Heart Failure in Polycystic Ovarian Syndrome and Hypothyroidism: A Retrospective Large Database Analysis
Evidence E Ohikhuai, Ngozi T Akueme, Seye Olaniyi, Oluwatosin B Iyun, Remil Thomas, Chidinma J Kanu, Bernard Wiredu, Tanvi Narendrula, Okelue E Okobi

TL;DR
This study finds that women with PCOS and hypothyroidism are more likely to develop heart failure and other metabolic conditions compared to those with PCOS alone.
Contribution
The study provides new evidence on the increased cardiovascular risk in PCOS patients with concurrent hypothyroidism using a large national database.
Findings
PCOS patients with hypothyroidism had a 20% higher risk of heart failure compared to those without hypothyroidism.
The combination of PCOS and hypothyroidism was associated with increased risks of T2DM, CKD, and hyperlipidemia.
No significant differences were found in mortality, stroke, or DVT between the two groups.
Abstract
Introduction Polycystic ovarian syndrome (PCOS) carries similar risks to metabolic syndromes, and the population with hypothyroidism and concurrent PCOS may demonstrate exponential cardiovascular risk. There is a paucity of data on the cardiovascular outcomes of the population with PCOS. We aimed to address this gap. Methods We queried the National Inpatient Sample Database (2016-2020), selected the population with a diagnosis of PCOS, and stratified them according to the presence or absence of hypothyroidism. Multivariable logistic regression models were applied to predict the outcomes. The primary outcome was mortality, while secondary outcomes were heart failure (HF), type 2 diabetes mellitus (T2DM), chronic kidney disease (CKD), stroke, hypertension (HTN), hyperlipidemia (HLD), and deep venous thrombosis (DVT). Results There were 78,470 hospitalizations with PCOS, and 14.6%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
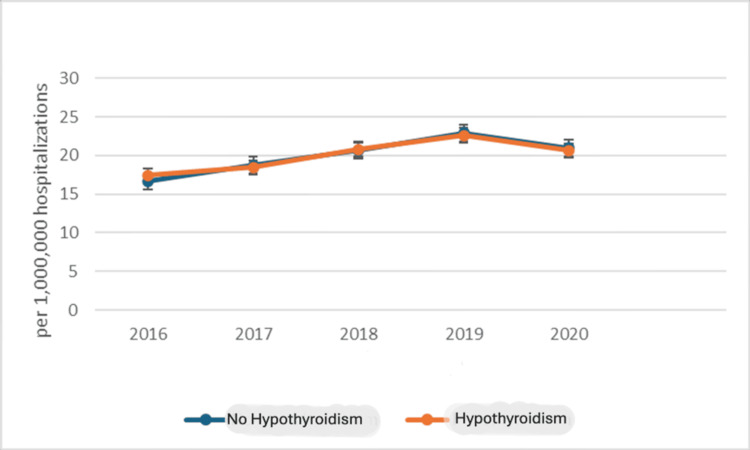 Figure 1
Figure 1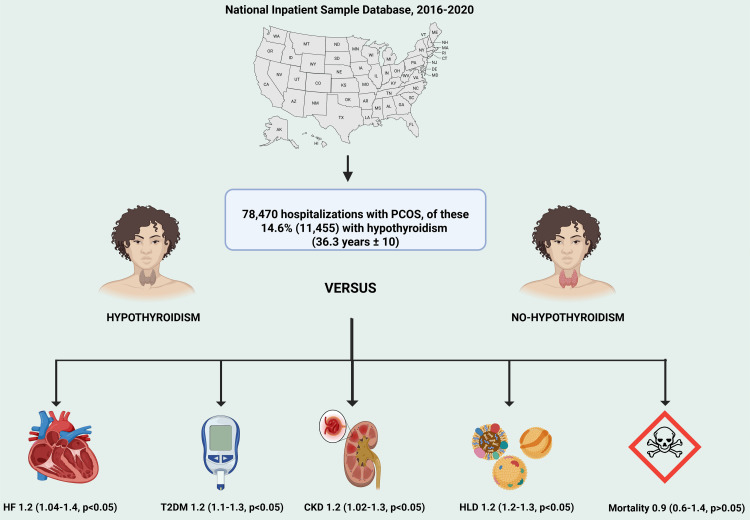 Figure 2
Figure 2| Characteristics | No hypothyroidism (N (%)) | Hypothyroidism (N (%)) | P-value |
| 67,015 (85.4) | 11,455 (14.6) | ||
| Mean age | 32.8 (SD = 9) | 36.3 (SD = 10) | 0.68 |
| Race | |||
| White | 42,730 (65.6) | 8,560 (77.0) | 0.01 |
| Black | 8,670 (13.3) | 540 (4.9) | |
| Hispanic | 8,705 (13.3) | 995 (9.0) | |
| Asian or Pacific Islander | 2,410 (3.7) | 605 (5.4) | |
| Native American | 360 (0.6) | 75 (0.7) | |
| Others | 2,300 (3.5) | 345 (3.1) | |
| Insurance type | |||
| Medicare | 3,625 (5.4) | 1,010 (8.8) | 0.08 |
| Medicaid | 16,580 (24.8) | 2,080 (18.2) | |
| Private insurance | 41,965 (62.7) | 7,640 (66.8) | |
| Self-pay | 2,510 (3.8) | 340 (3.0) | |
| No charge | 140 (0.2) | 20 (0.2) | |
| Others | 2,110 (3.2) | 345 (3.0) | |
| Median household income | |||
| 0-25th percentile | 16,245 (24.4) | 2,430 (21.5) | 0.15 |
| 26th to 50th percentile (median) | 18,080 (27.2) | 3,010 (26.6) | |
| 51st to 75th percentile | 17,160 (25.8) | 2,930 (25.9) | |
| 76th to 100th percentile | 15,000 (22.6) | 2,960 (26.1) | |
| Region of the hospital | |||
| Northeast | 4,125 (15.8) | 650 (13.3) | 0.20 |
| Midwest | 6,435 (29.1) | 1,425 (29.1) | |
| South | 11,400 (43.5) | 2,010 (41.0) | |
| West | 4,230 (16.2) | 815 (16.6) | |
| Location/teaching status of the hospital | |||
| Rural | 4,045 (6.0) | 735 (6.4) | 0.12 |
| Urban nonteaching | 10,225 (15.3) | 1,700 (14.8) | |
| Urban teaching | 52,745 (78.7) | 9,020 (78.7) | |
| Comorbidities | 0.40 | ||
| Coronary artery disease | 1,095 (1.6) | 240 (2.1) | 0.10 |
| Atrial fibrillation | 640 (1.0) | 145 (1.3) | 0.02 |
| Myocardial infarction | 265 (0.4) | 65 (0.6) | 0.01 |
| Inflammatory bowel disease | 530 (0.8) | 75 (0.7) | 0.10 |
| Pulmonary hypertension | 440 (1.0) | 115 (1.0) | <0.01 |
| Hypertension | 11,715 (17.5) | 2,550 (22.3) | <0.01 |
| Acute kidney injury | 2,540 (4.0) | 575 (5.0) | 0.3 |
| Respiratory failure | 2,980 (4.5) | 720 (6.3) | 0.01 |
| Chronic obstructive pulmonary disease | 1,065 (1.6) | 295 (2.6) | 0.03 |
| Major depressive disorder | 14,365 (21.4) | 2,875 (25.1) | 0.01 |
| Bipolar affective disorder | 3,780 (5.6) | 750 (6.6) | 0.7 |
| Generalized anxiety disorder | 18,320 (27.3) | 3,730 (32.6) | <0.001 |
| Smoking | 14,445 (21.6) | 2,195 (19.2) | <0.001 |
| Breast cancer | 165 (0.3) | 50 (0.4) | 0.2 |
| Current chronic long-term steroid use | 555 (0.8) | 130 (1.1) | 0.5 |
| Obesity | 31,980 (47.7) | 5,985 (52.3) | 0.01 |
| Pulmonary embolism | 805 (1.2) | 95 (0.8) | 0.04 |
| Inpatient procedures | |||
| Percutaneous coronary intervention | 115 (0.2) | 15 (0.1) | 0.4 |
| Blood transfusion | 1,500 (2.2) | 295 (2.6) | 0.2 |
| Hypothyroidism | No hypothyroidism | P-value | |
| Length of hospitalization | 4 days | 3.6 days | <0.001 |
| Cost of hospitalization | $43,509 | $39,943 | <0.001 |
| White % (n) | Black % (n) | Hispanic % (n) | Asian/Pacific Islander % (n) | Native American % (n) | Others % (n) | P-value | |
| No hypothyroidism | 65.56 (42,730) | 13.30 (8,670) | 13.36 (8,705) | 3.70 (2,410) | 0.55 (360) | 3.53 (2,300) | <0.01 |
| Hypothyroidism | 76.98 (8,560) | 4.86 (540) | 8.95 (995) | 5.44 (605) | 0.67 (75) | 3.10 (345) | <0.01 |
| PCOS prevalence by race | 67.23 (51,290) | 12.07 (9,210) | 12.71 (9,700) | 3.95 (3,015) | 0.57 (435) | 3.47 (2,645) | <0.01 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHormonal Regulation and Hypertension · Cardiovascular Function and Risk Factors · Liver Disease Diagnosis and Treatment
Introduction
An increased risk of cardiovascular disease (CVD) has been observed in women who have been diagnosed with polycystic ovarian syndrome (PCOS) [1]. These women also exhibit a higher prevalence of various modifiable risk factors such as diabetes, dyslipidemia, hypertension (HTN), abdominal adiposity, obesity, smoking, heightened alcohol consumption, depression, anxiety, and perceived stress. These factors are associated with a greater likelihood of developing cardiometabolic events [1].
The thyroid gland directly impacts human metabolism, particularly cardiovascular metabolism [2]. Hypofunction of the thyroid gland, ultimately leading to hypothyroidism, affects 3% of persons globally [3]. PCOS impacts 8-13% of women in their reproductive years, with about 70% of those affected being undiagnosed worldwide [4].
Hypothyroidism is known to exert direct negative chronotropic and inotropic impacts on the myocardium, resulting in a diminished heart rate and impaired contractile function, thereby compromising systemic circulation [5]. Concurrent PCOS contributes to an enhanced cardiovascular risk profile, predominantly through the pathophysiology of insulin resistance, which predisposes individuals to adiposity, glucose intolerance, and type 2 diabetes mellitus (T2DM), all factors that amplify cardiac workload and stress. The convergence of these abnormalities can catalyze the development of heart failure (HF) and other poor cardiovascular outcomes [6,7].
Emerging evidence suggests that oxidative stress, sustained systemic inflammation, and direct myocardial impairment are additional mechanistic pathways by which these conditions may promote cardiac dysfunction [8]. However, the cardiovascular profile of the PCOS population with and without hypothyroidism is lacking. Given the surmounting data correlating these endocrine disorders with cardiac morbidity, this research endeavor is concentrated on delineating the epidemiological linkage and mechanistic interplay of hypothyroidism within the hospitalized PCOS patient cohort and HF and other cardiovascular outcomes. With the era of artificial intelligence and machine learning, using large datasets like this study presents the opportunity for risk stratification and early detection, which may provide better outcomes [9].
Materials and methods
This study has been reported following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [10].
Database
The data used in the study was obtained from the US National Inpatient Sample Database, which covers the period from 2016 to 2020. The National Inpatient Sample Database comprises information about hospital stays across the United States based on billing data submitted by hospitals to statewide data organizations. This database represents more than 97% of the US population [11]. A weighted dataset is generated annually, comprising a 20% stratified sample of patient discharges from community hospitals in the United States. This sampling excludes long-term acute care hospitals and rehabilitation centers. The dataset is designed to achieve national estimates. The 2016-2020 datasets are coded using the International Classification of Diseases, Tenth Revision, and Clinical Modification/Procedure Coding System (ICD-10-CM/PCS). In the NIS, diagnoses are categorized as principal or secondary. This study's principal diagnosis refers to the main ICD-10 code assigned to the hospitalization, while secondary diagnoses comprise any other ICD-10 codes (see Appendices). ICD-10 codes used in our study have been previously validated in other studies [12,13].
Study population and criteria
We performed a retrospective cohort study of hospitalizations from 2016 to 2020 with a principal or secondary diagnosis of PCOS and a secondary diagnosis of hypothyroidism. We used ICD-10 codes obtained from other studies with validated ICD-10 codes [14,15]. This study was exempted from the Institutional Review Board approval because it utilized de-identified data available online at www.hcup-us.ahrq.gov.
From 2016 to 2020, hospitalizations related to PCOS were analyzed for the study population. The study parameters comprised sociodemographic characteristics, medical comorbidities, hospital attributes, and primary and secondary outcomes. We excluded patients aged <18 years. Baseline hospitalization characteristics for PCOS with and without a secondary diagnosis of hypothyroidism were studied.
Data analysis
We selected the population with a diagnosis of PCOS and stratified them according to the presence or absence of hypothyroidism. Then, the chi-squared test and Student's t-test were used to compare categorical and continuous variables. Continuous variables were represented as mean + standard deviation (SD), while categorical variables were represented as percentages. When comparing variables or groups within this data, we assumed that they were independent of each other and had enough statistical power. If this assumption was false, we used Fisher's exact test instead of the chi-squared test. Similarly, if the data was not normally distributed, we replaced Student's t-test with the Mann-Whitney U test. For trends in hospitalization, we utilized the Cochran-Armitage trend analysis to assess the proportion of this population of interest, i.e., hypothyroidism, over the study period, i.e., "YEARS".
Multivariable logistic regression models were applied to account for patient- and hospital-level confounders and to predict the outcomes. We modeled the dependent variable as the outcomes of interest while using independent variables as predictors. We also included their baseline characteristics to account for patient- and hospital-level confounders. This model allowed for the estimation of outcomes using a two-sided p-value and confidence interval (CI). A p-value of ≤0.05 was the statistical threshold of significance. All statistical analyses were conducted using the SAS 9.4 software (SAS Inc., Cary, NC, USA).
Outcomes of interest
Our primary outcome was mortality, while secondary outcomes were T2DM, HF, chronic kidney disease (CKD), stroke, HTN, hyperlipidemia (HLD), and deep venous thrombosis (DVT).
We also compared the median cost of hospitalization, mean length of hospitalization (length of stay (LOS)), and trend of hospitalization between both groups.
Results
Baseline characteristics
During the study period, a total of 78,470 hospitalizations were identified with a diagnosis of PCOS, of which 14.6% (11,455 patients) had concurrent hypothyroidism.
Regarding racial distribution, the majority of PCOS patients were White (67.2%), followed by Hispanic (12.7%), Black (12.1%), Asian/Pacific Islander (4%), and Native American (0.6%). When stratified by hypothyroidism status, 77% of patients in the hypothyroid group were White, compared to 65.6% in the non-hypothyroid group (χ²(5) = 105.32; p < 0.01; Cramér's V = 0.11), highlighting a significant racial discrepancy.
Notably, obesity (BMI >30 kg/m²) was highly prevalent in both groups, affecting 52.3% of hypothyroid patients compared to 47.7% of non-hypothyroid patients, indicating a significant association (χ²(1) = 6.43; p = 0.01; Cramér's V = 0.03). Psychiatric comorbidities were also more frequent in the hypothyroid group, with generalized anxiety disorder affecting 32.6% vs. 27.3% (χ²(1) = 8.72; p < 0.01; Cramér's V = 0.04) and major depressive disorder affecting 25.1% vs. 21.4% (χ²(1) = 7.51; p < 0.01; Cramér's V = 0.03).
Other significant differences included the prevalence of HTN (22.3% vs. 17.5%; χ²(1) = 18.75; p < 0.01; Cramér’s V = 0.05) and smoking rates (19.2% vs. 21.6%; χ²(1) = 9.21; p < 0.01; Cramér's V = 0.04) (Table 1).
Outcomes
Compared to the non-hypothyroid group, the population with hypothyroidism exhibited a significantly higher likelihood of HF, CKD, T2DM, and HLD, with odds ratios of 1.2 (95% CI: 1.04-1.4) for HF, 1.2 (95% CI: 1.02-1.3) for CKD, 1.2 (95% CI: 1.1-1.3) for T2DM, and 1.2 (95% CI: 1.2-1.3) for HLD (p < 0.05 for each). Chi-squared analyses revealed statistically significant differences in prevalence between the groups, with test statistics of χ²(1) = 7.02 and p = 0.008 for HF, χ²(1) = 6.89 and p = 0.009 for CKD, χ²(1) = 8.44 and p = 0.004 for T2DM, and χ²(1) = 9.51 and p = 0.003 for HLD, indicating a small but meaningful effect size (Cramér's V ranging from 0.03 to 0.04).
Additionally, hypothyroidism was associated with a longer length of hospitalization (four vs. 3.6 days) and increased hospitalization costs (39,943; p < 0.001), with chi-squared results demonstrating statistical significance (χ²(1) = 12.65 and p < 0.001 for LOS and χ²(1) = 15.78 and p < 0.001 for cost) and corresponding effect sizes (Cramér's V = 0.05-0.06). These findings emphasize the significant impact of hypothyroidism on hospitalization burden and cardiovascular/metabolic outcomes among patients with PCOS (Table 2).
A Cochran-Armitage trend test was performed to assess changes in the proportion of hypothyroidism among PCOS hospitalizations over the study period. The results indicated that the variation in hypothyroidism prevalence across the years was not statistically significant (χ²(1) = 1.02; p = 0.31), confirming a stable trend (Figure 1).
Trend analysis of hospitalization of the polycystic ovarian syndrome population stratified according to the presence or absence of hypothyroidism.
The chi-squared analysis comparing racial distribution between PCOS patients with and without hypothyroidism demonstrated a statistically significant difference (χ²(5) = 105.32; p < 0.01; Cramér's V = 0.11), highlighting a notable racial discrepancy. White patients had a higher prevalence of hypothyroidism (76.98%) compared to Black (4.86%) and Hispanic (8.95%) patients, which may suggest demographic variations in endocrine risk factors (Table 3).
Discussion
This study had intriguing results. It demonstrated that among 78,470 hospitalizations with PCOS, those with concurrent hypothyroidism had a higher likelihood of HF, CKD, T2DM, and HLD. However, there was no difference in terms of mortality, HTN, stroke, and DVT in the hypothyroid vs. non-hypothyroid group (Figure 2).
Graphical abstract comparing the population with PCOS with and without hypothyroidism.PCOS: polycystic ovarian syndrome; HF: heart failure; CKD: chronic kidney disease; T2DM: type 2 diabetes mellitus; HLD: hyperlipidemiaThis figure is an original creation of the authors.
These findings suggest an association between PCOS, hypothyroidism, T2DM, and HLD, consistent with recent international studies [16,17]. In one study, 52 euthyroid and 48 subclinical hypothyroidism (SCH) research participants were identified from a hospital-based cross-sectional study conducted among 100 PCOS patients. It was observed that the Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) and fasting serum insulin were significantly elevated in the SCH group compared to the euthyroid group [17]. This may result from the complex relationship between insulin resistance indices and thyroid-stimulating hormone (TSH) levels, explained by the tendency of hypothyroidism to increase adiposity and pro-inflammatory markers [17]. PCOS, obesity, thyroid dysfunction, and autoimmunity interact uniquely to create a complicated pathophysiological pathway that intensifies insulin resistance and raises the metabolic and cardiovascular risk in PCOS-affected women [18]. A meta-analysis of 28 studies also demonstrated higher insulin resistance in individuals with SCH, which is intriguing as insulin resistance is a central pathogenic feature of PCOS [19]. Another study revealed its unfavorable effects on high-density lipoprotein (HDL)-cholesterol and triglycerides (TG) [20].
Several studies have also shown an increased likelihood of HF and CKD in PCOS patients with coexisting hypothyroidism [18,21]. Even in the context of normal TSH levels, the hypothyroid state, precisely a low triiodothyronine level, has been linked to a poor prognosis and diminished cardiac performance in HF. Low levels of thyroid hormones alter cardiac gene expression and increase systemic vascular resistance, both resulting in a reduction of cardiac contractility and cardiac output [22]. When compared to 30 euthyroid control patients, a group of 54 individuals with SCH and elevated TSH had adverse measurements of multiple diastolic and systolic left ventricular function, assessed by echocardiography [23]. The increased likelihood for the development of CKD in PCOS patients with concurrent hypothyroidism could be explained by PCOS and hypothyroidism being independently associated with T2DM, which, when poorly controlled, can lead to diabetic nephropathy, which is known to be the most common cause of end-stage renal disease (ESRD) in the United States [24]. A prospective follow-up of 480 euthyroid patients and 89 patients with SCH for 26 months revealed adverse renal outcomes in the SCH group, with increased hazard ratios (HRs) for a composite outcome incorporating doubling of serum creatinine (SCr) and ESRD [25].
Previous studies that have examined the effect of PCOS on vascular diseases like HTN, DVT, and stroke showed increased odds of these diseases in the hypothyroid group compared to the non-hypothyroid group [26]. This could be explained by the effect of PCOS with concurrent hypothyroidism on lipid profile. Women with PCOS are prone to dyslipidemia. The most common dyslipidemia features in PCOS patients are hypertriglyceridemia, decreased HDL-cholesterol concentrations, and small, dense low-density lipoprotein (LDL) particles characteristic of the atherogenic lipoprotein phenotype [27]. Therefore, it is speculated that PCOS patients have a higher tendency to develop atherosclerosis. Atherosclerosis drives the narrowing of the blood vessels, increasing total peripheral resistance and blood pressure. Reduction of the luminal diameter of the blood vessels also reduces blood flow to different organs like the brain and limbs, resulting in ischemia, as seen in stroke. Deposition of LDL particles in the lumen of blood vessels causes oxidative stress and subsequent endothelial injury [28]. LDL are thrombogenic particles that cause the recruitment of platelets, and all these contribute to the narrowing of the blood vessels and, hence, stasis, which increases the likelihood of DVT [27,29].
Contrary to initial expectations, this study did not reveal significant differences regarding HTN, stroke, DVT, and overall mortality. This was in keeping with a few other observational studies, one of which enrolled 3,078 subjects with and without hypothyroidism and demonstrated no significant differences in office systolic and diastolic blood pressure measurements [30]. Furthermore, although we sought to compare both arms (hypothyroidism and no hypothyroidism), the population with PCOS is at baseline already predisposed to obesity, T2DM, heart disease, and HTN [4]. This may explain the non-difference in some outcomes of this study. Another possibility may be attributed to medical advances in CVD and especially for acute heart diseases, including specialized coronary care units, new pharmaceuticals with improvements in HTN management, the use of statins to lower circulating cholesterol levels, the development and timely use of thrombolysis, and advanced surgical procedures such as bypass surgery and angioplasty [31]. A more active approach to prevention and disease management, and behavioral changes such as reduced smoking rates and improved diet, further diminished the likelihood of heart and vascular diseases and the associated mortality risk [31-33]. The age group being studied may also be of value in this finding. With a mean of 36.3 years, it is unlikely to find an overwhelming difference in mortality, given that age is one of the single most significant variables that impact mortality [34]. We may argue that the accumulation of events resulting from the hypothyroid state may predispose to mortality down the road, but this study cannot draw such conclusions.
Nonetheless, this study has many strengths. Firstly, this population of 78,470 provides one of the largest databases of individuals with PCOS. Secondly, this sample had a decent inclusion of minority races, including Blacks, Hispanics, Asians, and Native Americans, for better generalizability to the real-world scenario. Thirdly, given the relatively young age of this population, which is relatively healthy, these findings are clinically thought-provoking since this population is often not burdened with comorbidities that may confound associations.
Limitations
It should be noted that this study has some limitations due to its retrospective and observational design. We could not obtain granular data such as laboratory values, echocardiogram parameters, levels of serum TSH, antibody titers, or thyroid ultrasound data. Additionally, we could not assess the severity of comorbidities, contraindications to procedures, and patients' beliefs and preferences. Age at diagnosis of hypothyroidism and the time difference between diagnosis of hypothyroidism and HF could not be ascertained; thus, causality cannot be inferred. Furthermore, despite multivariable analysis, confounding factors, such as obesity severity, medication use such as metformin and levothyroxine, or socioeconomic status, may influence outcomes, as could selection bias from the increased evaluation of the PCOS group. Nonetheless, this study holds significant power, involves a relatively large minority population, and adds to the body of knowledge through hypothesis-generating associations that may inform future studies.
Conclusions
This analysis of a large nationally representative database indicates that the population with PCOS and concurrent hypothyroidism may be at a significantly higher risk of developing HF, CKD, T2DM, and HLD compared to those without hypothyroidism. These findings emphasize the need for a comprehensive approach to patient care, as endocrine disorders and cardiovascular health are closely interrelated. Future studies that may inform guideline recommendations, clinical risk stratification, early detection, and management are warranted.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Risk and incidence of cardiovascular disease associated with polycystic ovary syndrome Eur J Prev Cardiol Wan Z Zhao J Ye Y 156015703120243837325910.1093/eurjpc/zwae 066 · doi ↗ · pubmed ↗
- 2Thyroid disorders and cardiovascular manifestations: an update Endocrine Paschou SA Bletsa E Stampouloglou PK 6726837520223503231510.1007/s 12020-022-02982-4 · doi ↗ · pubmed ↗
- 3The epidemiology of thyroid disease Br Med Bull Vanderpump MP 39519920112189349310.1093/bmb/ldr 030 · doi ↗ · pubmed ↗
- 4Polycystic ovary syndrome (PCOS) 2 2024 Eunice Kennedy Shriver 2024 https://www.nichd.nih.gov/health/topics/factsheets/pcos
- 5What is the association of hypothyroidism with risks of cardiovascular events and mortality? A meta-analysis of 55 cohort studies involving 1,898,314 participants BMC Med Ning Y Cheng YJ Liu LJ 211520172814824910.1186/s 12916-017-0777-9PMC 5289009 · doi ↗ · pubmed ↗
- 6Obesity and cardiovascular disease: a scientific statement from the American Heart Association Circulation Powell-Wiley TM Poirier P Burke LE 01010143202110.1161/CIR.0000000000000973 PMC 849365033882682 · doi ↗ · pubmed ↗
- 7Insulin resistance: an additional risk factor in the pathogenesis of cardiovascular disease in type 2 diabetes Heart Fail Rev Patel TP Rawal K Bagchi AK 11232120162654237710.1007/s 10741-015-9515-6 · doi ↗ · pubmed ↗
- 8Oxidative stress and inflammation in the evolution of heart failure: from pathophysiology to therapeutic strategies Eur J Prev Cardiol Aimo A Castiglione V Borrelli C 4945102720203141271210.1177/2047487319870344 · doi ↗ · pubmed ↗