Curative Gastrectomy for Advanced Gastric Cancer in a Patient with Idiopathic Multicentric Castleman Disease: A Rare Case Report
Ryohei Kawabata, Yuki Ushimaru, Hisashi Hara, Tomohira Takeoka, Yumiko Yasuhara, Terukazu Yoshihara, Akihiro Kitagawa, Takashi Takeda, Hideo Tomihara, Atsushi Naito, Masahiro Murakami, Shingo Noura, Atsushi Miyamoto

TL;DR
A 75-year-old man with a long history of iMCD successfully underwent curative surgery for gastric cancer after careful multidisciplinary care.
Contribution
Demonstrates successful curative surgery for gastric cancer in a patient with iMCD and sarcopenia through multimodal care.
Findings
Curative distal gastrectomy was performed without complications in a patient with iMCD and sarcopenia.
The patient remains recurrence-free at 24 months after surgery and initiation of tocilizumab.
Multidisciplinary care including preoperative rehabilitation and accurate nodal evaluation was critical for success.
Abstract
Idiopathic multicentric Castleman disease (iMCD) is a rare lymphoproliferative disorder characterized by systemic inflammation and chronic immunosuppression. When solid malignancies such as gastric cancer arise in patients with iMCD, perioperative management becomes particularly challenging due to nutritional decline, reactive lymphadenopathy, and elevated surgical risk. A 75-year-old man with a 26-year history of suspected iMCD treated with low-dose corticosteroids presented with epigastric discomfort. Endoscopy revealed a Borrmann type 2 lesion, and biopsy confirmed poorly differentiated adenocarcinoma. CT showed mild lymphadenopathy along the lesser curvature and left gastric artery, as well as systemic involvement. Inguinal node biopsy confirmed polyclonal plasma cell proliferation consistent with iMCD. The patient also met the Asian Working Group for Sarcopenia (AWGS) criteria for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
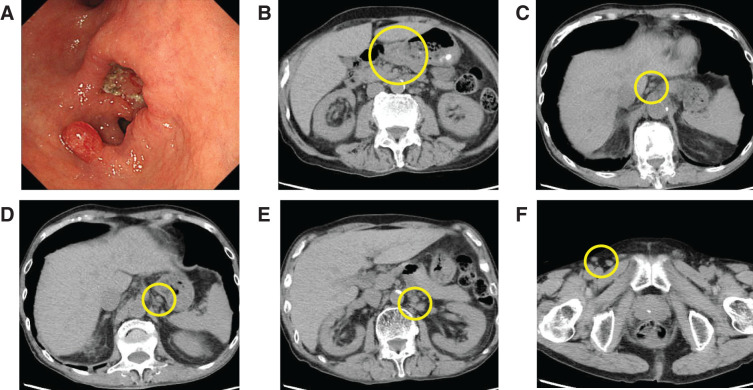 Fig. 1
Fig. 1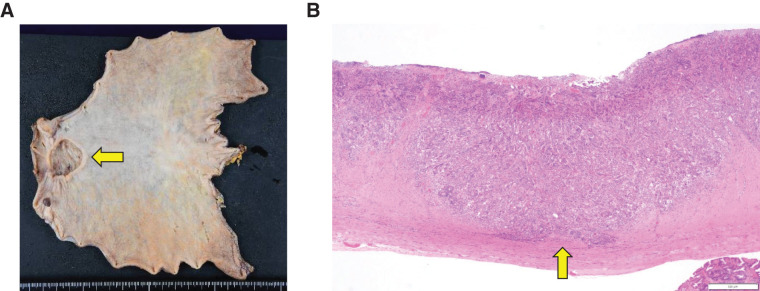 Fig. 2
Fig. 2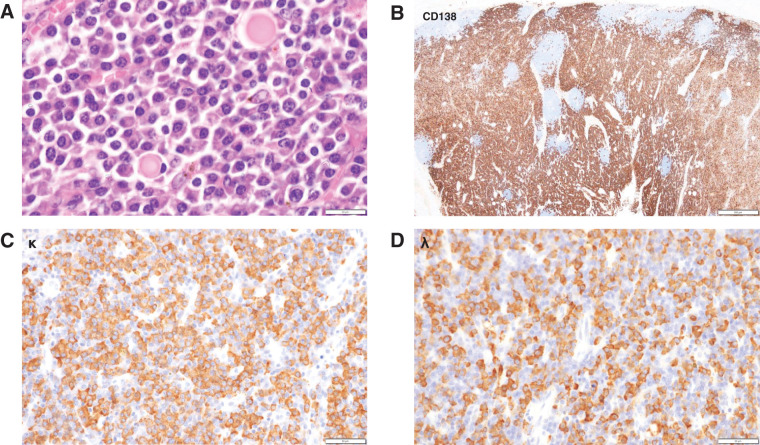 Fig. 3
Fig. 3| Parameter | Value | Unit | Reference range |
|---|---|---|---|
| Hematology | |||
| RBC | 2.60 × 106 | /μL | 4.35–5.55 × 106 |
| Hemoglobin (Hb) | 7.6 | g/dL | 13.7–16.8 |
| Hematocrit (Ht) | 23.6 | % | 40.7–50.1 |
| MCV | 90.8 | fL | 83.6–98.2 |
| MCH | 29.2 | pg | 27.5–33.2 |
| MCHC | 32.2 | g/dL | 31.7–35.3 |
| WBC | 6,840 | /μL | 3,300–8,600 |
| Platelets (PLT) | 27.1 × 104 | /μL | 15.8–34.8 × 104 |
| Biochemistry | |||
| AST | 28 | U/L | 13–30 |
| ALT | 30 | U/L | 10–42 |
| ALP | 136 | U/L | 38–113 |
| LDH | 98 | U/L | 124–222 |
| γ-GTP | 14 | U/L | 13–64 |
| Total bilirubin (T-Bil) | 0.14 | mg/dL | 0.4–1.5 |
| Albumin (Alb) | 1.8 | g/dL | 4.1–5.1 |
| Na | 133 | mEq/dL | 138–145 |
| K | 4.0 | mEq/dL | 3.6–4.8 |
| Cl | 106 | mEq/dL | 101–108 |
| BUN | 40.9 | mg/dL | 8–20 |
| Creatinine (Cre) | 1.82 | mg/dL | 0.65–1.07 |
| C-reactive protein (CRP) | 5.74 | mg/dL | <0.14 |
| Glycated hemoglobin (HbA1c) | 6.2 | % | 4.6–6.2 |
| Coagulation | |||
| Prothrombin time (PT) | 53.9 | % | 70–130 |
| PT-INR | 1.34 | 0.85–1.15 | |
| APTT | 36.5 | Sec | 24–32 |
| Tumor markers | |||
| CEA | 1.8 | ng/mL | <5.0 |
| CA19-9 | 11.5 | U/mL | <37 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple and Secondary Primary Cancers · Viral-associated cancers and disorders · Hepatocellular Carcinoma Treatment and Prognosis
INTRODUCTION
Castleman disease is a rare, non-clonal lymphoproliferative disorder characterized by systemic inflammation and generalized lymphadenopathy.^1,2)^ Among its subtypes, idiopathic multicentric Castleman disease (iMCD) is not associated with viral infection or paraneoplastic syndromes and typically follows a chronic course marked by immune dysregulation, anemia, hypoalbuminemia, and multi-site lymph node enlargement.^3–5)^
When solid malignancies such as gastric cancer occur in patients with iMCD, several clinical challenges arise.^6–8)^ Preoperative staging may be confounded by reactive lymphadenopathy, while long-term corticosteroid use and chronic inflammation can compromise nutritional status and physical function, often leading to sarcopenia, thereby increasing surgical risk.^7,9)^ Such patients require careful multidisciplinary evaluation, individualized surgical planning, and staged systemic therapy to ensure safe and effective oncologic management.^10)^
Although a few case reports have described the coexistence of Castleman disease and solid tumors, cases involving gastric cancer remain extremely rare.^6,11)^ Moreover, no previous studies have reported curative resection of gastric cancer in a patient with a pre-existing diagnosis of long-term treated iMCD.
Herein, we report the case of a patient with long-standing iMCD who underwent curative gastrectomy for advanced gastric cancer. This case highlights the importance of accurate staging, preoperative histologic evaluation of lymphadenopathy, and multidisciplinary perioperative decision-making in managing malignancy in patients with chronic inflammatory disorders.
CASE PRESENTATION
A 75-year-old man was referred to our department with epigastric discomfort. Twenty-six years earlier, he had presented with generalized lymphadenopathy and polyclonal hypergammaglobulinemia, raising suspicion of iMCD. However, a definitive diagnosis could not be established at that time due to the inability to obtain diagnostic tissue. The patient was maintained on low-dose oral prednisolone (3 mg/day). His past medical history included herpes zoster, vertebral compression fracture, type 2 diabetes mellitus, hypothyroidism, and obstructive ventilatory impairment. Preoperative pulmonary function tests showed a forced vital capacity (FVC) of 3.27 L (102.2% predicted) and a forced expiratory volume in one second (FEV_1_) of 1.94 L (59.3% predicted).
Initial laboratory tests revealed severe anemia (hemoglobin 7.6 g/dL), hypoalbuminemia (serum albumin 1.8 g/dL), elevated C-reactive protein (CRP: 5.74 mg/dL), and mild renal impairment (serum creatinine 1.82 mg/dL). Preoperative laboratory findings are summarized in Table 1. Upper gastrointestinal endoscopy revealed a circumferential Borrmann type 2 lesion along the lesser curvature of the antrum (Fig. 1A), and biopsy confirmed poorly differentiated adenocarcinoma. Computed tomography revealed antral wall thickening (Fig. 1B) and mild enlargement (≤10 mm) of lymph nodes along the lesser curvature and around the left gastric artery (Fig. 1C, 1D), as well as systemic lymphadenopathy involving the para-aortic region (Fig. 1E); and the bilateral axillary, supraclavicular, mediastinal, hilar, pelvic, and inguinal regions (Fig. 1F).
(A) Upper gastrointestinal endoscopy showing a circumferential Borrmann type 2 lesion along the lesser curvature of the gastric antrum. (B–F) Plain computed tomography images showing mild wall thickening in the gastric antrum and mildly enlarged lymph nodes (≤10 mm) along the lesser curvature and around the left gastric artery, as well as systemic lymphadenopathy including the para-aortic and inguinal regions.
To evaluate the etiology of lymphadenopathy, an excisional biopsy was performed on a mildly enlarged right inguinal lymph node. Histopathological examination revealed small reactive follicles and dense interfollicular infiltration of polyclonal plasma cells, with scattered Dutcher bodies. Immunohistochemistry showed mixed kappa and lambda light chains without restriction, and staining for human herpesvirus 8 (HHV-8) was negative. These findings were consistent with iMCD.
The clinical stage of the gastric cancer was assessed as cT3N1M0 (cStage III). After multidisciplinary discussion, curative resection of the gastric cancer was prioritized over initiation of iMCD-directed therapy. The patient was also diagnosed with severe sarcopenia according to the criteria of the Asian Working Group for Sarcopenia (AWGS),^12)^ based on decreased grip strength (23.4 kg), slow gait speed (0.83 m/s), and low skeletal muscle index (SMI, 6.2 kg/m^2^). Therefore, in addition to red blood cell transfusion, we initiated nutritional intervention and resistance exercise therapy for sarcopenia. Preoperative intervention lasted approximately 4 weeks. Nutritional support consisted of outpatient dietary counseling, including intake assessment, target energy/protein guidance, and proposal of oral nutritional supplements (ONS). Exercise therapy included leaflet-based resistance training and daily walking. For chronic respiratory disease, a combination of long-acting muscarinic antagonist (LAMA) and beta2-agonist (LABA) was introduced under pulmonologist supervision. Perioperative swallowing assessment and functional conditioning were also provided by speech and physical therapists. The patient subsequently underwent robot-assisted distal gastrectomy with D2 lymphadenectomy and Billroth I reconstruction. The operation lasted 3 hours and 47 minutes with minimal blood loss. No serosal exposure of the tumor was observed intraoperatively, and mild lymph node enlargement was noted in the dissection field. Perioperative corticosteroid supplementation was administered to prevent adrenal insufficiency and inflammatory complications due to long-term steroid use.
Gross examination of the resected specimen revealed a 33 × 30 mm type 2 tumor (Fig. 2). Histologically, the tumor was a poorly differentiated adenocarcinoma that had invaded the muscularis propria (pT2) and showed lymphatic and venous invasion (Ly1c, V1c), but no nodal or perineural invasion. Surgical margins were negative, and the final pathological stage was pT2N0M0 (Stage IB). Resected lymph nodes showed polyclonal CD138-positive plasma cell proliferation without light-chain restriction, consistent with reactive changes related to iMCD (Fig. 3).
(A) Gross appearance of the resected gastric specimen, showing a 33 × 30 mm type 2 tumor in the antrum (arrow). (B) Histological examination of the tumor demonstrating a poorly differentiated adenocarcinoma with invasion into the muscularis propria (pT2).
Histopathological evaluation of a resected lymph node. (A) Hematoxylin and eosin staining reveals dense interfollicular infiltration of plasma cells and reactive germinal centers. (B) Immunohistochemical staining for CD138 confirms polyclonal plasma cell proliferation. (C) Immunostaining for immunoglobulin κ light chain. (D) Immunostaining for immunoglobulin λ light chain, showing no light chain restriction.
The postoperative course was uneventful, and the patient was discharged on postoperative day 9. Tocilizumab therapy was initiated 3 months after surgery, and the patient remains free of gastric cancer recurrence and iMCD flare at 24 months postoperatively.
DISCUSSION
Idiopathic multicentric Castleman disease (iMCD) is a rare lymphoproliferative disorder characterized by IL-6-driven systemic inflammation, anemia, hypoalbuminemia, and generalized lymphadenopathy.^2–5)^ When a solid malignancy such as gastric cancer arises in the context of iMCD, surgical decision-making becomes particularly challenging due to overlapping factors including immunosuppression, nutritional deterioration, and the potential for radiologic overestimation of disease stage caused by reactive lymphadenopathy.^7,8)^
In the present case, preoperative CT demonstrated mild enlargement (up to 10 mm) of lymph nodes along the lesser curvature and around the left gastric artery, leading to a clinical diagnosis of cN1 gastric cancer based on the Japanese Classification of Gastric Carcinoma. However, given the patient’s long-standing iMCD, reactive lymphadenopathy was strongly suspected. To clarify the nature of the nodal findings, an excisional biopsy of a mildly enlarged right inguinal lymph node was performed before surgery. Histological analysis revealed reactive follicles, dense interfollicular polyclonal plasma cell infiltration, scattered Dutcher bodies, negative staining for HHV-8, and no evidence of light chain restriction, findings consistent with iMCD. This confirmed the likelihood of non-metastatic lymphadenopathy and facilitated more appropriate staging and surgical planning. Although PET-CT was initially planned for this patient to further evaluate the extent of lymphadenopathy, the examination was ultimately not performed due to concerns about insurance coverage for iMCD in Japan. According to recent consensus guidelines and the literature, PET-CT is considered useful in assessing the systemic distribution and disease activity of lymphadenopathy in iMCD, and may help distinguish between iMCD and other malignancies such as lymphoma or metastatic disease.^4,13,14)^ However, FDG uptake in iMCD is not specific and may overlap with findings seen in malignancies. Therefore, histological confirmation remains essential. In this case, an excisional lymph node biopsy was performed instead, which allowed for definitive diagnosis and facilitated appropriate treatment planning for the concurrent advanced gastric cancer.
The patient had been treated with low-dose corticosteroids for over 20 years. At the time of cancer diagnosis, he presented with severe anemia (hemoglobin 7.6 g/dL), hypoalbuminemia (serum albumin 1.8 g/dL), and elevated C-reactive protein (CRP: 5.74 mg/dL), indicating significant inflammation and nutritional decline. After multidisciplinary discussion, a decision was made to prioritize curative resection of the gastric cancer. Preoperative preparation included respiratory rehabilitation, transfusion of two units of red blood cells, perioperative steroid coverage, nutritional support and resistance exercise therapy for sarcopenia (conducted over more than 2–3 weeks), and infection control measures. Anti-IL-6 therapy was deferred until wound healing was confirmed.
Tocilizumab, a monoclonal antibody targeting the IL-6 receptor, is considered the preferred alternative to siltuximab in Japan.^2,15,16)^ However, its use in the perioperative setting requires caution due to its potential to suppress CRP responses and delay wound healing. In this case, tocilizumab was safely initiated 3 months after surgery without complication. The patient has remained free from recurrence of both gastric cancer and iMCD flare for 24 months.
According to the risk calculator provided by the National Clinical Database (NCD) of Japan,^17)^ the estimated risks for operative mortality and postoperative pneumonia in this patient were 19.1% and 19.0%, respectively. Despite these high-risk estimates, the patient experienced no perioperative complications. This favorable outcome may be attributed to a multidisciplinary approach involving preoperative respiratory rehabilitation, epidural analgesia for postoperative pain control, and perioperative steroid coverage. In addition, the patient had been diagnosed with severe sarcopenia, and preoperative nutritional support combined with resistance exercise therapy was implemented. According to the 2021 ESPEN guidelines on perioperative nutrition, preoperative nutritional intervention for at least 7–14 days is recommended for malnourished patients, even if surgery must be postponed.^18)^ Furthermore, a meta-analysis in the field of sarcopenia treatment emphasizes the benefit of combined nutritional and resistance exercise interventions in improving physical function and clinical outcomes.^19)^ Although the optimal duration of such intervention remains unclear, in this case, approximately 4 weeks of multidisciplinary prehabilitation was feasible following lymph node biopsy and before the gastrectomy. These interventions likely helped improve his physical function and contributed to a more robust perioperative recovery. These coordinated efforts likely contributed to respiratory stability, immune modulation, and enhanced recovery, even in the setting of long-term immunosuppression.
Coexistence of gastric cancer and iMCD is exceedingly rare, with most reported cases involving incidental diagnosis of Castleman disease during or after surgery.^8,11)^ To the best of our knowledge, this is the first report of curative gastrectomy with D2 lymphadenectomy in a patient with pre-existing, clinically managed iMCD. This case illustrates that with careful staging, multidisciplinary coordination, and appropriately timed systemic therapy, major oncologic surgery can be safely performed even in patients with chronic inflammatory disease.
CONCLUSIONS
We report a rare case of advanced gastric cancer arising during the long-term clinical course of iMCD, in which curative gastrectomy was successfully performed following multidisciplinary planning. This case highlights the importance of accurate clinical staging, preoperative lymph node assessment, and coordinated perioperative management in achieving safe and effective surgical outcomes in patients with chronic inflammatory conditions such as iMCD.
ACKNOWLEDGMENTS
We sincerely thank all medical staff involved in the care of this patient, including physicians, nurses, pharmacists, rehabilitation specialists, pathologists, and other allied health professionals. Their dedicated multidisciplinary efforts were essential for the successful management of this complex case.
DECLARATIONS
Funding
No funding was obtained for this study. The funding body played no role in the design of the study; collection, analysis, and interpretation of data; or writing of the manuscript.
Authors’ contributions
RK and HH collected the clinical data and drafted the manuscript.
RK, YU, and TTakeoka participated in the clinical management of the patient.
YY performed the pathological analysis.
All authors have read and approved the final manuscript, and agree to be held accountable for all aspects of the research.
Availability of data and materials
Not applicable.
Ethics approval and consent to participate
This work does not require ethical considerations or approval. Informed consent to participate in this study was obtained from the patient.
Consent for publication
Informed consent for publication was obtained from the patient.
Competing interests
The authors have no competing interests to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fajgenbaum DC van Rhee F Nabel CS. HHV-8-negative, idiopathic multicentric Castleman disease: novel insights into biology, pathogenesis, and therapy. Blood 2014; 123: 2924–33.24622327 10.1182/blood-2013-12-545087 · doi ↗ · pubmed ↗
- 2Committee for the Guidelines for Castleman Disease. Clinical Practice Guidelines for Castleman Disease, 2020 edition. Tokyo: Japanese Society of Hematology; 2020. (in Japanese)
- 3Liu AY Nabel CS Finkelman BS Idiopathic multicentric Castleman’s disease: a systematic literature review. Lancet Haematol 2016; 3: e 163–75.27063975 10.1016/S 2352-3026(16)00006-5 · doi ↗ · pubmed ↗
- 4Fajgenbaum DC Uldrick TS Bagg A International, evidence-based consensus diagnostic criteria for HHV-8-negative/idiopathic multicentric Castleman disease. Blood 2017; 129: 1646–57.28087540 10.1182/blood-2016-10-746933 PMC 5364342 · doi ↗ · pubmed ↗
- 5Nishimoto N Kanakura Y Aozasa K Humanized anti-interleukin-6 receptor antibody treatment of multicentric Castleman disease. Blood 2005; 106: 2627–32.15998837 10.1182/blood-2004-12-4602 · doi ↗ · pubmed ↗
- 6Zhang X Niyazi S Guo H Mimickers and associated neoplasms of castleman disease. J Clin Transl Pathol 2025; 5: 20–9.
- 7Dong Y Liu B Ju G Concomitant perinephric Castleman disease and renal cell carcinoma initially suspected to be metastasis: a case report and 24 months follow up. Urol Case Rep 2018; 22: 70–2.30479965 10.1016/j.eucr.2018.08.019PMC 6249408 · doi ↗ · pubmed ↗
- 8Shimura Y Hirao T Hara S A case of Castleman’s disease with lymphadenopathy during the treatment of gastric cancer. Gan To Kagaku Ryoho 2019; 46: 739–41. (in Japanese)31164520 · pubmed ↗