A shorter pre-vitrification equilibration time for laser-collapsed human blastocysts is associated with a lower miscarriage rate in ART treatments
Romualdo Sciorio, Liuguang Zhang, Yuhu Li, Ning Li

TL;DR
Shortening the equilibration time before freezing blastocysts may reduce miscarriage rates in assisted reproductive treatments.
Contribution
This study shows that a shorter equilibration time (7-8 minutes) is linked to lower miscarriage rates in frozen embryo transfers.
Findings
The miscarriage rate was significantly lower in the 7-8 minute equilibration group (7.6%) compared to the 9-10 minute group (14.2%).
Clinical pregnancy and survival rates were similar between the two equilibration time groups.
Live birth and neonatal outcomes were not significantly different between the groups.
Abstract
Frozen embryo transfer in humans, especially at the blastocyst stage, provides a valid alternative to fresh embryo transfer. However, protocols for blastocyst vitrification are not yet standardized; for example, exposure to the first equilibration solution before vitrification commonly ranges from 2-3 minutes at 37°C or 2-15 minutes at room temperature. This study compared the clinical and neonatal outcomes involving vitrified-warmed blastocysts. The main aim of this prospective study was to compare the clinical and neonatal outcomes for 831 warmed blastocysts, returned in 585 frozen embryo transfers with two exposure times to the equilibration solution at room temperature: (A) 7-8 minutes and (B) 9-10 minutes. The patients’ characteristics were comparable between the two groups with no significant difference in their mean age, the average number of blastocysts transferred, basal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
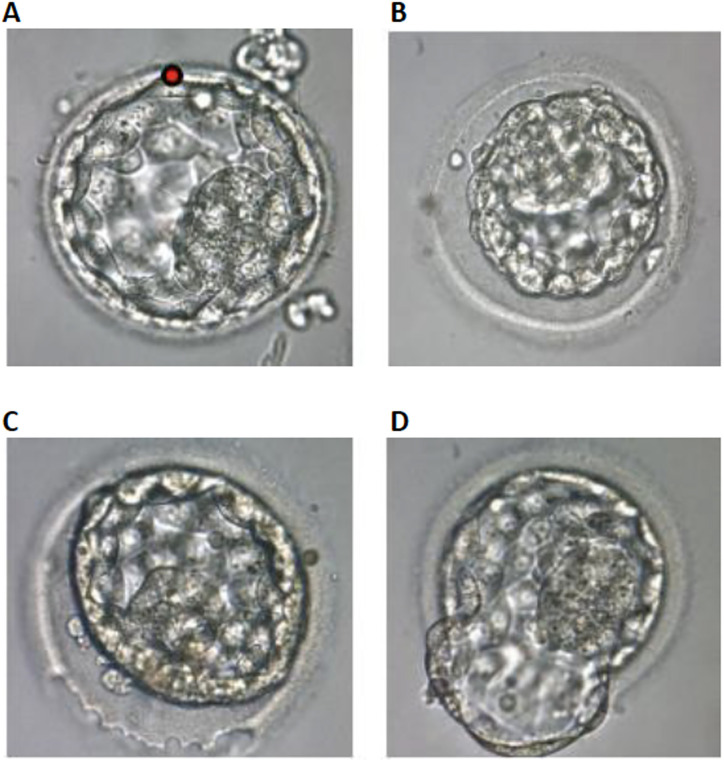 Figure 1
Figure 1| Overall Clinical Outcomes | |
|---|---|
| Blastocyst survival | 99.3% (825/831) |
| Clinical pregnancy | 68.5% (401/585) |
| Live birth | 61.0% (357/585) |
| Miscarriage | 11.0% (44/401) |
| Multiple (twin) gestation | 22.2% (89/401) |
| Group A | Group B | ||
|---|---|---|---|
| FET cycles | 285 | 300 | |
| Maternal age (years) | 30.17±3.48 | 29.50±4.09 | 0.767 |
| Transferred blastocysts (n) | 1.44 ±0.55 | 1.38±0.52 | 0.599 |
| Basal FSH (mIU/mL) | 7.33±1.51 | 7.00±1.79 | 0.734 |
| Maternal BMI | 22.67±2.16 | 21.17±2.14 | 0.254 |
| Infertility duration (years) | 4.17±1.47 | 4.67±1.75 | 0.604 |
| Primary infertility | 65 (26.0%) | 62 (21.5%) | 0.223 |
| Endometrial thickness (mm) | 8.83±1.47 | 9.0±1.10 | 0.828 |
| Artificial cycles | 244 (85.6%) | 240 (80.0%) | 0.073 |
| Natural cycles | 41 (14.4%) | 60 (20.0%) | 0.610 |
| Group A (7-8 minutes) | Group B (9-10 minutes) | p-value | |
|---|---|---|---|
| Survived blastocysts (%) | 99.3 (410/413) | 99.3 (415/418) | 1.000 |
| Clinical pregnancy (%) | 69.1 (197/285) | 68.0 (204/300) | 0.770 |
| Live birth (%) | 63.8 (182/285) | 58.3 (175/300) | 0.171 |
| Miscarriage (%) | 7.6 (15/197) | 14.2 (29/204) | 0.034 |
| Multiple (twin) gestation (%) | 20.8 (41/197) | 23.5 (48/204) | 0.513 |
| Group A | Group B | p-value | |
|---|---|---|---|
| Male babies (%) | 57.1 (104/182) | 55.4 (97/175) | 0.601 |
| Gestational age (weeks) | 38.67±1.37 | 38.33±1.21 | 0.664 |
| Preterm birth (%) | 19.2 (35/182) | 20.6 (36/175) | 0.733 |
| Birth weight (Kg) | 2.95±0.58 | 3.05±0.63 | 0.780 |
| Low birth weight (%) | 17.0 (31/182) | 25.1 (44/175) | 0.052 |
| Macrosomia (%) | 3.3 (6/182) | 2.8 (5/175) | 0.381 |
| Cesarean section (%) | 70.0 (128/182) | 68.5 (120/175) | 0.771 |
| Congenital abnormalities (%) | 0.5 (1/182) | 0 (0/175) | 0.913 |
- —Medical and Health Research Project of Hainan
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive Biology and Fertility · Reproductive Health and Technologies · Assisted Reproductive Technology and Twin Pregnancy
INTRODUCTION
Since the birth of Louise Joy Brown in 1978, assisted reproductive technology (ART) has been constantly increasing, and has permitted millions of infertile couples to conceive (De Geyter et al., 2020). Advancements in ART have been achieved thanks to several improvements, including ovarian stimulation, fertilization, embryo culture procedures and, importantly, to the progress in cryopreservation methods with the application of vitrification (Kuwayama et al., 2005a; 2005b). Indeed, the ability to cryopreserve human embryos has improved significantly in the last decade (Rienzi et al., 2017; Sciorio et al., 2018; Nagy et al., 2020). Since the introduction of minimal volume vitrification protocols, it has become increasingly evident that vitrification is very effective for human blastocysts (Ferreux et al., 2018; Sciorio et al., 2018; 2019). However, it remains important to ascertain whether the methods utilized to cryopreserve human embryos might be improved.
Cryoprotective agents (CPAs) applied during the vitrification process might negatively impact cellular metabolism and function, cell growth and apoptosis (Kollerup Madsen et al., 2018; Smith et al., 2018). Also, a high concentration of CPAs might increase the levels of reactive oxygen species (ROS) and induce epigenetic dysregulation (Zhao et al., 2016; Verheijen et al., 2019; Barberet et al., 2020; Lin et al., 2022; Mao et al., 2022). Several publications reported that human embryos should be kept in the vitrification solution (VS) for a maximum of 1 minute (Loutradi et al., 2008; AbdelHafez et al., 2010; Zhu et al., 2011), while the equilibration times normally ranged from 2 to 15 minutes (Sciorio et al., 2018; 2019; Verheijen et al., 2019; Nagy et al., 2009; 2020).
The exposure time of embryos to CPAs represents an important concern for successful vitrification. Longer exposure to equilibration solution (ES) may be detrimental to further embryo development, while a shorter time may be not enough for the penetration of CPAs into the cells. Contrasting results have been found in the literature, with studies reporting a fixed equilibration time of 5 minutes and others increasing the exposure time up to 15 minutes (Bagis et al., 2005; Hiraoka et al., 2009; Rezazadeh Valojerdi et al., 2009; Selman et al., 2009; Kader et al., 2010; Xie et al., 2010; Shi et al., 2012; Desai et al., 2013). Novel studies have shown that a shorter equilibration time of 8-11 minutes can be sufficient for effective vitrification of human blastocysts (Mitsuhata et al., 2020). Also, a study investigating blastocyst vitrification in the bovine model, by Martínez-Rodero et al. (2021) showed that a shorter equilibration time (3 minutes) during the vitrification procedure resulted in a significantly lower apoptosis rate when compared to a longer equilibration time (12 minutes).
These variations imply that an agreement is still missing regarding the correct equilibration time for human embryo vitrification and, therefore, to improve our vitrification protocol we decided to investigate the effects of two different equilibration times (7-8 versus 9-10 minutes) and to establish any correlation with embryo survival rate, pregnancy and clinical outcomes, and percentage of spontaneous miscarriage.
MATERIALS AND METHODS
This was a prospective study, performed at the Centre for Reproductive Medicine, Haikou Mary Hospital, China from March 2018 to May 2022, and included 585 frozen embryo transfers (FETs). Informed consent for experimentation with human subjects was obtained before the patients started their ovarian stimulation. All participants understood what the study was and what they were consenting to and had the opportunity to opt out at any time. Female age <35 years, and causes of infertility included male factors, female infertility, and unexplained infertility. In this prospective cohort study, all patients undergoing ART treatment with embryos available for vitrification were included in the investigation, excluding only couples undergoing preimplantation genetic assessment and those azoospermic males who had to be treated with surgical sperm retrieval for oocytes injection.
Embryos were produced by either standard IVF insemination or using intracytoplasmic sperm injection (ICSI), according to the sperm assessment previously performed. Following the fresh embryo transfer, ≥2 supernumerary good quality blastocysts, according to Gardner’s score (Gardner & Schoolcraft, 1999) excluding those with a grade of CC, BC, or CB, were vitrified on day 5 after fertilization. The study included 831 expanded blastocysts, which were divided into two groups according to the equilibration time: group (A) 7-8 minutes (n=413) and group (B) 9-10 minutes (n=418). To avoid any skewing of results and to perform blastocyst allocation as equally as possible, we included in the study only those patients who had a minimum of two blastocysts available for vitrification, assigning one blastocyst to group A (7-8 minutes) and the other to group B (9-10 minutes). Exposure time in ES was meticulously controlled by an additional operator, who recorded the exact time of transfer into the vitrification solution. Also, all blastocysts with a Gardner’s expansion grade of ≥3 were artificially collapsed with a laser shot at the minimum setting. Expanding blastocysts contain a considerable amount of fluid, which may be susceptible to formation of ice crystals and increase the risk of cell death. Thus, as described by others, artificial shrinkage (AS) induces a collapse over a short time and converts the blastocyst to a morula-like stage without any fluid-filled cavity, allowing an easy passage of CPAs into the embryo (Mukaida et al., 2006; Taylor et al., 2010; Li et al., 2014; Levi-Setti et al., 2016; Sciorio et al., 2018; 2019).
The primary outcomes of this study were to investigate if different equilibration times might have an impact on live birth rate (LBR) and miscarriage rate. The secondary outcomes included survival rate at warming and the clinical pregnancy rate (CPR).
Ovarian stimulation
In all patients, controlled ovarian stimulation was achieved with either a Gonadotrophin-Releasing Hormone (GnRH) agonist (subcutaneous Buserelin 0.5 ml daily) or GnRH antagonist (subcutaneous Cetrorelix 0.5 mg daily, Merck Serono) treatment. The long protocol was used for downregulation using subcutaneous Buserelin or the GnRH antagonist; Cetrotide was administered daily on day six of the onset of menses. Ovarian stimulation was carried out using either Gonal F (Merck Serono) or Menopur (Ferring) based on individual patient characteristics. Follicular development was monitored by transvaginal ultrasound and ovulation was triggered when three follicles were 18 mm or above. Each patient received human Chorionic Gonadotrophin (hCG; Ovitrelle 0.25 mg, Merck Serono) to trigger ovulation.
Oocyte retrieval and embryo development
Oocyte recovery was carried out under sedation using transvaginal ultrasound guidance at 36 hours following Ovitrelle injection using a 17-gauge single-lumen needle (K-OPS-7035-RWH-ET; Cook Medical Australia) (Sciorio et al., 2019). Cumulus-oocyte-complexes (COC) were isolated from follicular fluid, rinsed, and transferred to 0.6 ml of Universal IVF Medium (CooperSurgical Fertility Solutions, Denmark) covered with oil for tissue culture (CooperSurgical Fertility Solutions, Denmark) in four-well dishes (Nunc™; ThermoFisher Scientific) and returned to the incubator (Astec Co., Ltd, Japan) equilibrated at 37°C, 6% CO_2_, 5%O_2_ and 89% N_2_. All media used were covered with oil and incubated overnight. Semen used for either standard IVF insemination or the ICSI procedure was collected by masturbation and processed using a standard method as reported by Bourne et al. (2004). All oocytes were cultured in Universal IVF Medium on the day of insemination as reported by Zhang et al. (2022).
The technique for insemination (standard IVF or ICSI) was decided according to the semen sample parameters and the histories of the couple. For IVF procedures, oocytes were exposed to 150,000 motile sperm/ml, while ICSI injection was performed 38-42 h post-hCG. Fertilization was identified by the presence of two pronuclei and two polar bodies approximately 16-19 hours post insemination or microinjection. At this stage, normally fertilized oocytes were cultured individually in a 25 µl pre-equilibrated droplet of Quinn’s Advantage Cleavage medium (CooperSurgical Fertility Solutions, Denmark) under oil in a standard incubator (Astec Co., Ltd, Japan) equilibrated at 37°C, 6% CO_2_, 5% O_2_ and 89% N_2_. Dishes were removed from the incubator for morphological assessment approximately 42-44 hours after insemination on day 2.
On the morning of day 3, about 66-68 hours post-insemination, embryos were moved from cleavage medium to a 25 µl droplet of Quinn’s Advantage Blastocyst medium (CooperSurgical Fertility Solutions, Denmark) and were cultured in groups of two or three embryos. On the morning of day 5, the best quality blastocyst, based on Gardner’s score (Gardner & Schoolcraft, 1999) was replaced in a fresh embryo transfer; any remaining good quality blastocysts were cryopreserved. Some patients had no fresh embryo replacement, and all the blastocysts were vitrified for future use. All blastocysts included in the study were cryopreserved on day 5.
Artificial shrinkage of blastocysts
Blastocysts were classified using Gardner’s score according to blastocyst size, the morphology of the inner cell mass (ICM) and trophectoderm (TE) (Gardner & Schoolcraft, 1999). Blastocysts with a score ≥2, excluding those with a grade of CC, BC, or CB, were selected on day 5 for vitrification. Hatching and expanded blastocysts (grade ≥ 3) were artificially collapsed by applying one or two laser pulses (Hamilton Thorn Bioscience Inc, Beverly, MA, USA) before vitrification, as already reported by several authors (Vanderzwalmen et al., 2002; Mukaida et al., 2006; Wang et al., 2007; Van Landuyt et al., 2015; Levi-Setti et al., 2016). The blastocyst was positioned to provide a safe distance between the ICM and the focus of the laser beam, before being exposed to a minimum setting (200 ms) laser pulse to produce a small hole at the junction of two TE cells, resulting in the discharge of fluid from the blastocoel cavity (Figure 1A). Normally, AS occurred within 1 or 2 minutes; rarely a second laser pulse was applied, and for some blastocysts responding slowly, it took up to 5-8 minutes to observe AS and disappearance of the blastocoel (Figure 1B). Subsequently, the embryo was rapidly vitrified (Sciorio et al., 2019).
Figure 1A: Laser drilling at the cellular junction of the trophectoderm before vitrification (red dot). B: Blastocyst after AS. C: A continuous laser beam was emitted tracing the ZP to drill a hole over about one quarter of the ZP surface. D: Blastocyst partly hatched from the ZP after approximately two hours culture (Magnification: x 400).
Blastocyst vitrification
The Cryotop^®^ method (Kitazato Cryotop^®^, Kitazato Corporation, Shizuoka, Japan) initially described by Kuwayama and colleagues (Kuwayama et al., 2005a; 2005b; Kuwayama, 2007) and utilized by several other groups (Mukaida et al., 2003; Mukaida & Oka, 2012) was applied for blastocyst vitrification. The procedure comprised two different steps: equilibration and vitrification, which are both carried out at room temperature (22-25°C). The blastocyst following AS was transferred into the ES containing Trehalose functioning as an osmotic agent, which provides protection of the cellular membranes, in combination with dimethyl sulfoxide (DMSO) and ethylene glycol (EG). Given the critical point of this first step in the study, the time in ES was scrupulously measured by two operators, to establish two groups: the first in which blastocysts were kept in ES for 7-8 minutes (Group A) and the second where embryos were in ES in the range of 9-10 minutes (Group B). Those times were chosen following studies reporting that reducing the equilibration time to 8 minutes can be sufficient for successful vitrification (Mitsuhata et al., 2020). Following the exposure to the ES, the embryos were exposed to the VS containing DMSO and EG, plus trehalose, gentamicin and hydroxypropyl cellulose for 45-60 seconds. Blastocysts were immediately placed on the Cryotop^®^ device, using a narrow and sterile micropipette, with the smallest possible amount of VS, and were quickly immersed into liquid nitrogen (LN_2_). A single blastocyst was always vitrified on each Cryotop^®^ device.
Blastocyst warming and laser-assisted hatching
The Cryotop^®^ Thawing Media Kit (Kitazato Cryotop^®^) was used for warming. In a Nunc 35x10 mm culture dish, 1 ml of Thawing Solution (TS) was heated at 37°C for 30-60 minutes and then positioned on the stage warmer. The Cryotop^®^ device containing the embryo was removed from the LN_2_ and placed as quickly as possible into the dish containing the preheated TS.
The blastocyst instantly fell from the device and could be easily detected in the media under the microscope. After 1 minute, blastocysts were transferred to the Diluent Solution (DS) for 3 minutes at room temperature (22-25°C). At this stage, laser-assisted hatching (Hamilton Thorn Bioscience Inc, Beverly, MA, USA) was completed. Approximately a quarter of the zona pellucida (ZP) was thinned, using up to six laser pulses at a minimum setting (200 ms). The laser pulses were orientated on the ZP where the largest perivitelline space was seen, distant from the cells to avoid any damage (Figure 1C). However, the size of the laser hole would never exceed the thickness of the ZP, which is usually 5-10 µm in diameter. The last step was for 5 minutes, twice, in the Washing Solution (WS) and then the embryo was returned to culture in Quinn’s Advantage Blastocyst medium equilibrated at 37°C, 6% CO2, 5% O2 and 89% N2. An assessment was quickly performed on an inverted microscope to evaluate whether the embryo survived the warming, according to the morphological integrity of the ICM and TE.
After one or two hours of culture, the embryo was re-assessed again and often the re-expansion of the blastocoel was observed, which proves the embryo physiologically survived the warming procedure (Figure 1D). Embryo transfer was normally performed within 2 or 3 hours. Patients received one or a maximum of two blastocysts for transfer according to quality. In case the embryo did not survive, another embryo, if available, was warmed, otherwise the transfer was cancelled. All programmed warmed FET cycles were timed for a day-5 endometrium.
Programmed warmed frozen embryo transfer
FETs were performed in natural and artificial cycles. Women with regular menstrual cycles (25-35 days) underwent downregulation using a GnRH agonist, Triptorelin acetate (Decapeptyl 3 mg) which was administered on day 21 of their menstrual cycle (Li et al., 2022; Zhang et al., 2022). Patients were instructed to take 6 mg estradiol valerate (Progynova) orally, daily from day 2 or 3 of initiation of their period after administration of Triptorelin acetate. A transvaginal scan was performed after the administration of estradiol valerate for about 14 days to measure endometrial thickness. If the endometrial thickness was more than 6 mm, embryo replacement was planned after five full days of progesterone pessary, Cyclogest 400 mg twice daily per vaginal administration. Thus, the day of embryo transfer was agreed upon after a transvaginal scan to prove that the optimal thickness was reached (preferably ≥ 8 mm). All warmed FETs were completed in a day 5 endometrium, after five full days of progesterone pessary administration. For patients who have regular menstrual cycles, as defined above, and who desired a natural cycle, baseline estradiol (E2) and Luteinizing Hormone (LH) were measured between days 2-5 of their menstrual cycle. They were then advised to have blood tests for LH/E2 from day 10 onwards either daily or every two days depending on their LH/E2 result. The blastocyst transfer was arranged four days after the detected LH peak. For luteal supplementation, progesterone vaginal gel (Crinone 8%, Merck Serono SA, Geneva, Switzerland) was utilized, which was continued daily for at least 2 weeks after embryo transfer. Serum β-hCG was measured 14 days after embryo replacement. Clinical pregnancy was determined by a fetal heartbeat on ultrasound screening after 35 days (Li et al., 2022; Zhang et al., 2022).
Clinical outcome definitions
Clinical outcomes in this study were as follows: CPR, LBR, miscarriage rate, and multiple pregnancy rate (MPR). Clinical pregnancy was confirmed when a gestational sac and fetal heartbeat were visualized via an ultrasound examination at about 7 weeks of gestation; after that, any following loss of a fetus was considered a miscarriage. LBR was calculated by dividing the number of live birth deliveries by the number of transfers performed. The evaluated neonatal outcomes were as follows: sex; gestational age; birth weight; preterm birth, defined as a baby born before 37 weeks of gestation; low birth weight, defined as birth weight ≤2500 g; macrosomia, defined as birth weight ≥4000g; the delivery method; and presence of malformations.
Statistical analysis
Data were described as numbers and percentages where appropriate. Statistical analyses were performed with either the Student’s t-test for comparison of mean values or the chi-square test to compare percentages using the Statistical Package for Social Science, version 19.0. Differences were considered statistically significant at a p value <0.05.
RESULTS
A total of 831 vitrified-warmed blastocysts were analyzed in this study, of which 825 survived at the warming step (99.3%). All surviving blastocysts were transferred in 585 FETs. Overall, the CPR per transfer was 68.5%, and LBR and miscarriage rates were 61.0% and 11.0%, respectively (Table 1).
Table 1: Overall clinical outcomes of patients undergoing blastocyst cryopreservation.
The patient’s characteristics are depicted in Table 2. There were no significant differences regarding the mean age of patients, the average number of blastocysts transferred, the basal Follicle Stimulating Hormone (FSH), body mass index, infertility duration or endometrial thickness between the two groups.
Results show the same survival rate after warming (group A: 99.3% and group B: 99.3%), as well as a similar CPR (A: 69.1% versus B: 68.0%). The LBR was slightly different between the groups (A: 63.8% versus B: 58.3%); this was probably due to the relatively low number of FETs performed (n=585); we are still collecting data and, presumably, when we get to more than a thousand FETs, we should reach statistical significance. Further, the multiple pregnancy rate (MPR) (A: 20.8% versus B: 23.5%) was comparable between the two groups. However, observing the overall miscarriage rate, data displayed a statistically significant difference (p<0.05) in favor of group A (7.6%) compared to group B (14.2%; Table 3). The miscarriage rate in the study period for fresh embryo replacements was 15.6%, comparable to that observed in group B.
Table 4 depicts the neonatal outcome of patients who completed the vitrified/warming program. There were no differences between the two groups concerning the parameters evaluated. The only difference observed was the percentage of low birth weight, which was higher in group B: 25.1% compared to group A: 17.0%, but this difference was not statistically significant (p=0.052).
DISCUSSION
The results of this prospective study demonstrate that a shorter equilibration time of 7-8 minutes resulted in optimal survival, CPR, and LBR compared to exposure to ES for 9-10 minutes. Thus, this suggests that extending the duration of ES to 9-10 minutes does not bring any further benefits to the vitrification process. Above all, a longer ES time of 9-10 minutes resulted in a statistically significant higher miscarriage rate (14.2%) compared to 7-8 minutes (7.6%).
Currently, a two-step vitrification protocol is commonly adopted worldwide to cryopreserve human embryos and blastocysts (Vanderzwalmen et al., 2003; Roy et al., 2014; Sciorio et al., 2019; Kadour-Peero et al., 2022; Keshavarzi et al., 2022; Li et al., 2022; Xu et al., 2022). In the first solution, the ES, embryos are in contact with a lower concentration of CPAs, while in the VS they are exposed to a higher percentage of CPAs, which induces a profound volumetric change and osmotic imbalance of embryos. Limited exposure to a high concentration of CPAs is thought to be critical for the efficiency of vitrification, considering that high concentrations might induce osmotic imbalance and oxidative stress (Ginström Ernstad et al., 2019; Estudillo et al., 2021; Agarwal et al., 2022; Berteli et al., 2022; Chen et al., 2022; Ducreux et al., 2024). Therefore, a correct balance between the concentration of CPAs duration of embryo exposure is important for vitrification success (Seki & Mazur, 2012; Agarwal et al., 2022; Ducreux et al., 2024).
It is worth mentioning that temperature also plays an important role during vitrification, regulating the flow rate of CPAs into the cells (Seki & Mazur, 2012). Indeed, in this study, vitrification was performed at room temperature, using the Kitazato protocol, which suggests maintaining blastocysts in VS for 1 minute (45-60 seconds), while the time in ES generally fluctuates between 5 and 15 minutes, which agrees with several published articles (Stanger et al., 2012; Li et al., 2014; Sciorio et al., 2018; 2019; Endo et al., 2020). Animal studies have reported contrasting results on this topic. Kader et al. (2010) evaluated the impact of equilibration time on the DNA integrity of vitrified-warmed mouse blastocysts. They recommended an equilibration time of 8 minutes at room temperature to improve mouse blastocyst DNA integrity. Conversely, Bagis et al. (2005) found that vitrification with a 15 minute equilibration time resulted in a higher hatched blastocyst rate compared to that seen at 5 or 10 minutes. Recently, Berteli et al. (2022) analyzed about 1,000 vitrified mice oocytes and found that a longer equilibration time (10 minutes) produced lower oocyte survival and blastocyst formation rates compared to the 7-minute exposure, concluding that a longer exposure to ES might impair embryo development and cause modification in oocyte lipid composition associated with membrane integrity. Divergent results have also been found in humans, where some reports adopted a fixed equilibration time of 5 minutes (Xie et al., 2010; Shi et al., 2012), while others increase the equilibration phase pre-vitrification to 10 (Hiraoka et al., 2009) or up to 15 minutes (Rezazadeh Valojerdi et al., 2009). Xiong et al. (2016) analyzed this issue in 517 frozen-warmed human embryos. They split the cycles into four groups according to the equilibration time: 5-6 min, 7-8 min, 9-10 min and 11-12 min, and found no differences in terms of survival rate between the groups; but the implantation rate (IR) and LBR were lower in the 5-6 minutes exposure group compared with the three other groups. However, that study was performed on cleavage-stage embryos, while our study was performed on blastocysts, which were artificially collapsed before vitrification and therefore respond differently to the permeation of CPAs. Mitsuhata et al. (2020) reviewed 80 non-expanded and 112 expanded blastocysts and applied two equilibration times pre-vitrification: 8-11 and 12-15 minutes. They found no difference between the two groups in terms of survival and LBR, which agrees with our results. However, in Mitsuhata et al. (2020) study, the 112 expanded blastocysts were not collapsed prior to vitrification, while our study adopted a laser pulse to induce AS in all expanded vitrified embryos.
AS impacts the flow rate of CPAs into the embryo, and thus reducing the ES exposure to 7-8 minutes would be adequate to obtain an efficient vitrification process (Mukaida et al., 2006; Li et al., 2014; Levi-Setti et al., 2016; Sciorio et al., 2018; 2019). Expanding and fully expanded blastocysts enclose a considerable quantity of fluid in the blastocoel, which may increase the risk of ice crystal production during vitrification. On the other hand, when AS is applied, expanded blastocysts collapsed within a few minutes, and were rapidly converted into a morula-like stage without any fluid-filled cavity (Taylor et al., 2010). This is concordant with several studies applying AS prior to vitrification, reporting significant improvements in survival rate, CPR and IR (Mukaida et al., 2006; Taylor et al., 2010; Li et al., 2014; Levi-Setti et al., 2016; Sciorio et al., 2018; 2019).
Mukaida et al. (2006) showed a significant improvement in survival and pregnancy rates in 502 blastocysts using a laser pulse prior to vitrification compared to a retrospective control group. Also, Iwayama et al. (2011) found a significant increase in IR from 34.2% to 59.7% following AS using a laser pulse. Darwish & Magdi (2016) studied the effectiveness of AS prior to vitrification, analyzing about 500 human blastocysts. They noted that the survival rate was significantly higher in the AS group compared with the control group (97.3% versus 74.9%, respectively). Further, they found a significant increase in CPR and IR if AS was performed, concluding that the elimination of blastocoel fluid prior to vitrification significantly enhances clinical outcomes in vitrified-warmed blastocysts. A recent analysis correlated IR, CPR, and LBR in 1,028 consecutive warmed cycles, in which blastocysts were vitrified either with or without AS (Levi-Setti et al., 2016). Results found that IR, CPR, and LBR in the AS group were significantly higher (p<0.05) compared to the non-AS group (IR: 29.9% versus 23.0%; CPR: 36.3% versus 27.9 %; and LBR: 26.5% versus 18.1%, respectively). A study by Desai et al. (2008) noted that blastocysts vitrified without AS experienced more damage and degeneration compared to blastocysts with AS. Similar to our study, George et al. (2016) analyzed 200 FETs and found a comparable survival rate and IR between the two groups (collapsed and non-collapsed); while the CPR approached statistical significance (collapsed 50% versus non-collapsed 37%; p=0.06), and the abortion rate was significantly different between the two groups (collapsed 5.0% versus 13.0% non-collapsed; p<0.05). This is consistent with our study reporting that a shorter exposure to ES pre-vitrification provided a statistically significant reduction in total miscarriage rate (7-8 minutes: 7.6% versus 9-10 minutes: 14.2%; p<0.05).
A concern recently explored by several groups was whether prolonged cryo-storage after vitrification affects embryo viability, competence, and pregnancy outcomes. Several authors have investigated the duration of storage of vitrified oocytes and embryos in LN_2_ and found no change in gene expression (Huo et al., 2021; Canosa et al., 2022; Yan et al., 2023). No impairments were reported by Stigliani et al. (2015) when embryos were stored in LN_2_ for up to 6 years. Along the same lines, Yan et al. (2023) investigated the pregnancy outcomes following different lengths of storage (from less than 3 years up to 10 years). They found a reduced survival rate for blastocysts that were stored for longer than 6 years. Similarly, CPR and LBR were significantly decreased in blastocysts stored for more than 6 years compared with the group frozen for less than 3 years.
No difference was reported in the rates of miscarriage and ectopic pregnancy (Yan et al., 2023). In our study, both groups A and B had matched storage times, which were less than 16 months. The possible mechanisms by which different exposure times to ES influence the abortion rate could be explained by several reasons, such as DNA damage and fragmentation as demonstrated in an animal model study (Kader et al., 2010). Spindle abnormalities were observed in vitrified blastocysts compared with fresh blastocysts (Chatzimeletiou et al., 2012); severe changes in temperature and osmotic and oxidative stresses, as well as damage induced by exposure to a high concentration of CPAs (Agarwal et al., 2022; Sciorio et al., 2023a; 2023b; 2023c).
Additional studies, especially large-scale epidemiological reports are needed to further understand the possible implications that CPAs and cryopreservation might have on the future health of children conceived following ART. However, the current study carries the limitation that it is not a randomized controlled trial, it is a prospective observational cohort study. Also, the possibility cannot be excluded that in those couples with more than two good quality embryos, the best quality one was replaced in the fresh cycle, although attention to allocate the same quality embryo to both groups was always paid in couples with higher numbers of blastocysts.
Finally, it is worth mentioning that the manipulation skills of each embryologist may influence the overall vitrification process; however, in this study, vitrification and warming procedures were performed by only two experienced embryologists; therefore, we do believe that variations in technique between operators presumably did not influence the results.
CONCLUSIVE REMARKS
To conclude, this prospective study shows the relationship between different ES exposure times pre-vitrification on LBR and neonatal outcomes. Our findings demonstrated that laser collapse of expanded blastocysts prior to vitrification and a shorter equilibration time of 7-8 minutes leads to a decreased miscarriage rate and a trend towards a lower percentage of low birth weight. However, there are some potential confounding factors due to the heterogeneous nature of the study sample investigated, which may impair the validity of our conclusions. Therefore, our preliminary results require further investigations with larger studies to confirm the benefit of shorter ES exposure times as a routine protocol to improve the efficacy of the vitrification process.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abdel Hafez FF Desai N Abou-Setta AM Falcone T Goldfarb J. Slow freezing, vitrification and ultra-rapid freezing of human embryos: a systematic review and meta-analysis Reprod Biomed Online 20102020922210.1016/j.rbmo.2009.11.01320113959 · doi ↗ · pubmed ↗
- 2Agarwal A Maldonado Rosas I Anagnostopoulou C Cannarella R Boitrelle F Munoz LV Finelli R Durairajanayagam D Henkel R Saleh R. Oxidative Stress and Assisted Reproduction: A Comprehensive Review of Its Pathophysiological Role and Strategies for Optimizing Embryo Culture Environment Antioxidants 20221147710.3390/antiox 1103047735326126 PMC 8944628 · doi ↗ · pubmed ↗
- 3Bagis H Mercan HO Cetin S Sekmen S. The effect of equilibration time on survival and development rates of mouse pronuclear-stage embryos vitrified in solid surface (SSV) and convential straws: in vitro and in vivo evaluations Mol Reprod Dev 20057249450110.1002/mrd.2026316110514 · doi ↗ · pubmed ↗
- 4Barberet J Barry F Choux C Guilleman M Karoui S Simonot R Bruno C Fauque P. What impact does oocyte vitrification have on epigenetics and gene expression?Clin Epigenetics 20201212110.1186/s 13148-020-00911-832778156 PMC 7418205 · doi ↗ · pubmed ↗
- 5Berteli TS Vireque AA Da Luz CM Borges ED Ferreira CR Navarro PA. Equilibration solution composition and extended exposure to equilibration phase affect embryo development and lipid profile of mouse oocytes Reprod Biomed Online 20224496197510.1016/j.rbmo.2022.01.00635501271 · doi ↗ · pubmed ↗
- 6Bourne H Edgar D Baker H. Sperm preparation techniques Gardner DK Weissman A Howles CM Shoham Z Textbook of Assisted Reproductive Techniques: Laboratory and Clinical Perspectives New York Informa Healthcare;20047991
- 7Canosa S Cimadomo D Conforti A Maggiulli R Giancani A Tallarita A Golia F Fabozzi G Vaiarelli A Gennarelli G Revelli A Bongioanni F Alviggi C Ubaldi FM Rienzi L SIERR The effect of extended cryo-storage following vitrification on embryo competence: a systematic review and meta-analysis J Assist Reprod Genet 20223987388210.1007/s 10815-022-02405-335119549 PMC 9050987 · doi ↗ · pubmed ↗
- 8Chatzimeletiou K Morrison EE Panagiotidis Y Vanderzwalmen P Prapas N Prapas Y Tarlatzis BC Handyside AH. Cytoskeletal analysis of human blastocysts by confocal laser scanning microscopy following vitrification Hum Reprod 20122710611310.1093/humrep/der 34422028018 · doi ↗ · pubmed ↗