. The purpose of our study is to compare demographic and comorbidity profiles with postoperative outcomes in children with and without developmental delay undergoing pediatric spinal fusion using a large multi-institutional database. To our knowledge, no studies have specifically evaluated developmental delay as an independent risk factor for unfavorable outcomes following pediatric spinal fusion. These findings will improve risk stratification for patients with developmental delay undergoing complex spinal fusion procedures.
Materials and methods
Study design and data sources
This is a retrospective study of patients in the American College of Surgeons National Surgical Quality Improvement Program Pediatric (ACS-NSQIP- Pediatric) database. The ACS-NSQIP-Pediatric is a national surgical database of data from hospitals providing pediatric care throughout the United States. The participating institutions have certified clinical reviewers responsible for verifying the authenticity of the data and the database has regular audits [16]. IRB approval was not requested as the database contains de-identified information.
Disclaimer
American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Study population
Data from 2016 to 2021 were reviewed to collect data on patients undergoing pediatric spinal fusion procedures. Patients were identified using the Current Procedural Terminology codes 22800, 22802, 22804, 22808, 22810, 22812. The identified and exclusions are outlined in the CONSORT flow chart (Fig. 1). Using unique case identifiers, the ACS-NSQIP Pediatric dataset was merged with the ACS-NSQIP Pediatric Spinal Fusion Procedure Targeted dataset. Patients not found in both datasets were excluded from the study. Patients identified in the database to have a developmental delay were assigned to the developmental delay cohort while all remaining patients were assigned to the no developmental delay cohort. Developmental delay, defined by impaired cognitive status, was a predefined variable in the ACS-NSQIP database. The clinical diagnosis of developmental delay was determined by certified clinical reviewers after electronic medical record review.Fig. 1. Flow diagram of the cohort selection process
Patient variables and outcomes of interest
Patient and clinical characteristics collected from the ACS-NSQIP-Pediatric database included demographic variables, medical comorbidities, intraoperative data, and postoperative outcomes within the first 30 postoperative days. The list of preoperative comorbidity variables includes: ventilator requirement, asthma, history of chronic lung disease (CLD), tracheostomy, esophageal or intestinal disease, prior cardiac surgery, cardiac risk factors, pulmonary abnormalities, impaired cognition status, seizure, intraventricular hemorrhage, steroid use within 30 days of surgery, nutritional support, bleeding disorder, hematological disorder, previous sepsis, childhood malignancy, and the American Society of Anesthesiologist (ASA) classification. Outcomes were categorized by the presence or absence of medical and surgical complications. Surgical complications included wound disruption, superficial surgical site infection (SSI), deep SSI, organ SSI, or wound dehiscence. Medical complications included pneumonia, unplanned intubation, renal insufficiency, acute renal failure, urinary tract infection (UTI), stroke with neurological deficit, seizure, nerve injury, cardiac arrest, bleeding transfusion, vein thrombosis, sepsis, Clostridioides difficile colitis, reoperation, extended length of stay or intensive care unit (ICU) stay. Extended hospital length of stay (LOS) was defined by a stay greater than or equal to two standard deviations above the mean.
Statistical analysis
Differences in pre- and peri-operative variables were compared between the developmental delay cohorts using t-test for continuous variables and chi-square tests for categorical variables. Multivariate logistic regression analyses were used to determine independent associations of developmental delay with the occurrence of medical and surgical complications, intensive care unit stay, and extended length of stay, within thirty days. We included preoperative variables with n > 10 and p < 0.05 from the covariate screening in the multivariate logistic regression. Given the large number of potential confounders, multivariate analyses were completed using model selection by Akaike information criterion in backward stepwise regression to isolate development delay as a risk factor while controlling for pre-operative comorbidities and demographic characteristics. Significant variables initially in the regression included age, sex, race, admission status, surgical approach, scoliosis type, ventilator dependence, asthma, chronic lung disease, oxygen support, tracheostomy, esophageal, gastric or intestinal disease, history of cardiac surgery, cardiac risk factors, pulmonary abnormalities, seizure, cerebral palsy, structural CNS abnormalities, neuromuscular disorder, intraventricular hemorrhage, steroid use, ostomy, pre-operative wound infection, nutritional support, sepsis prior to surgery, hematologic disorders, cardiovascular pulmonary resuscitation within seven days of surgery, transfusions, childhood malignancy, ASA class, type of fusion, and operative time. Significance was defined as p < 0.05. All statistical analyses were performed using the statistical coding program R version 4.3.3 (R, Vienna, Austria).
Results
Developmental delay and the overall pediatric spinal fusion population
A total of 32,621 pediatric spinal fusion patients were identified, of which 7,637 (23.4%) had developmental delay (Table 1). The developmental delay cohort was significantly younger (p < 0.001) and contained significantly more males compared to the control population (p < 0.001). Significant differences in comorbidities between the two groups were identified. Compared to the no developmental delay group, the developmental delay group had higher rates of most comorbidities with statistically significant associations. This list includes ventilator dependence (7.95%; p < 0.001), asthma (16.6%; p < 0.001), CLD (16.3%; p < 0.001), oxygen support (6.5%; p < 0.001), tracheostomy (6.8%; p < 0.001), history of cardiac surgery (9.9%; p < 0.001), severe cardiac risk factors (0.9%; p < 0.001), pulmonary abnormalities (20.8%; p < 0.001), seizure (40.9%; p < 0.001), cerebral palsy (38.5%; p < 0.001), structural CNS abnormalities (37.3%; p < 0.001), neuromuscular disorder (63.7%; p < 0.001), intraventricular hemorrhage (3.3%), steroid use (2.4%; p < 0.001), wound infection (1.0%; p < 0.001), nutritional support (33.2%; p < 0.001), hematologic disorders (6.0%; p < 0.001), childhood malignancy (1.5%; p = 0.031), and an ASA classification greater or equal to 3 (80.6%; p < 0.001).Table 1. Demographics variables and comorbidities in patients undergoing pediatric spinal fusion (N = 32,621)Developmental Delayn = 7,637No Delayn = 24,984pAge12.28 (3.16)13.61 (2.45) < 0.001Sex Female53.1472.91% < 0.001 Male46.8627.09%Race65.54%64.81%0.252White15.14%15.37%Black2.78%3.32%Asian0.55%0.37%American Indian or Alaskan Native0.37%0.23%Native Hawaiian or Pacific Islander15.63%15.90%Unknown65.54%64.81%Admission status Inpatient97.89%97.89%0.519 Outpatient2.11%2.11%Surgical approach Anterior2.15%2.85% < 0.001 Posterior97.85%97.15%ScoliosisCongenital/Structural6.77%6.66%< 0.001Idiopathic16.57%78.69%Unable to classify1.34%1.32%Kyphosis4.79%4.48%Neuromuscular62.34%6.42%Syndromic8.19%2.41%Ventilator dependence7.95%0.86%< 0.001Asthma16.62%5.23%< 0.001Chronic lung disease16.34%1.86%< 0.001Oxygen support6.53%0.37% < 0.001Tracheostomy6.81%0.44% < 0.001Esophageal, Gastric, or intestinal disease30.2%3.55%< 0.001History of cardiac Surgery9.86%2.39% < 0.001Cardiac risk factors Severe cardiac risk factors0.90%0.34% < 0.001 Major cardiac risk factors9.31%2.69% Minor cardiac risk factors11.18%3.11% No cardiac risk factors78.60%93.85%Pulmonary Abnormalities20.81%2.62% < 0.001Seizure40.85%1.38% < 0.001Cerebral palsy38.47%1.14% < 0.001Structural CNS abnormalities37.37%6.4% < 0.001Neuromuscular Disorder63.69%8.12%< 0.001Intraventricular Hemorrhage3.26%0.16% < 0.001Steroid use2.37%0.55% < 0.001ostomy40.41%1.77% < 0.001Wound infection0.98%0.16% < 0.001Nutritional support33.17%1.07% < 0.001Sepsis prior to surgery0.92%0.51% < 0.001Hematologic disorders6.06%1.84%< 0.001Inotropic support at Time of surgery0.52%0.49%0.804CPR within 7 days of Surgery0.08%0.02%0.018Transfusions0.33%0.14% < 0.001Childhood malignancy1.49%0.97% < 0.001ASA ClassI: No disturbance1.00%21.01% < 0.001II: Mild disturbance18.16%60.15%III: Severe disturbance73.10%17.72%IV: Life threatening7.45%0.94%V: Moribund0.03%0.00%Work RVU (mean)33.6432.34**< 0.001**Laparoscopic/Minimally Invasive surgery1.55%1.69%0.417Type of fusion Primary84.46%92.30% < 0.001 Revision15.54%7.70% Operative time (minutes)315.56 (119.21)277.78 (102.47) < 0.001ASA American society of anesthesiologists, RVU Relative value units
Developmental delay and pediatric spinal fusion procedure characteristics
Overall, patients with developmental delay experienced longer operative times (315.6 min vs 277.8 min; p < 0.001) and a higher prevalence of procedures using a posterior surgical approach (97.9% vs 97.2%; p < 0.001) (Table 1). Patients without developmental delay had a higher prevalence of patients classified as neuromuscular scoliosis (62.3% vs 6.4%) compared to patients with no developmental delay who had a greater proportion of scoliosis classified as idiopathic (78.7% vs 16.6%; p < 0.001). Patients with developmental delay had a higher intraoperative use of antifibrinolytic (89.7% vs 88.0%; p < 0.001) and postoperative ICU stay (6.2% vs 1.6%; p < 0.001) (Table 3) while patients with no developmental delay had a higher proportion of patients who had a pre-operative MRI for spinal fusion (38.4% vs 25.0%; p < 0.001) (Table 2).Table 2. Univariate analysis of pediatric spinal fusion characteristics by developmental delay cohortDevelopmental Delayn = 7,637No Delayn = 24,984pPre-operative MRI for spinal fusion24.97%38.42% < 0.001Intensive care unit stay6.22%1.64% < 0.001Intraoperative use of neuromonitoring93.57%96.89% < 0.001Intraoperative use of antibiotics84.92%81.54%< 0.001Intraoperative use of antifibrinolytics89.69%87.98% < 0.001Postoperative neurological deficit1.11%1.3%0.218Values are bolded for p < 0.05
Postoperative complications and multivariate analyses
Patients with developmental delay had a higher rate of having the occurrence of one or more surgical complications or medical complications (5.4% vs 1.4%; p < 0.001) compared to patients with no developmental delay. The prevalence of post-operative pneumonia (3.3% vs 0.3%; p < 0.001), reoperation (21.4% vs 7.2%; p < 0.001), and extended length of stay (6.2% vs 1.6%; p < 0.001) was greater in cohort with developmental delay (Table 3). Multivariate logistic regression was performed to determine the differential effect of developmental delay compared to the no developmental delay group on medical complications, surgical complications, ICU stay, extended length of stay, and death while adjusting for the greater comorbidity burden (Table 4). Patients with developmental delay were found to have an increased risk of (OR: 1.099, 95% CI (1.009–1.978), surgical complications (OR: 1.4833, 95% CI (1.197–1.838), extended hospital LOS (OR: 1.250, 95% CI (1.028–1.518), intensive care unit stay (OR: 1.333, 95% CI (1.227–1.446), and death (OR: 9.638, 95% CI 2.150–68.700).Table 3. Univariate analysis of thirty-day post-operative complications after pediatric spinal fusion by cohortDevelopmental Delay n = 7,637No Delayn = 24,984pDeath0.32%0.01% < 0.001surgical complications5.38%1.41% < 0.001Superficial incisional surgical site infection1.78%0.62% < 0.001Deep incisional surgical site infection2.11%0.41% < 0.001Organ space surgical site infection0.9%0.19%< 0.001Wound disruption1.24%0.35% < 0.001Medical Complications5.38%1.41%< 0.001Pneumonia3.31%0.29%< 0.001Unplanned intubation2.12%0.13%< 0.001Renal insufficiency0.09%0.04%0.104Acute renal failure0.07%0.01%0.011Urinary tract infection (UTI)1.95%0.22% < 0.001Coma > 24 hours0.03%0.00%0.085Stroke or intracranial hemorrhage0.03%0.01%0.728Seizure0.16%0.03%< 0.001Nerve injury0.22%0.37%0.063Cardiac arrest Requiring CPR0.42%0.03% < 0.001Bleeding/transfusions76.08%66.9% < 0.001deep vein Thrombosis0.45%0.07%< 0.001C. diff Colitis0.62%0.06% < 0.001Sepsis2.07%0.21%< 0.001Reoperation21.37%7.18% < 0.001Extended length of hospital stay6.22%1.64%< 0.001Values are bolded for p < 0.05Table 4Multivariate adjusted 30-day pediatric spinal fusion postoperative outcomes between groupsOverall CohortDevelopmental Delay(n = 7,637)pAdjusted Odds Ratio95% CILowerUpperMedical complications1.0991.0091.9780.032surgical Complications1.6191.2302.131** < 0.001extended hospital LOS1.2501.0281.5180.025Intensive care unit stay1.4001.2921.517 < 0.001Death9.6382.15068.7000.007**Values are bolded for p < 0.05^^Relative to No Delay cohort
Discussion
This study represents the first large-scale database study evaluating associations between demographic and comorbidity profiles in patients with developmental delay and post-operative outcomes in patients undergoing pediatric spinal fusion surgery. The most important finding of this study was the finding that developmental delay was an independent predictor for medical complications, surgical complications, extended hospital LOS, ICU stay, and death in pediatric spinal fusion patients. As the available research showing associations between developmental delay and poor health and surgical outcomes grows, it is important to understand how this information affects pediatric spinal fusion outcomes.
Several studies have previously elucidated poor surgical outcomes among pediatric patients with developmental delay [9–11]. Dobek et al. described a population of pediatric femoral shaft fracture patients with and without developmental delay. They found that developmental delay was an independent risk factor for hospital readmission, concluding that individual treatment plans should be created to optimize readmission risk and lower costs for the patient and hospital [11]. Boulos et al. evaluated pediatric patients undergoing open reduction internal fixation for upper and lower extremity fracture as well as those undergoing hardware removal due to hardware complications [10]. They discovered that patients who underwent hardware removal were more likely to suffer from developmental delay. Developmental delay subsequently was defined as a key risk factor for infection-relation removal and subsequent investigation was recommended [10]. Fraser et al. conducted a retrospective analysis of patients with Down syndrome treated with spinal fusion. Their analysis showed that the high prevalence of medical comorbidities suggests that the population with Down Syndrome is medically complex and requires meticulous preoperative and postoperative individualized care [9].
The challenges of treating these patients extend beyond comorbidities seen within the population. Despite investigating psychosocial factors affecting treatment of pediatric patients with developmental delay, our analysis demonstrates the challenge of treatment extends beyond the comorbidities seen in this population [17, 18]. These patients can have difficulty following postoperative care instruction and expressing pain, resulting in increased agitation necessitating additional psychosocial support in their recovery [17, 19]. The importance of psychosocial factors in the care of all pediatric patients has been highlighted by Richard et al. in their investigation of pediatric patients undergoing external fixation, and this can likely be extended to developmental delay patients and the increased complications seen in this population [17]. Additionally, Chun et al. postulated that factors such as ability to communicate, tolerance of postoperative eye drops and examinations, and self-injurious behaviors contributed to the increased association endophthalmitis in their investigation of pediatric cataract surgery complications [20]. These previous investigations in addition to our multivariate analysis highlight the importance of preoperative and postoperative care needs in this specific population.
Our study also demonstrates that despite undergoing significantly more preoperative preparation and optimization, shown by increased preoperative MRI, ICU stay, intraoperative neuromonitoring, and antifibrinolytic usage, patients with developmental delay still experienced more surgical complications when controlling for demographic differences. This finding emphasizes the need for preoperative discussions with patients and risk assessment. This population also requires in-depth behavioral and stress-reduction strategies to facilitate all stages of the perioperative experience. Patients with developmental delay can have difficulties with communication and social interaction which can make the preoperative and perioperative environment difficult [21]. Understanding these factors will help optimize care for pediatric patients with developmental delay receiving spinal fusion.
This study has several limitations. The retrospective design and use of the ACS-NSQIP database limits our ability to randomize our patient population and control specific variables, such as variations in postoperative intensive care unit stay protocols. Additionally, developmental delay is a predetermined variable available within the database. The variable is captured by certified clinical reviewers. Although ACS-NSQIP database collects data on a wide array of predetermined factors, it does not include patient-reported outcomes or radiological results. Furthermore, the database only captures information up to thirty days after surgery. This limits our capacity to assess the long-term outcomes, such as fusion data, and may result in the exclusion of unreported complications (e.g. pseudoarthrosis and hardware failure) and functional outcomes beyond the thirty-day period. Evaluating these complications is crucial for assessing the overall efficacy and potential risks associated with pediatric spine surgery. Although the database captures a wide variety of complications; a reduced number of occurrences may contribute to large confidence intervals [22]. Additionally, the study design does not allow us to establish a causal relationship between developmental delay and postoperative complications. Despite these limitations, we were able to find an association between developmental delay in pediatric spinal fusion patients and increased chances of surgical complications and ICU stay. This information can aid surgeons in identifying patients in need of not only medical optimization, but more personalized care due to differences in communication in this population.
In conclusion, patients with developmental delay undergoing pediatric spinal fusion had an increased risk for surgical complications. The findings of this study serve as a valuable resource in aiding surgeons in preoperative risk assessment and in facilitating comprehensive discussions with patients and their caregivers. Given the heterogenous nature presentation of developmental delay within the pediatric population, personalized postoperative management, guided by risk assessment, may help mitigate postoperative complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Scoliosis. AANS. Published April 30, 2024. https://www.aans.org/patients/conditions-treatments/scoliosis/#:~:text=Scoliosis%20affects%202%2D 3%20percent.