Lumbar Brucella Spondylodiscitis with Extensive Vertebral Abscesses
Shutao Gao, Yukun Hu, Weibin Sheng

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
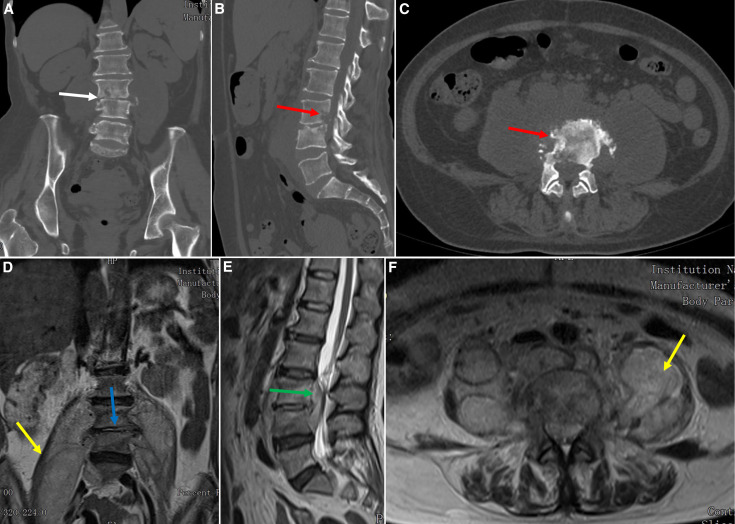 Figure 1
Figure 1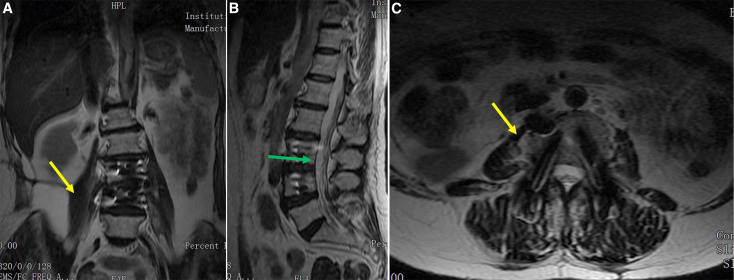 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBrucella: diagnosis, epidemiology, treatment · Bartonella species infections research · Diphtheria, Corynebacterium, and Tetanus
A 59-year-old woman was referred to the outpatient department, complaining of 2 months of low back pain and intermittent fever. She is a shepherd and lives in a village in the Aksu Prefecture of Xinjiang. She had consumed unpasteurized milk a few weeks before the onset of her symptoms. The spinal physical examination showed impaired sensation below the knees, 4/5 strength in the lower extremities, and weak patellar tendon and Achilles tendon reflexes. Laboratory tests indicated a normal white cell count, an increased erythrocyte sedimentation rate (ESR; 50 mm/hour), and an elevated level of C-reactive protein (CRP; 91 mg/L). The interferon-γ release assay (T-spot test) was negative. The Rose–Bengal test result was positive, and the serum agglutination test showed an increased diluted titer of 1:400. Brucella melitensis was obtained from blood cultures. Computed tomography revealed a collapsed L3/4 intervertebral space (Figure 1A) and destruction of the L3 and L4 vertebrae (Figure 1B and C). Magnetic resonance imaging showed L3/4 spondylodiscitis (Figure 1D), a massive psoas abscess extending from L3 to the iliac fossa (Figure 1E), and an L3/4 epidural abscess (Figure 1F).
Given the intolerable back pain, massive psoas and epidural abscesses, and neurologic deficit, surgical treatment was recommended. The patient underwent a one-stage anterior debridement of the abscesses, interbody bone grafting, and internal fixation, followed by posterior debridement and pedicle screw fixation. The patient’s symptoms significantly improved postoperatively. A histopathologic examination and bacterial cultures confirmed the diagnosis of *Brucella *spondylodiscitis (BS). Anti-brucellosis chemotherapy with doxycycline at a dose of 200 mg/day and rifampicin at a dose of 600 mg/day was administered for 6 months. At the 12-month follow-up, the ESR and CRP values were normal. Magnetic resonance imaging showed that the epidural and paraspinal abscesses were cured (Figure 2).
*Brucella *spondylodiscitis most frequently affects the lumbar spine (81.2%),1 but BS with massive psoas and epidural abscesses is a rare condition. Treatments for BS include medication and surgery.2 Surgical indications include progressive deformity, large abscess, neurological deficit, and intolerable pain.3 After surgery, regular anti-brucellosis chemotherapy and close follow-up are recommended to prevent relapses.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liang C Wei W Liang X De E Zheng B, 2019. Spinal brucellosis in Hulunbuir, China, 2011–2016. Infect Drug Resist 12: 1565–1571.31239732 10.2147/IDR.S 202440 PMC 6559255 · doi ↗ · pubmed ↗
- 2Cannella AP Lin JC Liang L Atluri V Gotuzzo E Felgner PL Tsolis RM Vinetz JM, 2012. Serial kinetics of the antibody response against the complete Brucella melitensis OR Feome in focal vertebral brucellosis. J Clin Microbiol 50: 922–926.22219303 10.1128/JCM.05298-11PMC 3295165 · doi ↗ · pubmed ↗
- 3Spernovasilis N Karantanas A Markaki I Konsoula A Ntontis Z Koutserimpas C Alpantaki K, 2024. Brucella spondylitis: Current knowledge and recent advances. J Clin Med 13: 595.38276100 10.3390/jcm 13020595 PMC 10816169 · doi ↗ · pubmed ↗