Clinical Trial Sites and Malaria Incidence Mismatch
Siddharth Brahmbhatt, Mukul Jain, Nilima Kshirsagar

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
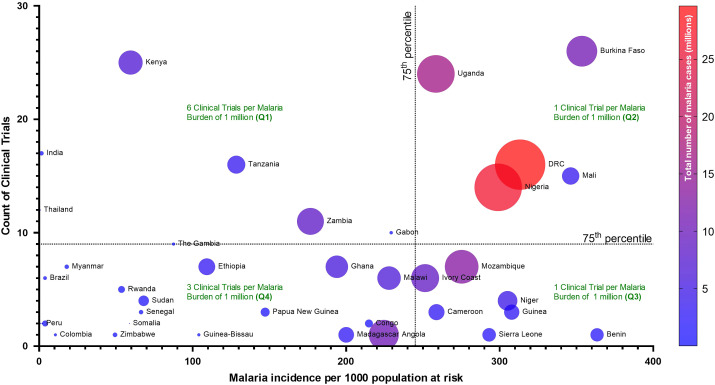 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMalaria Research and Control · Metabolomics and Mass Spectrometry Studies
Dear Editor,
We read, with great interest, the January 2025 Supplemental Issue of the AJTMH (112-1), which highlights the importance of surveillance data for transformative malaria control and elimination.1 It quite correctly emphasizes the need for data-driven decision making. The focus is on high quality and comprehensive surveillance data on vectors and parasites, including molecular and genomic data and use of digital technology. The WHO global malaria program has also advocated subnational tailoring and provides guidance for using granular data. It is recommended that countries must strengthen their surveillance systems to detect early signs of partial artemisinin resistance, which could derail malaria control within a country.
Surveillance of antimalarial drug efficacy is needed for timely detection of, and response to, resistance. However, we wish to highlight gaps in the conduct of clinical trials that lead to challenges in the development of effective regional guidelines and policies, culminating in inefficient malaria-control programs. In a scoping review, Arena et al highlighted how nearly two-thirds of the malaria parasite-positive subjects presented to health facilities were excluded from antimalarial treatment trials, with the reasons for exclusion not reported for nearly one-third of these subjects.2 This gap in data is concerning, as the study populations may not be representative of their communities. In addition, studies have shown that genotypes vary across regions, for both the host and the parasite, thus the efficacy of drugs may vary. Therefore, pragmatic trials with appropriate geographic representation would improve insights into malaria control and elimination.
It is important that clinical studies are done in countries or regions with high malaria burdens. However, we have identified a mismatch between the malaria burden and the frequency of treatment efficacy trials. We obtained data for clinical trials, which are currently recruiting, from the WHO International Clinical Trials Registry Platform and extracted the number of national clinical trials.3 For multi-region trials, each country listed in the record was included. Further, we extracted data on malaria burden, i.e., estimated malaria incidence (per 1,000 population at risk) and total number of malaria cases (presumed + confirmed cases) from the WHO Global Health Observatory. A bubble scatter plot was then generated to assess the correlation between malaria burden and the number of clinical trials (Figure 1).4 The size of the bubble and color were adjusted based on the total estimated number of malaria cases.
This analysis points to a disproportionate intensity of clinical trials in countries that have relatively low malaria burdens. For instance, a subset of relatively low burden countries (Q1) are running an estimated six clinical trials per million malaria cases, while some high burden countries (Q2) are running only one clinical trial per million malaria cases (Figure 1). Further, among high-burden countries, drug efficacy trials remain restricted to only a few countries, in particular, the Democratic Republic of Congo, Uganda, Burkina Faso, Nigeria, and Mali. This mismatch between malaria burden and trial intensity may be limiting the abilities of many high-burden countries to best control malaria.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1YéY Prosnitz D, 2025. Harnessing malaria surveillance data for transformative malaria control and elimination. Am J Trop Med Hyg 112 (Suppl 1): 1–2.10.4269/ajtmh.24-0817 PMC 1172068639787617 · doi ↗ · pubmed ↗
- 2Arena L , 2023. Malaria patient spectrum representation in therapeutic clinical trials of uncomplicated malaria: A scoping review of the literature. Malar J 22: 1–50.36765317 10.1186/s 12936-023-04441-5PMC 9913008 · doi ↗ · pubmed ↗
- 3World Health Organization (WHO), 2025. International Clinical Trials Registry Platform (ICTRP). Available at: https://www.who.int/clinical-trials-registry-platform. Accessed February 3, 2025.
- 4World Health Organization (WHO), 2025. The Global Health Observatory. Available at: https://www.who.int/data/gho. Accessed February 3, 2025.