Endoscopic intermuscular dissection for a duodenal neuroendocrine tumor using saline-immersion therapeutic endoscopy
Priscilla Lopez, Mohan Ramchandani, Sundeep Lakhtakia, Pradev Inavolu, Hardik Rughwani, Anjan Kaipa, D. Nageshwar Reddy

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1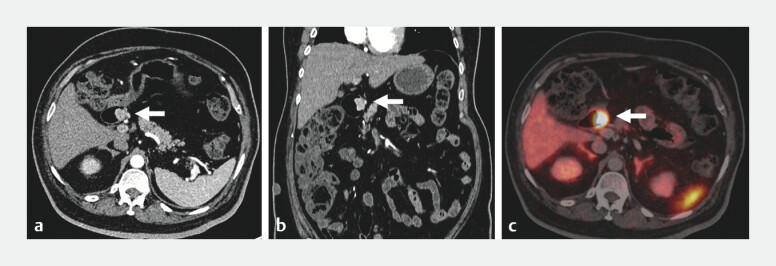 Fig. 2
Fig. 2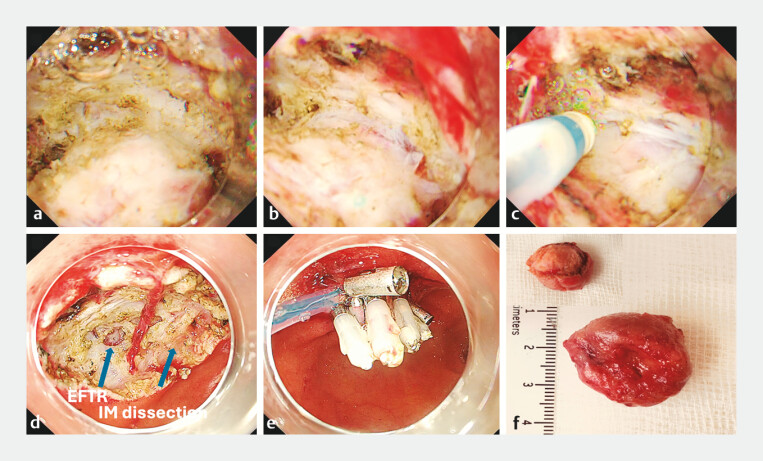 Fig. 3
Fig. 3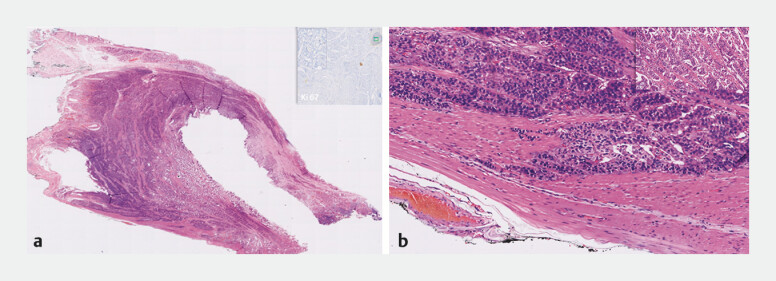 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Gastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment
A 68-year-old man with type 2 diabetes and hypertension underwent upper gastrointestinal endoscopy for anemia, revealing an ulcerated subepithelial lesion on the anterior-superior wall of the duodenal bulb ( Fig. 1 a ). Endoscopic ultrasound revealed a 25-mm hypoechoic lesion arising from the submucosa and extending into the muscularis propria, with increased vascularity ( Fig. 1 b, c ).
Initial investigations. a Ulcerated subepithelial lesion in the duodenal bulb (D1). b Endoscopic ultrasound showing a 25-mm hypoechoic lesion arising from the submucosa and extending into the muscularis propria. c Endoscopic ultrasound with Doppler demonstrating increased vascularity within the lesion.
Computed tomography (CT) and positron emission tomography-CT confirmed a localized lesion without nodal or distant spread ( Fig. 2 ). Based on these features, endoscopic full-thickness resection (EFTR) was planned.
Computed tomography (CT) imaging. a–c Ga-68 DOTA-TOC positron emission tomography with CT showing a tracer-avid (maximum standardized uptake value: 178.3), well-defined, intensely arterially enhancing polypoidal soft tissue lesion (arrow) in the duodenum (D1) along the medial aspect.
The procedure was performed under general anesthesia. Initial dissection with conventional EFTR using carbon dioxide insufflation was limited by poor maneuverability, presence of fibrosis, and bleeding. The approach was converted to saline-immersion therapeutic endoscopy (SITE). Swift Coagulation (effect 3.5) was used to safely coagulate vessels without a coagulation grasper, minimizing the risk of perforation.
An intermuscular dissection technique was employed to target the space between the inner and outer muscularis propria, avoiding EFTR when possible. Only a <6-mm area required EFTR due to deep invasion. This approach minimized peritoneal exposure and avoided pneumoperitoneum ( Fig. 3 , Video 1 ). The resection site was closed using the loop-and-clip technique. No complications occurred.
Endoscopy images. a–c Endoscopic intermuscular dissection using saline-immersion therapeutic endoscopy, showing the space between the inner and outer muscularis propria. d Resection site demonstrating predominant intermuscular dissection with a small area (<6 mm) of endoscopic full-thickness resection where the lesion extended into the muscularis propria (arrows). e Defect closed using the loop-and-clip technique. f Resected tumor.
Saline immersion and intermuscular dissection enabled safe resection of a duodenal neuroendocrine tumor involving the muscularis propria, minimizing full-thickness resection and preventing procedural complications.Video 1
Histology confirmed a well-differentiated neuroendocrine tumor, infiltrating the muscularis propria, with negative lateral and vertical margins and no lymphovascular invasion ( Fig. 4 ).
Histology. a Well-differentiated (G1) neuroendocrine tumor with Ki-67 index <2%. b Negative resection margins; inset demonstrates tumor cell infiltration into the muscularis propria.
Endoscopic resection of duodenal lesions involving the muscularis propria is challenging due to the thin wall, narrow lumen, and proximity to important vessels 1 . While EFTR offers an alternative to surgery, it carries risks such as pneumoperitoneum and bleeding 2 .
This video demonstrates a combined approach using the advantages of SITE-enhanced visualization, elimination of gas insufflation, buoyancy-assisted traction, and reduced thermal injury through gradual coagulation enabled by improved conductivity 3 4 (“frozen tree” effect). Furthermore, intermuscular dissection 5 enabled a targeted approach, limiting EFTR to only the extent necessary for complete tumor removal, highlighting its value in anatomically challenging cases.
Endoscopy_UCTN_Code_TTT_1AO_2AC
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gaspar JP Stelow EB Wang AY Approach to the endoscopic resection of duodenal lesions World J Gastroenterol 20162260061710.3748/wjg.v 22.i 2.60026811610 PMC 4716062 · doi ↗ · pubmed ↗
- 2Jian G Tan L Wang H Factors that predict the technical difficulty during endoscopic full-thickness resection of a gastric submucosal tumor Rev Esp Enferm Dig 2021113354033207904 10.17235/reed.2020.7040/2020 · doi ↗ · pubmed ↗
- 3Capogreco A Maselli R Enderle M Different behavior of electrosurgical currents between air and saline immersion therapeutic endoscopy Sci Rep 202515438839910260 10.1038/s 41598-024-83503-3PMC 11799136 · doi ↗ · pubmed ↗
- 4Despott EJ Murino A Saline-immersion therapeutic endoscopy (SITE): an evolution of underwater endoscopic lesion resection Dig Liver Dis 201749137610.1016/j.dld.2017.08.03528967632 · doi ↗ · pubmed ↗
- 5Moons LMG Bastiaansen BAJ Richir MC Endoscopic intermuscular dissection for deep submucosal invasive cancer in the rectum: a new endoscopic approach Endoscopy 20225499399810.1055/a-1748-857335073588 · doi ↗ · pubmed ↗