Endoscopic closure of a congenital tracheo-esophageal fistula using a through-the-scope suturing device in a young boy
Mark Ellrichmann, Gennadii Ivanov, Ina D. Ellrichmann, Mareike Mumm, Andreas Meinzer, Claudio C. Conrad, Robert Bergholz

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
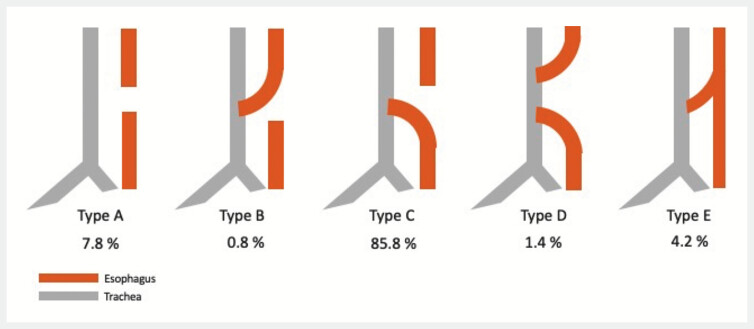 Fig. 1
Fig. 1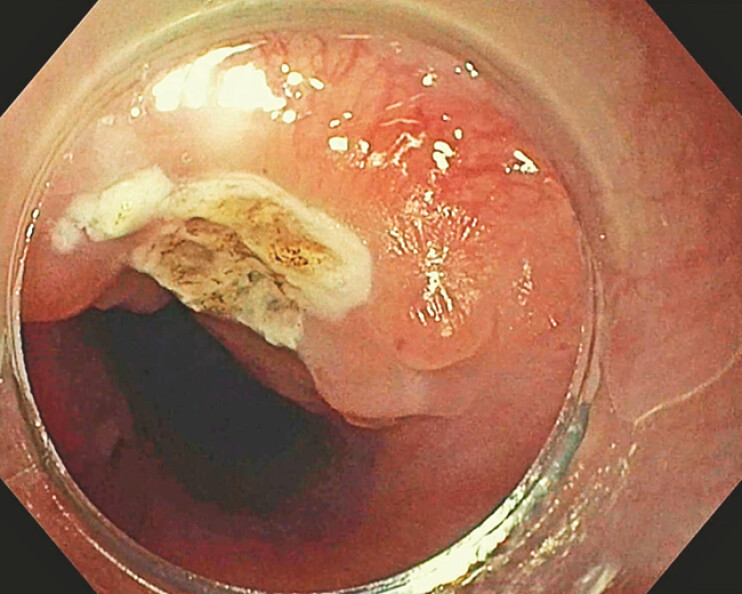 Fig. 2
Fig. 2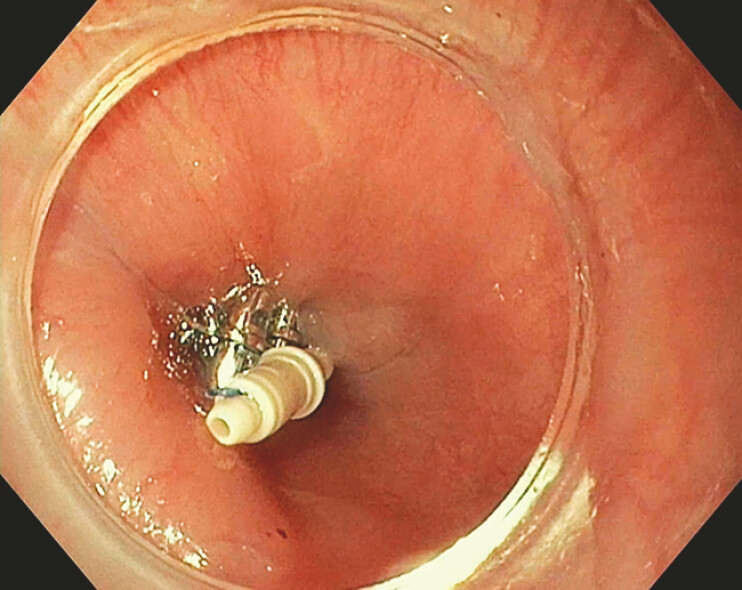 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Tracheal and airway disorders · Foreign Body Medical Cases
Tracheoesophageal fistulas (TEF) are a congenital anomaly with an incidence of approximately 1 in 4,000 births. TEF are classified into types A–E, with type E being the most amenable to endoscopic closure ( Fig. 1 ) 1 . Advances in endoscopic techniques have expanded the therapeutic options for managing TEF. Here, we present a case of successful endoscopic closure of a TEF using a novel through-the-scope suturing device (TTS-SD, X-Tack, Boston Scientific) 2 . A 37-month-old boy presented with postprandial coughing and recurrent bronchopulmonary infections. Initial endoscopy revealed a small, non-functional porus without significant TEF. Six months later, the patient’s condition worsened with the diagnosis of a significant type E TEF, located 13 cm from the dental arch. An attempt of clip closure failed after 2 weeks. A fully covered self-expanding metal stent (fcSEMS, 10 × 80mm) was then placed but dislocated within days, another fcSEMS (20 × 80mm) was removed after 1 day due to thoracic pain. Given the narrow esophageal diameter, over-the-scope clips and overstitch devices were not feasible. The novel TTS-SD was employed instead. The fistula was debrided with argon plasma coagulation and brushing ( Fig. 2 ). Four helices were placed 4 mm from the fistula margin in a Z-shaped configuration and secured with a closure plug. Air insufflation confirmed successful closure ( Fig. 3 ). At 2 weeks, the helices were partially detached but the patient was asymptomatic. By six weeks, the helices had fully detached, with no symptoms. At 6 months, follow-up confirmed stable closure without recurrence ( Video 1 ). Endoscopic closure of Type E tracheoesophageal fistula presents a minimally invasive alternative to surgery 3 . The TTS-SD significantly expands the endoscopic therapeutic armamentarium, especially in narrow spaces or distorted anatomy. This case demonstrates the successful closure of a congenital H-fistula with endoscopic techniques, suggesting that endoscopy could be the method of choice for treating Type E fistulas.
Schematic overview of different categories of tracheo-esophageal fistula Type A–E with respective distribution of occurrence of the subtypes (%), own picture based on McGowan et al. 2022 1 .
Argonplasma coagulation of tracheo-esophageal fistula Type E.
Successful endoscopic suturing of tracheo-esophageal fistula Type E with helices and locking plug in place.
Endoscopic closure of a congenital tracheo-esophageal fistula using a through-the-scope suturing device in a young boy.Video 1
Endoscopy_UCTN_Code_TTT_1AO_2AI
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Gowan NA Grosel J An overview of esophageal atresia and tracheoesophageal fistula JAAPA 202235343710.1097/01.JAA.0000830180.79745.b 935617475 · doi ↗ · pubmed ↗
- 2Gong R Wang S Song J Closure methods for large defects after gastrointestinal endoscopic submucosal dissection J Gastroenterol Hepatol 202410.1111/jgh.16722 PMC 1166021239175260 · doi ↗ · pubmed ↗
- 3Ling Y Sun B Li J Endoscopic interventional therapies for tracheoesophageal fistulas in children: A systematic review Front Pediatr 202311112180310.3389/fped.2023.1121803 PMC 999242536911034 · doi ↗ · pubmed ↗