Undocumented UroLume Stent Presenting Years Later With Acute Urinary Retention and Infection in a Patient With Dementia
Omar Demachkie, Evan Ehsan, Andres Saucedo, Dulcinea D Jones, Sivarama K Kotikalapudi

TL;DR
An elderly patient with dementia had severe urinary issues caused by an undocumented stent and implant, showing the need for thorough medical evaluations.
Contribution
Highlights the clinical significance of undocumented implants in elderly patients with altered mental status.
Findings
A retained UroLume stent and undocumented AUS caused acute urinary retention and infection.
Lack of documentation significantly delayed diagnosis and treatment.
Elderly patients with dementia require meticulous clinical evaluation for hidden medical devices.
Abstract
An 87-year-old male with dementia was admitted to the behavioral health unit for behavioral disturbances, including increased confusion, agitation - especially when taking medications - daytime somnolence with nighttime wakefulness, and disorientation. He rapidly deteriorated, becoming nonverbal and unresponsive to questions, due to urinary retention and infection caused by a retained UroLume stent placed approximately 30 years earlier. Despite stable vitals and a normal white blood cell count just days prior, his WBC acutely rose to 27,000 cells/mm3, prompting urgent urological intervention. The evaluation also revealed an undocumented artificial urinary sphincter (AUS), which further contributed to urinary retention and complicated management. This case emphasizes the importance of thorough history-taking, physical exams, and awareness of outdated implants, as the absence of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1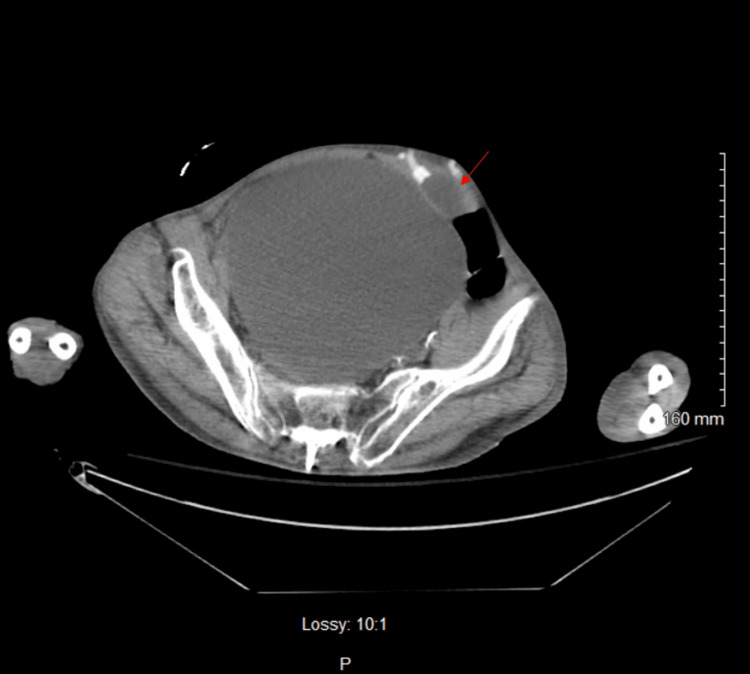 Figure 2
Figure 2 Figure 3
Figure 3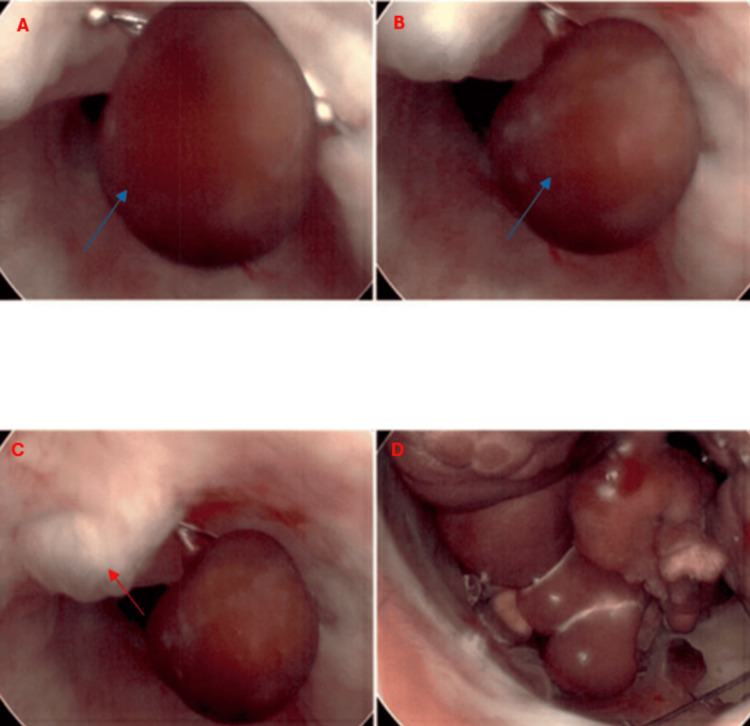 Figure 4
Figure 4| Parameter | February 24, 2025 | February 23, 2025 | February 22, 2025 | Reference range |
| Complete blood count | ||||
| White blood cells (WBC) | 9.20 | 13.90 (H) | 27.50 (H) | 4.0-11.0 x 10^9/L |
| Red blood cells (RBC) | 3.90 | 4.22 | 4.65 | 4.2-5.4 x 10^12/L |
| Hemoglobin (Hgb) | 11.3 (L) | 12.0 | 13.7 | 13.5-17.5 g/dL |
| Hematocrit (HCT) | 35.2 (L) | 38.1 | 41.6 | 40-50% |
| Mean corpuscular hemoglobin (MCH) | 28.9 | 28.4 | 29.5 | 27-31 pg/cell |
| Mean corpuscular hemoglobin concentration (MCHC) | 32.1 (L) | 31.5 (L) | 33.1 | 32-36 g/dL |
| Mean corpuscular volume (MCV) | 90.1 | 90.1 | 89.4 | 80-100 fL |
| Platelet count | 239 | 252 | 317 | 150-450 x 10^9/L |
| Mean platelet volume (MPV) | 8.5 | 8.1 | 8.4 | 7.5-11.5 fL |
| Red cell distribution width (RDW) | 14.1 | 13.9 | 13.6 | 11.5-14.5% |
| Differential | ||||
| Neutrophils (%) auto | 76.2 (H) | 88.4 (H) | 96.2 (H) | 40-70% |
| Lymphocytes (%) auto | 14.0 | 5.5 (L) | 1.1 (L) | 20-40% |
| Monocytes (%) auto | 7.5 | 5.4 | 2.4 (L) | 2-8% |
| Basophils (%) auto | 0.8 | 0.2 | 0.3 | 0-1% |
| Eosinophils (%) auto | 1.5 | 0.5 | 0.0 | 0-5% |
| Neutrophils (#) auto | 7.0 | 12.3 (H) | 26.5 (H) | 2.0-7.5 x 10^9/L |
| Lymphocytes (#) auto | 1.3 | 0.8 | 0.3 (L) | 1.0-3.0 x 10^9/L |
| Monocytes (#) auto | 0.7 | 0.7 | 0.6 | 0.1-0.8 x 10^9/L |
| Basophils (#) auto | 0.1 | 0.0 | 0.1 | 0.0-0.1 x 10^9/L |
| Eosinophils (#) auto | 0.1 | 0.1 | 0.0 | 0.0-0.5 x 10^9/L |
| General chemistry | ||||
| Blood urea nitrogen | 32 | 32 | 34 | 7-20 mg/dL |
| Creatinine | 1.02 | 1.57 | 2.17 | 0.6-1.2 mg/dL |
| Estimated glomerular filtration rate (eGFR) | 71 | 42 | 29 | >60 mL/min/1.73 m² |
| Blood urea nitrogen (BUN)/creatinine ratio | 31.4 | 20.4 | 15.7 | 10-20 |
| Parameter | Value | Normal range |
| UA macroscopic | ||
| Ur color | Red | Yellow |
| Ur appearance | Cloudy | Clear to pale yellow |
| Ur specific gravity | 1.010 | ≤1.005 |
| Ur pH | 6.5 | 5-7.5 |
| Ur protein | 30 | Negative |
| Ur glucose | Negative | Negative |
| Ur ketone | Negative | Normal: negative |
| Ur nitrite | Negative | Normal: negative |
| Ur urobilinogen | 0.2 | Normal: 0.2 |
| Ur leukocyte esterase | Trace | Negative |
| Ur collection source | Random | |
| UA microscopic | ||
| Ur WBC | 0-5 | Negative |
| Ur RBC | TNTC | Negative |
| Ur bacteria | Few | Negative |
| Ur epithelial cells | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPediatric Urology and Nephrology Studies · Kidney Stones and Urolithiasis Treatments · Ureteral procedures and complications
Introduction
Acute urinary retention (AUR) in elderly patients with dementia is often attributed to benign prostatic hyperplasia (BPH), medications such as anticholinergics and opioids [1], or neurological disorders like Parkinson’s disease, where dysfunction of the autonomic nervous system affects the normal control of bladder function [2]. Mechanical obstruction due to encrustation can occur with UroLume stents, as observed in this case. Urinary retention occurs postoperatively in 8-32% of patients who undergo artificial urinary sphincter (AUS) implantation, but it typically occurs early [3]. To the best of our knowledge, there have been no reports of this complication presenting so long after implantation. However, common causes of urinary obstruction, such as BPH and urolithiasis, are more frequently encountered in clinical practice. We present the case of an 87-year-old male whose symptoms, including increased confusion, agitation, daytime somnolence with nighttime wakefulness, and disorientation, were initially mistaken for dementia progression. However, upon further evaluation, including a bladder scan, imaging, and failed catheterization attempts, the true cause was revealed to be a retained UroLume stent and multiple bladder stones.
Case presentation
An 87-year-old male with a history of coronary artery disease (CAD), hypertension (HTN), post-traumatic stress disorder (PTSD), and dementia on hospice was admitted to the behavioral health unit for worsening confusion, agitation, and restlessness. His dementia, which developed after a past brain hemorrhage and subsequent surgery, had progressively worsened, though he had been managed at home until recently. At home, he had become increasingly disoriented, exhibited sleep disturbances, and resisted taking medications.
Three days before admission, recent laboratory results, including a complete blood count (CBC), were unremarkable with a normal white blood cell (WBC) count of 6.7 × 10^3^ cells/mm^3^. Upon arrival, the patient was alert but combative, with a 3/6 holosystolic murmur and a firm, non-reducible mass in the left lower quadrant. The patient attributed the mass to a recent hernia repair surgery. However, within 48 hours of admission, his clinical picture deteriorated. He became minimally responsive to verbal commands and hypertensive (198/91 mmHg) and developed leukocytosis (Table 1). The differential diagnosis was expanded beyond psychological conditions. Urinalysis (UA) revealed red-colored, cloudy urine with a specific gravity of 1.010, proteinuria (30 mg/dL), trace leukocyte esterase, numerous red blood cells (too numerous to count (TNTC)), and few bacteria (Table 2). Physical examination at this point revealed suprapubic distension with a firm and spastic bladder. While these findings can suggest a urinary tract infection, in this case, they were more concerning for obstructive uropathy causing near-complete urinary retention and potential kidney injury rather than a primary infection. A bladder scan showed over 800 mL of retained urine. Attempts at Foley catheter placement with 14- and 16-French (Fr) catheters were unsuccessful. A computed tomography (CT) scan of the abdomen and pelvis revealed bilateral hydronephrosis (Figure 1), bladder distention (Figure 2), an enlarged prostate with multiple brachytherapy seeds, and a history of transurethral resection of the prostate (TURP), as well as an internal bladder-urethral sphincter (Figure 3), which was later determined to be an AUS by the urologist. Additionally, mild bilateral patchy basilar posterior airspace infiltrates consistent with pneumonia were noted.
Axial non-contrast CT image at the renal levelMild-to-moderate bilateral hydroureteronephrosis, with red arrows pointing to both sides.
Axial non-contrast CT image at the bladder levelThe bladder is obstructed and distended, measuring 18 cm, with no apparent gross thickening of the bladder wall; a red arrow points to the abdominal balloon reservoir of the artificial urethral sphincter.
Axial non-contrast CT image at the prostate and penile regionThe prostate appears enlarged with multiple brachytherapy seeds and prior transurethral resection of the prostate (TURP). The red arrow points to the internal bladder-urethral sphincter.
A urologist was consulted after failed catheterization attempts and concern for urinary obstruction. During evaluation, an AUS was identified. Believing that previous failures may have resulted from an inflated AUS cuff, the urologist deflated the device and attempted catheterization with 10-, 12-, and 14-Fr catheters, but all attempts were unsuccessful. Given the persistent obstruction, a cystoscopy was performed, which disclosed significant obstruction of the prostatic urethra caused by a heavily encrusted UroLume stent that had been implanted decades earlier. The stent exhibited extensive encrustation, characterized by the accumulation of mineral deposits - likely calcium or other urinary salts - on its surface. This encrustation manifested as irregular, rough, and whitish deposits, giving the stent a markedly uneven and less smooth texture. The severe calcification of the stent ultimately impeded the advancement of the cystoscope into the bladder, preventing further visualization. Additionally, multiple large bladder stones were identified, further contributing to the obstruction (Figure 4). However, the stones could not be removed because they were corroded and fused to the bladder wall. Given the findings, a suprapubic catheter was placed using a trocar-assisted technique. The procedure was well tolerated, and the patient was transitioned to floor care for further management following cystoscopy and treatment of pneumonia.
Cystoscopy Large bladder stones are seen in panels A and B (e.g., blue arrow), alongside an encrusted and heavily calcified UroLume stent in panel C (red arrow). Multiple large bladder stones are also visible in panel D.
The following day, the patient's blood pressure stabilized at 122/68, and his WBC count decreased to 13.9 (Table 1), likely due to the drainage from the catheter. He was also able to eat and communicate properly, which had been initially impaired. Despite not removing the stones, the patient's symptoms significantly improved, and his overall condition showed marked improvement, including the above findings as well as the absence of agitation, a calm demeanor, and a willingness to take his medication. Additionally, the urine culture collected post-catheterization showed no bacterial growth at two days.
Discussion
This case emphasizes the importance of vigilant observation and thorough physical exams in elderly dementia patients. In patients with dementia, new or altered symptoms, such as confusion and agitation, can often be mistakenly attributed solely to the progression of cognitive decline. However, it is crucial to recognize that these symptoms may reflect underlying physical issues that are not immediately apparent, even despite unremarkable labs and vital signs. Dementia can mask acute illnesses, increasing the risk of misdiagnosis and delayed care. According to a report by the Agency for Healthcare Research and Quality (AHRQ), over 10% of both overdiagnosis and underdiagnosis occur in conditions like dementia, chronic obstructive pulmonary disease (COPD), Parkinson’s, heart failure, stroke, and myocardial infarction [4]. Additionally, 26% of hospitalized patients with pre-existing dementia lacked proper documentation of their diagnosis, potentially leading to mismanagement [5].
Urinary obstruction is one such condition that can be easily overlooked, particularly when initial UA findings are misinterpreted. It is absolutely possible to observe hematuria (red blood cells TNTC), proteinuria, trace leukocyte esterase, and cloudy, red urine in the setting of obstruction without active infection. Obstruction, especially prolonged, can lead to bladder wall irritation, pressure-induced renal tubular damage, or even microhemorrhage, all of which can mimic or overlap with typical infectious UA patterns. These findings must be carefully correlated with clinical context, particularly in patients unable to articulate symptoms, such as those with dementia.
Despite initially stable vitals and a normal white blood count, the patient rapidly developed AUR, severe leukocytosis, and HTN. The presence of normal labs and stable vital signs - paired with the patient’s cognitive decline - initially led to the misattribution of his symptoms to dementia progression. However, this abrupt clinical deterioration highlights the importance of frequent reassessment rather than relying solely on initial laboratory results. Urethral obstruction can progress quickly, leading to life-threatening complications if not promptly diagnosed.
This case is particularly notable due to the presence of a UroLume stent, a once-common implant for bladder outlet obstruction that was largely abandoned due to complications like encrustation and obstruction. Developed in the 1980s, the UroLume is a permanent, self-expanding metallic stent designed to maintain urethral patency in patients with urinary obstruction. Once deployed, it expands to approximately 30 Fr in diameter and is delivered using a 24 Fr system for ease of placement during endoscopic procedures [6]. Initially recommended for men who were not candidates for major surgery but still required urethral patency, it was also used in cases of radiation-induced strictures [7]. However, studies reported high complication rates, including hematuria, chronic pain, infections, and stone formation, often necessitating removal. One study found a 35% complication rate, including gross hematuria and intermittent clot retention, in patients who received the UroLume stent for BPH [8]. Another study linked permanent urethral stents, such as the UroLume, to encrustation, urinary tract infections, chronic pain, and stone formation, reinforcing the need for their removal [9].
The presence of a long-residing UroLume stent, undocumented in the patient’s recent medical records, suggests that the delayed complications may have arisen in part due to patient-related factors such as poor compliance with follow-up care and memory lapses over the years. These factors likely contributed to the progression of urinary obstruction and the development of associated clinical symptoms in advanced age.
The calcified UroLume stent was left in place due to severe calcifications and adhesions, making its removal risky and potentially harmful, especially considering the patient's advanced age and complex medical history. Similarly, the stones were not removed, as their extraction was deemed too difficult and dangerous, with the risks outweighing the potential benefits. After discussing the patient's condition and options with the family, including the impact on quality of life with or without surgery, the decision was made to insert a suprapubic catheter for symptom management. The patient was then transferred to home hospice care to focus on comfort and quality of life.
A similar case report describes a 24-year-old male who developed malignant HTN and azotemia secondary to bladder outlet obstruction, with significant improvement following transurethral dilation [10]. While the patient in this case report initially did not have azotemia on admission, this may be explained by either the presence of intermittent or partial bladder outlet obstruction or by the patient’s low muscle mass, as was the case here. For example, serum creatinine is influenced by muscle mass; individuals with low muscle mass may produce less creatinine, resulting in deceptively normal values even in the presence of reduced glomerular filtration rate [11]. Therefore, a normal creatinine level does not necessarily exclude kidney dysfunction.
The calcified UroLume stent was left in place due to severe calcifications and adhesions, making its removal risky and potentially harmful, especially considering the patient's advanced age and complex medical history. Similarly, the stones were not removed, as their extraction was deemed too difficult and dangerous, with the risks outweighing the potential benefits. After discussing the patient's condition and options with the family, including the impact on quality of life with or without surgery, the decision was made to insert a suprapubic catheter for symptom management. The patient was then transferred to home hospice care to focus on comfort and quality of life.
According to an article by National Health Service England, managing an AUS properly during catheterization is essential to avoid complications. The guidelines stress that the AUS cuff must always be deflated before catheter insertion to prevent tissue damage, trauma, or infection. If this step is not performed, serious harm can occur [12]. Identifying an AUS during a physical exam can be difficult because of its internal placement. Typically, the device includes a cuff around the urethra, a control pump in the scrotum, and a pressure-regulating balloon in the abdomen. Palpation of the scrotum may reveal the pump, which can aid in recognizing the presence of an AUS. However, imaging studies such as CT or MRI are more effective in visualizing the entire device and assessing its condition [13]. The study by Capra and Chou (2018) on the cross-sectional appearance of common implants revealed the following features: 1) the urethral cuff appears as a circumferential structure surrounding the urethra; 2) the scrotal pump is visible within the scrotum, identifiable by its characteristic shape and location; and 3) the abdominal balloon reservoir is located in the abdomen, typically near the bladder, and is distinguishable based on its size and configuration.
The current recommendation from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) for obtaining a CT scan in cases of urinary retention is when symptoms remain unresolved or are severe, particularly if initial evaluations (e.g., bladder scan or ultrasound) do not clarify the cause. A CT scan is also recommended if the physician suspects that the retention is due to an obstruction or in cases involving sepsis, hematuria, or recurrent urinary tract infections [14].
AUR is a urologic emergency that requires immediate intervention. This intervention should occur as soon as retention is clinically suspected or confirmed via ultrasound [15]. For patients with a history of urethral stricture, injury, bladder or urethral surgery, or pelvic/perineal trauma that may have altered urethral anatomy, it is advisable to urgently refer them for urologic evaluation rather than attempting standard catheterization. These individuals may require alternative approaches, such as using a coudé-tip catheter, endoscopic catheter placement via cystoscopy, or suprapubic catheterization, to ensure safe and effective management [16].
The decision to escalate care to cystoscopy and suprapubic catheterization was critical in preventing further complications such as renal failure or septic shock. A study suggests that integrating bedside retrograde urethrogram and retrograde urethroscopy can help identify urethral pathology, allowing for dilatation and per urethral catheterization, thus avoiding suprapubic catheter placement [17].
Conclusions
This case reinforces the importance of maintaining a high index of suspicion for urinary obstruction in elderly patients with altered mental status. Clinicians should always consider past urological interventions, even if undocumented, and act promptly to prevent severe complications. Ultimately, early urological intervention, including cystoscopy and suprapubic catheter placement, played a crucial role in stabilizing this patient and preventing further complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1What do we know about opioids and the kidney?Int J Mol Sci Mallappallil M Sabu J Friedman EA Salifu M 2231820172811775410.3390/ijms 18010223 PMC 5297852 · doi ↗ · pubmed ↗
- 2Treatment options for urogenital dysfunction in Parkinson’s disease Curr Treat Options Neurol Batla A Tayim N Pakzad M Panicker JN 451820162767944810.1007/s 11940-016-0427-0PMC 5039223 · doi ↗ · pubmed ↗
- 3Transcorporal artificial urinary sphincter cuff placement is associated with a higher risk of postoperative urinary retention Can J Urol Smith PJ Hudak SJ Scott JF Zhao LC Morey AF 67736777202013 https://pubmed.ncbi.nlm.nih.gov/23783046/23783046 · pubmed ↗
- 4Unique challenges in approaching diagnostic safety in older adults 2024 https://www.ahrq.gov/diagnostic-safety/resources/issue-briefs/dxsafety-older-adults 2.html
- 5How well are the diagnosis and symptoms of dementia recorded in older patients admitted to hospital?Age Ageing Crowther GJ Bennett MI Holmes JD 1121184620172818165410.1093/ageing/afw 169 · doi ↗ · pubmed ↗
- 6Preservation of lower urinary tract function in posterior urethral stenosis: selection of appropriate patients for urethral stents J Urol Eisenberg ML Elliott SP Mc Aninch JW 2456246017820071793796210.1016/j.juro.2007.08.013 · doi ↗ · pubmed ↗
- 7Management for prostate cancer treatment related posterior urethral and bladder neck stenosis with stents J Urol Erickson BA Mc Aninch JW Eisenberg ML Washington SL Breyer BN 19820318520112107479610.1016/j.juro.2010.09.020PMC 3557853 · doi ↗ · pubmed ↗
- 8Long term results with the Urolume urethral stent: single surgeon experience over 11 years.: 572J Urol Haraway AM Secrest CL 2041812009 https://journals.lww.com/auajuro/citation/2009/04001/long_term_results_with_the_urolume_urethral_stent_.572.aspx