Periodontitis as a risk factor for colorectal cancer: systematic review and meta-analysis
Rosita Elena Espejo-Carrera, Tammy Margarita Honores-Solano, Teresa Verónica Ulloa-Cueva, José Antonio Caballero-Alvarado, Carlos Alberto Minchón-Medina, Angel Steven Asmat-Abanto

TL;DR
This study finds that periodontitis is not a general risk factor for colorectal cancer, but it may increase the risk in men.
Contribution
The study identifies a gender-specific risk of colorectal cancer associated with periodontitis in men.
Findings
Periodontitis is not a general risk factor for colorectal cancer (RR=1.34; 95% CI: 0.96-1.89).
Men with periodontitis have a 32% increased risk of colorectal cancer (RR=1.32; 95% CI: 1.16-1.50).
The evidence for the general population has very low certainty, while the evidence for men has moderate certainty.
Abstract
Primary studies on the association between periodontitis and colorectal cancer (CRC) may have insufficient statistical power to reach a reliable conclusion. In this regard, the present systematic review and meta-analysis were conducted to determine whether periodontitis is a risk factor for CRC. A systematic search was carried out in five databases, which included cohort and case-control studies published up to July 3, 2024, in which periodontitis was evaluated as a risk factor for CRC using relative risk (RR), hazard ratio (HR) or odds ratio (OR). The Newcastle-Ottawa Scale (NOS) was used to assess the risk of bias, and the GRADE system was used to determine the certainty of the evidence. Of 1476 articles retrieved, 8 cohort studies were included for qualitative analysis and meta-analysis. The overall synthesis showed that periodontitis is not a risk factor for CRC (RR=1.34; 95% CI:…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
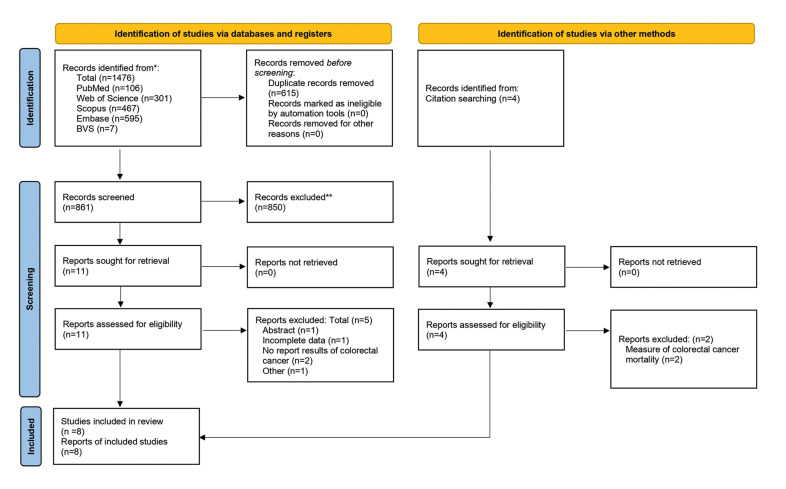 Figure 1
Figure 1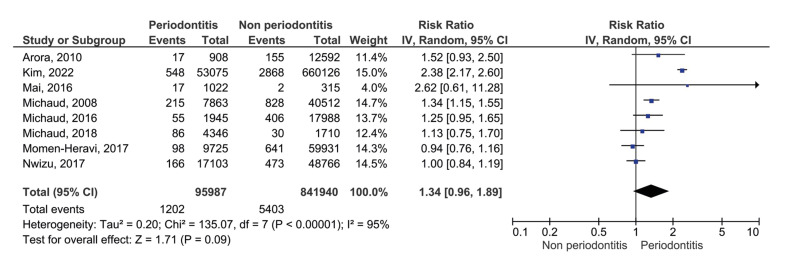 Figure 2
Figure 2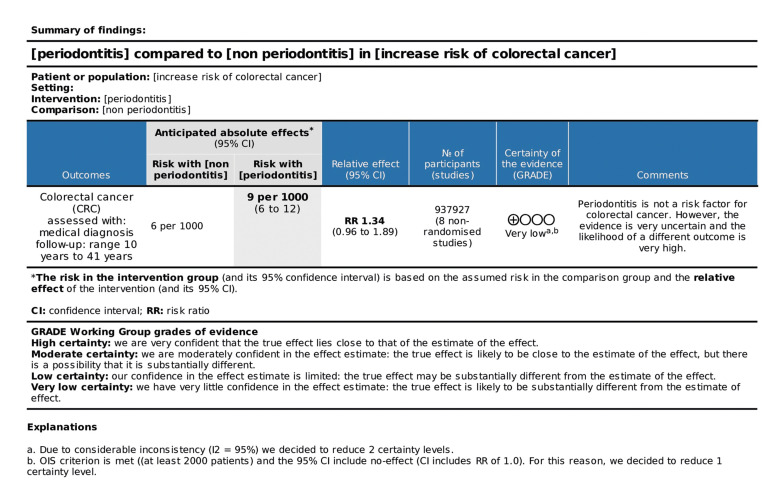 Figure 3
Figure 3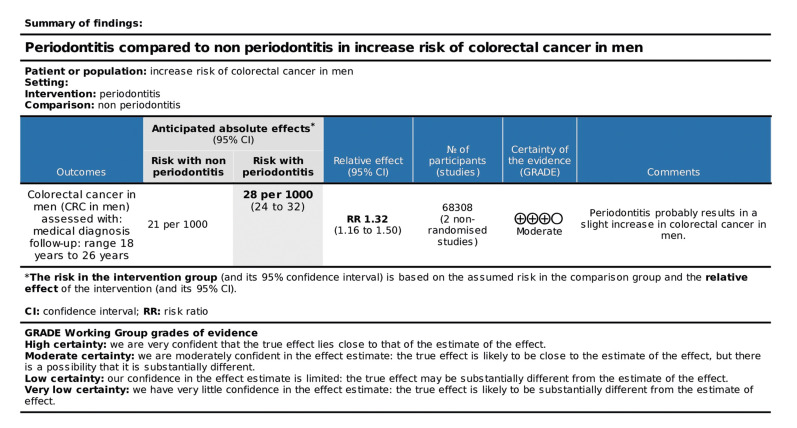 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral Health Pathology and Treatment · Oral microbiology and periodontitis research · HIV/AIDS oral health manifestations
Introduction
Periodontitis, one of the most prevalent inflammatory diseases, causes progressive and irreversible destruction of periodontal tissues, which eventually leads to mobility and tooth loss. The most serious condition of this disease affects between 10.8 and 11.2% of the world's population (1,2).
Colorectal cancer (CRC) is one of the leading causes of morbidity and mortality worldwide, and it is ranked second as regards the number of deaths associated with malignant neoplasms in both men and women. Furthermore, it is the third most commonly diagnosed form of cancer, accounting for approximately 10% of all new cases of cancer (3-6).
Numerous pathophysiological mechanisms, such as abnormal cell proliferation, cell differentiation, resistance to apoptosis, invasion of adjacent structures, and metastasis, are involved in colorectal carcinogenesis (4). These processes are initiated by the complex interaction of genetic and environmental factors, including sedentary lifestyle, obesity, alcohol consumption, smoking, and intestinal microbiota (3,4). Primary and secondary prevention and education about risk factors are essential elements for reducing the burden of this disease and improving prognosis and survival rates (5,7). Although there are systemic treatments, the rapid progress of the disease and its resistance to existing treatments have generated the need to investigate its risk factors, progression, and resistance to therapy (6).
The interaction of cancer cells with the microbiota is a unique feature in CRC compared to other types of cancer. Under normal conditions, the microbiota plays a protective role by participating in immunological homeostasis and the growth of intestinal lymphatic tissues; however, a change in balance leads to the proliferation of opportunistic pathogenic bacteria (6). In the cases of CRC, two specific species of periodontal bacteria are outstanding, namely F. nucleatum and P. gingivalis; the former has been more noTable in regional lymph node metastases (8). These pathogens produce harmful metabolites, including toxins and antigens, that cause maladaptive immune responses and inflammation, damage to DNA, genomic instability, and tumor progression (6).
Translocation of periodontal pathobionts with oncogenic properties and subgingival proinflammatory mediators could potentiate carcinogenic agents, thereby changing the conditions favoring the development and progression of CRC (6,9).
Despite the growing evidence that periodontitis could be a risk factor for CRC, the primary studies may have insufficient statistical power to reach a reliable conclusion. In this sense, the present systematic review and meta-analysis were conducted to evaluate the possible association between periodontitis and the risk of CRC.
Material and Methods
- Protocol and registration
The present systematic review was carried out according to the Preferred Reporting Items for Systematic Reviews and Metanalyses checklist (PRISMA, 2020) (10), and the protocol was registered in PROSPERO under the reference number CRD42024557822.
- Focused question
The research question: Is periodontitis a risk factor for colorectal cancer in adult patients? The question was raised according to the PECOS search strategy (population/patients, exposure, comparison, results, and design of study), where P = adults, E = exposure to periodontitis, C = absence of periodontitis, O = risk of colorectal cancer, and S = cohort and case-control studies.
- Eligibility criteria and process of selection
The observational cohort design and case-control studies included published until July 3, 2024, which studied periodontitis as a risk factor for CRC in adult patients (Over 18 years of age) and calculated the odds ratio (OR), relative risk (RR) or hazard ratio (HR). The excluded studies did not have an independent statistical analysis of the risk of CRC, those with incomplete data, fewer than 1000 participants, and a follow-up period of less than 5 years.
- Operational definitions
Periodontitis was diagnosed using clinical, radiographic assessment, and epidemiological periodontal indicators. Hospital records and self-reports were also considered.
- Search strategy
The search was carried out in the electronic databases of PubMed/Medline, Web of Science, Scopus, Embase, and BVS, as well as manual searches in the reference lists of all included studies and revisions previously published. The complete search strategy, adapted according to the syntax rules of each database, is presented in Supplement 1.
- Data extraction and synthesis
The bibliographic search results were uploaded to the Rayyan application for systematic revisions (https://www.rayyan.ai/), and the duplicate records were eliminated. Two researchers (T.H.S. and T.U.C.) independently selected the articles to be analyzed, first by title and abstract, then four researchers working in pairs (T.H.S. with T.U.C. and R.E.C with A.A.A) analyzed the complete texts. Any disagreement was discussed among the above-mentioned researchers. Therefore, the data was independently extracted and entered into an Excel spreadsheet (Microsoft® Excel® for Office 365). Afterward, the articles selected and data extracted were revised and approved by a fifth expert investigativ e (J.C.A.).
- Risk of bias and certainty of evidence
The studies included were analyzed using the Newcastle-Ottawa Scale (NOS) tool to assess the risk of bias. The quality of evidence of the studies included in the meta-analysis was evaluated by the GRADE tool, using the GRADEpro GDT software (11).
- Statistical analysis
Data collected from the studies selected for the meta-analysis were processed using RevMan software (Review Manager v.5.3, The Cochrane Collaboration) to evaluate periodontitis as a risk factor for CRC. The random effects model was applied to develop the forest plot, and the heterogeneity between the studies was assessed using the I2 index. A sensitivity analysis was also performed to verify each study's influence on the pooled results. Subgroup analysis was performed to determine potential sources of variability. Moreover, an assessment of potential publication bias was performed using Egger's test and Stata 16.0 software (StataCorp LLC, College Station, TX).
- Summary of results
The primary outcome was periodontitis as a risk factor for CRC. The information required from each study was collected in a preliminary summarized Table, and results with sufficient data to calculate an effect estimate were used for the meta-analysis.
Results
- Selection of studies
As presented in the PRISMA 2020 flowchart (12) (Fig. 1), 1476 records were retrieved. After removing duplicates and screening by title and abstract, 11 articles (10 cohort and one case-control study) remained for full-text evaluation, of which 5 (4 cohort and one case-control) were excluded. After manually searching the references of previous systematic reviews, four additional studies were retrieved, of which two were excluded. The reasons for excluding studies are described in detail in Supplement 2. Finally, eight studies were chosen for qualitative analysis and meta-analysis.
- Characteristics of studies
In the 8 cohort studies included (Table 1), 988,897 subjects were evaluated; the study with the smallest number of participants had 1,337 (1,022 exposed and 315 unexposed) (13), and the one with the largest number had 713,201 (53,075 exposed and 660,126 unexposed) (14). The ages of the patients studied ranged from 15 (14) to 85 years (13); the shortest follow-up period was 10 years (14), and the longest was 41 years (15).
The included studies were conducted in the United States (13,16-20), Sweden (15), and Korea (14). All studies declared that they had been funded; while five (14-17,19) mentioned that there was no conflict of interest, two (13,20) did not mention it, and one (18) indicated that the financing agent participated in the design and data collection.
- Risk of bias
As shown in Table 2, most of the studies included in the present analysis had a low risk of bias (13,14,16,17,19,20). The NOS categories with the lowest compliance were the representativeness of the cohort exposed and the determination of exposure.
Figure 1. Flow chart for inclusion of the studies evaluating periodontitis as a risk factor for CRC.
- Meta-analysis of synthesis
The 8 cohort studies were analyzed using the random effects model and considering the relative risk (RR) as the measure of effect. The global synthesis showed a RR of 1.34 (95% CI: 0.96-1.89) and p=0.09, with considerable general heterogeneity (I2=95%; p<0.00001), as shown in the forest plot of Fig. 2. In this sense, because the CI crosses the line of no effect, periodontitis would not be a risk factor for CRC.
- Analysis of subgroups
Analysis of the subgroups, which included gender, methods of diagnosis of periodontitis, and risk of bias, was performed, as shown in Table 3. The heterogeneity drastically decreased in the subgroup gender in the studies that included only men (I2=0%, p=0.68), only women (I2=0%, p=0.38), and an unclear risk of bias (I2=0%, p=0.36). A decrease in heterogeneity, although moderate, was also found when the method of periodontitis diagnosis was self-reported (I2=59%, p=0.12). In this sense, the analysis showed an increase of 32% in the CRC risk for men with periodontitis (RR=1.32; 95% CI: 1.16-1.50; p<0.00001). The forest plot of the analysis of subgroups may be visualized in Supplemen 3t.
- Publication bias and sensitivity analysis
The Egger test was used, and no publication bias (t=0.40, p=0.7026) was detected, which was confirmed by the Harbor test (t=0.21, p=0.8407) and the Begg test based on the Kendall score (z=1.11, p=0.2655).
The sensitivity analysis is shown in Table 4, in which the study of Momen-Heravi et al. (16) was omitted. An association was found between periodontitis and CRC (RR=1.43; 95%CI:1.00-2.03; p=0.05). Moreover, omitting the study of Kim et al. (14) decreased the heterogeneity to 53%. However, the decision was to maintain these studies due to the statistical power of the sample.
Figure 2. Forest plot of the studies evaluating periodontitis as a risk factor for CRC.
- Quality of evidence
As presented in the SoF Table in Fig. 3, periodontitis was not a risk factor for CRC, with very low certainty of evidence, indicating that the probability of a different result for future studies would be very high. Considering the finding that periodontitis was a risk factor for CRC in the male gender, a second GRADE analysis was performed (Fig. 4) with the studies included in this subgroup, obtaining a moderate certainty of evidence, which suggested a good indication of the probable effect.
Figure 3. SoF table of the eight studies evaluating periodontitis as a risk factor for CRC.
Figure 4. SoF table of the studies evaluating periodontitis as a risk factor for CRC in men.
Discussion
In recent years, studies have suggested a link between periodontitis and the risk of gastrointestinal cancer. The exact biological mechanisms of this association have not yet been fully understood. Some potential pathways have, however, been identified, such as the production of carcinogenic metabolites by specific oral microorganisms and the induction of chronic low-grade systemic inflammation, leading to the release of free radicals and cytokines (21).
Although the overall synthesis showed an RR of 1.32, in the present meta-analysis, the CI crossed the line of no effect, indicating that periodontitis was not a risk factor for CRC. This was in disagreement with the findings of Wang et al. (21) and Li et al. (22), who reported that periodontal disease (PD) increased the risk of CRC by 21% and 44%, respectively. These authors used HR as a measure of effect, and although this can be interpreted as an RR, it can convey different information. The former quantifies the instantaneous relative risk, while RR quantifies the cumulative risk; therefore, these two estimates may differ considerably for the same data (23). It should be noted that the meta-analysis by Wang et al. included one study (24) that did not evaluate CRC directly; instead, it evaluated benign and malignant colorectal tumors and found an association only for the former. Likewise, the review by Li et al. included one study (25) that evaluated mortality. In contrast, both reviews evaluated PD (gingivitis and periodontitis) and not specifically periodontitis, accentuating the discrepancy.
When performing subgroup analysis, a 32% increase in the risk of CRC was found for men with periodontitis, coinciding with the findings reported by Li et al. (22). This is due to the differences in exposure to risk factors such as alcohol and tobacco, dietary patterns and sex hormones. Considering that men diagnosed with CRC had a worse prognosis and a 40% higher mortality rate than women (26), strategies for early detection of periodontitis and colonic lesions with oncogenic potential should be considered for this group.
A limitation to be considered for the present review would be the high heterogeneity, possibly due to the large difference in sample sizes, population characteristics, criteria for classifying exposed/non-exposed participants, and indicators for periodontitis diagnosis, among other factors. Concerning sample sizes, the study by Mai et al. (13) had a sample of only 1337 participants, while Kim et al. (14), Momen-Heravi et al. (16), and Nwizu et al. (17) had samples larger than 50,000 participants, which would contribute to the power of the meta-analysis for detecting real effects (27-29). Similarly, the study by Kim et al. (14) showed a significant difference in the ages of their exposed vs. unexposed groups, with mean ages of 49 [39-60] and 31 [15-46], respectively. This difference in ages could be critical, considering that CRC occurs more frequently in patients over 50 years of age (26,30), and the approximate period in which malignancy findings may occur in the colorectal region is 10 and 15 years, mainly in cases of polyps or in patients with Lynch syndrome (26,31). Moreover, concerning the diagnosis of periodontitis, the majority of studies included in this analysis were based on self-reports validated in previous studies by radiographic bone loss or clinical examination. Only a few used a periodontal index or clinical and/or radiographic diagnosis, the latter being, according to Heitz (32), the standard method for periodontitis diagnosis. While it is true that the use of self-reported data could be susceptible to recall bias or patients could modify their responses to align with concepts they considered socially accepTable, an interesting finding of the present systematic review and meta-analysis was that the self-report subgroup data did not differ from those of the clinical-radiographic diagnosis of periodontitis, which would suggest that self-report could be a reliable method for use in this type of studies.
According to the GRADE assessment of the eight studies included in the meta-analysis, there was great uncertainty in the results, and further studies on the subject would likely provide substantially different results. However, when assessing studies that included men, a moderate certainty of evidence was obtained, indicating that the results probably reflect the situation that occurred in reality. From this aspect, we do recommend that future studies must focus on the presence or predominance of bacterial complexes with evidence of oncogenic properties, such as Fusobacterium nucleatum and Porphyromonas gingivalis (33-35), and show specific results according to gender. Likewise, the periodontal epidemiological index should be homogenized to classify the exposed group and incorporate the evaluation of biomarkers of chronic systemic inflammation.
Conclusions
Periodontitis is not a risk factor for CRC, with very low certainty of evidence and high heterogeneity of the studies included. However, periodontitis is a risk factor in males, with moderate certainty of evidence and without heterogeneity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Asmat-Abanto AS Portocarrero-Reyes A Espejo-Carrera RE Minchón-Medina CA Timaná-Palacios DJ Bibliometric analysis in Scopus of scientific production on the relationship between periodontitis and gastrointestinal cancer (2014 - 2023)Med Oral Patol Oral Cir Bucal 202526269693986408410.4317/medoral.26969 PMC 12019650 · doi ↗ · pubmed ↗
- 2Freiherr Von Seckendorff A Nomenjanahary MS Labreuche J Ollivier V Di Meglio L Dupont S Periodontitis in ischemic stroke: impact of Porphyromonas gingivalis on thrombus composition and ischemic stroke outcomes Res Pract Thromb Haemost 202481023133831815210.1016/j.rpth.2023.102313 PMC 10840352 · doi ↗ · pubmed ↗
- 3Siegel RL Miller KD Wagle NS Jemal A Cancer statistics, 2023 CA Cancer J Clin 20237317483663352510.3322/caac.21763 · doi ↗ · pubmed ↗
- 4Ionescu VA Gheorghe G Bacalbasa N Chiotoroiu AL Diaconu C Colorectal cancer: From risk factors to oncogenesis Medicina (Kaunas)20235916463776376510.3390/medicina 59091646 PMC 10537191 · doi ↗ · pubmed ↗
- 5Klimeck L Heisser T Hoffmeister M Brenner H Colorectal cancer: a health and economic problem Best Pract Res Clin Gastroenterol 2023661018393785270710.1016/j.bpg.2023.101839 · doi ↗ · pubmed ↗
- 6Eskandari-Malayeri F Rezeai M Narimani T Esmaeil N Azizi M Investigating the effect of Fusobacterium nucleatum on the aggressive behavior of cancer-associated fibroblasts in colorectal cancer Discov Oncol 2024152923903044510.1007/s 12672-024-01156-0PMC 11264641 · doi ↗ · pubmed ↗
- 7Zhang C Stampfl-Mattersberger M Ruckser R Sebesta C Kolorektales Karzinom [Colorectal cancer]Wien Med Wochenschr 2023173216203634812910.1007/s 10354-022-00975-6 · doi ↗ · pubmed ↗
- 8Aghili S Rahimi H Hakim LK Karami S Soufdoost RS Oskouei AB Interactions between oral Microbiota and cancers in the aging community: a narrative review Cancer Control 2024311173909298810.1177/10732748241270553 PMC 11378226 · doi ↗ · pubmed ↗