The Safety of Drug Treatment in Patients with Neuropathic Pain: Data from Ambulatory Care in a Real-Life Setting
Cristina Vocca, Vincenzo Rania, Antonio Siniscalchi, Caterina Palleria, Gianmarco Marcianò, Cecilia Galati, Luca Catarisano, Valentina Mastrangelo, Franco Corasaniti, Francesco Monea, Lucia Muraca, Rita Citraro, Bruno D’Agostino, Luca Gallelli, Giovambattista De Sarro

TL;DR
This study examines adverse drug reactions in patients with neuropathic pain in a real-world clinical setting.
Contribution
The study provides real-life data on drug safety and adverse reactions in neuropathic pain patients.
Findings
18% of patients experienced documented adverse drug reactions.
No significant association was found between adverse reactions and patient characteristics or dosage.
Most patients had multiple comorbidities and used an average of five drugs daily.
Abstract
Introduction: Drug treatment can be related to the development of adverse drug reactions (ADRs). Aim: In this paper, we evaluated ADRs in patients admitted to the Ambulatory of Pain Medicine of the University Hospital Renato Dulbecco in Catanzaro. Methods: We conducted a prospective analysis between 1 February 2021 and 20 July 2023 on patients with neuropathic pain referred to the Ambulatory of Pain Medicine of “Renato Dulbecco” University Hospital in Catanzaro (Calabria, Italy). Patients aged >18 years with clinical signs of neurologic pain and a score upon completing the Douleur Neuropathique en 4 Questions (DN4) questionnaire of ≥4 were included. The association between drugs and ADR or between drugs and drug–drug-interactions (DDIs) was evaluated using Naranjo’s probability scale and Drug Interaction Probability Scale (DIPS), respectively. Results: During the study period, we…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
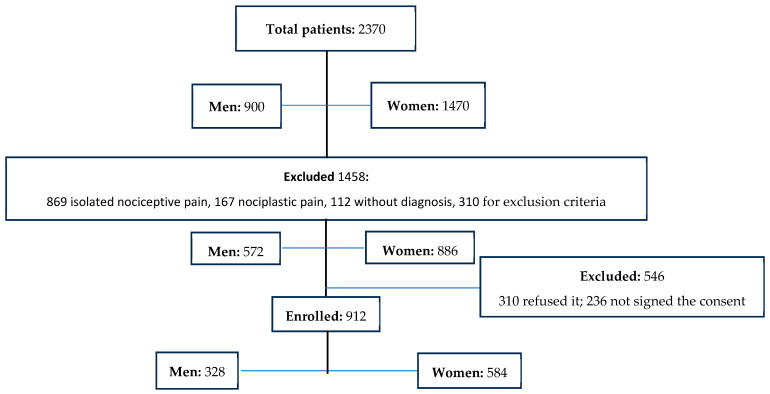 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmacovigilance and Adverse Drug Reactions · Pain Mechanisms and Treatments · Pain Management and Placebo Effect
1. Introduction
The International Association for the Study of Pain (IASP) defines neuropathic pain as pain caused by a lesion or disease of the somatosensory nervous system [1].
In a recent review of international guidelines and recommendations for the pharmacological treatment of neuropathic pain [2], we reported that first-line drugs with a moderate-to-high quality of evidence and strong recommendation are tricyclic antidepressants (TCA, e.g., amitriptyline), antiepileptics (α2δ calcium channel unit blockers, pregabalin, and gabapentin), and serotonin noradrenaline reuptake inhibitors (SNRI: duloxetine and venlafaxine). Capsaicin 8% patches, lidocaine patches, and subcutaneous injections of botulinum toxin type A have weak recommendations and are indicated for peripheral neuropathic pain only [2]. Finally, even if opioids have not been recommended in the treatment of chronic non-cancer pain due to the development of serious adverse drug reactions (ADRs), some authors have suggested that tramadol could be used in the management of neuropathic pain [3,4,5,6,7].
ADRs represent a serious problem during the treatment of patients with pain (i.e., anticholinergic effects for tricyclic antidepressants [8], abuse and misuse of gabapentinoids in patients using opioids [9], and constipation during opioid treatment [10].
Meaadi et al. studied the safety and efficacy of gabapentinoids in the management of neuropathic pain as follows: a systematic review with the meta-analysis of randomized controlled trials.
These reduce patients’ compliance [11,12,13]. To reduce the development of ADRs, which could be also related to the dosage and the long duration of treatment, a non-pharmacological treatment has been suggested. Nutrients are commonly used in patients with pain, e.g., Acetyl-L-carnitine [14,15,16,17,18,19,20], palmitoylethanolamide (PEA) [21,22,23,24,25,26,27], and alpha-lipoic acid [28,29,30,31,32,33,34,35].
However, local techniques, e.g., high-intensity low-frequency-pulsed magnetic fields (diamagnetic therapy) or the administration of oxygen–ozone therapy, could represent an add-on treatment in the management of neuropathic pain [36,37,38,39,40].
The aim of this study was to evaluate, in a real-life ambulatory care study, both the development and the characteristics of ADRs in patients with neuropathic pain.
2. Materials and Methods
2.1. Study Design
We conducted a prospective study between 1 February 2021 and 20 July 2023 on patients with neuropathic pain who were referred to the Ambulatory of Pain Medicine of “Renato Dulbecco” University Hospital in Catanzaro (Calabria, Italy). The study, approved by the Ethics Committee (Calabria Centro: number 22/2021), was carried out according to the Good Clinical Practice guidelines and under the ethical principles of the Declaration of Helsinki. Before the beginning of this study, all participants signed a written informed consent form.
2.2. Inclusion and Exclusion Criteria
We enrolled patients aged >18 years with clinical signs of neurologic pain and a score from the Douleur Neuropathique en 4 Questions (DN4) questionnaire of ≥4. Patients with less than two clinical accesses to the ambulatory were excluded.
Exclusion criteria included current patients with nociceptive pain or nociplastic pain, patients with Alzheimer’s disease, and patients with active cancer. Moreover, patients who did not sign the informed consent were excluded.
2.3. Protocol
Consecutive patients were referred to the Ambulatory of Pain of Medicine of the University of Catanzaro for chronic pain, and were screened for neuropathic pain using both clinical tests and the DN4 questionnaire. In agreement with inclusion and exclusion criteria, patients were enrolled in this study and signed informed consent forms. During the admission, demographic data, comorbidity, polytherapy, the drug used and dosage, previous ADRs, and the intensity of pain (using the Numerical rating scale, NRS) were collected. Each patient was asked if he or she could evaluate his or her level of pain on a scale from 0 to 10, where 0 equaled an absence of pain and 10 indicated the maximum level.
The DN4 is a clinician-administered, neuropathic pain diagnostic questionnaire consisting of ten items grouped in four sections evaluating the quality of pain (burning, painful cold, electric shocks) and its association with abnormal sensations (tingling, pins and needles, numbness, itching). A score ≥ 4 was suggestive of neuropathic pain.
The ADRs correlated to the treatment were evaluated using the Naranjo probability scale, which is in agreement with our previous studies [41,42].
The Naranjo probability scale is a validated scale used to classify the probability that an adverse event is related to drug therapy based on a list of weighted questions, which examine factors such as the temporal association of drug administration and event occurrence, alternative causes for the event, drug levels, dose–response relationships and previous patient experience with the medication. A score of 1–4 suggested the possible correlation between the drug and ADR, a score of 5–8 represented a probable correlation, and a score >8 indicated a certain correlation [42,43,44].
Collected data were then stored in an Access database with security code protection.
2.4. Endpoints
The primary endpoint was the development of ADRs during the treatment of neuropathic pain. The secondary endpoint was the correlation between ADRs and age, comorbidity, and polytherapy in men and women with neuropathic pain.
2.5. Statistical Analyses
Data are presented as the mean ± standard deviation (SD). For categorical parameters, the chi-square test was used. Student’s t-test and the Kruskal–Wallis test were used for non-parametric variables. The Shapiro–Wilk test was used to evaluate the normality of distribution. Pearson’s test and Sperman’s test were used for the correlation study. Logistic regression was performed to evaluate the influence of different factors on pain levels. p-values < 0.05 were considered statistically significant. Statistical analysis was performed using SPSS 22.0 (International Business Machines Corporation, Armonk, NY, USA).
3. Results
3.1. Demographic and Clinical Characteristics
During the study, we analyzed 2370 patients (men: 900, age 59.7 ± 11.6; women 1470, mean age 60.3 ± 11.9). After the evaluation of inclusion and exclusion criteria evaluation, 912 patients (38.5%, mean age 61.4 ± 13; 328 men and 584 women, mean age 60.6 ± 13.4 and 61.8 ± 12.9) with neuropathic pain were enrolled (Figure 1) (Table 1).
Statistical evaluation failed to show a significant difference between men and women with respect to age, instruction level, and smoking history (p > 0.05). Evaluating the patients stratified by age, we documented that 133 men (59.4%) and 251 women (57%) were enrolled in the group 18–64 years, while 195 men (40.6%) and 333 women (43%) were in the group > 65 years. Statistical evaluation did not document a significant difference between these groups for age, BMI, DN-4, NRS, degree, or smokers (Table 2).
Of the 912 enrolled patients, 886 patients (97.2%, mean age 61.7 ± 12.9) had at least one comorbidity (men 313, mean age 61.4 ± 13; women 573, mean age 61.9 ± 13); the most common were diabetes and osteoarthritis (Table 2). Psychiatric, rheumatologic, and orthopedic diseases were significantly more common in women (Table 2).
Concerning the comorbidity, we documented that diabetes was the most common comorbidity in the group 18–64 years (men 55.3%, women 55.4%, p > 0.05) and in elderly men (73.1%), while cardiovascular diseases and osteoarthritis were the most common comorbidities in elderly women (83.7%) (Table 3).
Moreover, we documented a statistically significant difference between men and women for the presence of urological diseases (elderly men’s group, p < 0.01), rheumatological diseases (women’s groups, p < 0.01), and psychiatric diseases (elderly women’s group, p < 0.01) (Table 2). All enrolled patients of both sexes and in both groups used drugs for pain treatment (Table 2 and Table 3).
3.2. ADRs
During the study, 164 patients (18%), including 67 men (40.7%) and 97 women (59.4%) developed ADRs (Table 4).
The statistical evaluation did not show any significant difference between men and women regarding age, BMI, DN4, degree, or if they were smokers (Table 4). Evaluating the comorbidities, we documented that women had a significant increase in neurological and rheumatologic diseases compared to men (p < 0.05) (Table 4).
Moreover, considering the gender differences between the patients with and without ADRs, we did not record any statistical difference between the patients who developed ADRs and those who did not (Table 5).
When we considered the difference between men and women with and without ADRs, we documented that smoking was most common in patients with ADRs compared to patients without ADRs (p < 0.01), without differences between men and women (Table 6). Considering the comorbidity, we recorded that rheumatological diseases and renal diseases were common in men with ADRs compared to men without (p < 0.01), while urological diseases were common in women with ADRs compared to women without (Table 7).
Considering the drugs involved in the development of ADRs, even if we documented a probable association between drugs and ADRs (Naranjo score: 6), we failed to record a significant correlation between the drug used and their dosages (Table 8).
We did not find any significant difference between the drugs used in patients with ADRs and patients without (Table 9).
The evaluation of the treatments involved in ADRs failed to identify a difference between men and women (p = 0.115). Moreover. the use of Pearson’s test failed to show a correlation between age, sex, degree, BMI, drug dosage, and ADRs (Table 10). The same result was recorded using multiple logistic regression analysis. The evaluation of ADRs documented that 1 patient (a man, smoker, 68-year-old, BMI 28.4) developed stypsis, confusion, and somnolence during polytherapy (Table 11). Similarly, six women developed more than one ADR during polytherapy.
Finally, the Pearson test did not show a correlation between polytherapy and ADRs (r: 0.02358).
4. Discussion
In this prospective study performed in the ambulatory care real-life setting, we evaluated both the types and the characteristics of ADRs to pharmacological and non-pharmacological treatments used to treat neuropathic pain.
Neuropathic pain is a chronic manifestation in which several clinical conditions (e.g., diabetes, inflammation, viral infections, injury) are able to induce a neuronal lesion with continuous neural activation.
Therefore, drugs able to modulate neural activation (e.g., channel blockers and modulators of neurotransmitter pathways) are commonly used [2].
In our study, we enrolled consecutive patients who were referred to the Pain Medicine Ambulatory of our University Hospital of General Practitioners for neuropathic pain. History and clinical evaluation documented that these patients (men and women) had suffered from low back pain or cervicobrachial pain for several years, and all these patients received treatment, commonly opioids since international guidelines suggest that opioids are not the first line of treatment. This could be related to the idea that drugs must be used for pain intensity management more than for the type of pain.
Moreover, a clinical evaluation documented that 92.3% of enrolled men and 100% of enrolled women presented a comorbidity, commonly in both sexes, diabetes, and osteoarthritis.
This agrees with data from the literature reporting that osteoarthritis and diabetes mellitus are associated in the same patients [45,46]. Louati et al. [47], in a systemic review, documented the high prevalence of osteoarthritis among patients with diabetes mellitus (29.5 ± 1.2%) and of diabetes mellitus among patients with osteoarthritis (14.4 ± 0.1%). Moreover, in our study, we recorded a high prevalence of urological diseases in men and rheumatological diseases in women, as also reported in data from the literature [48].
The presence of comorbidity or polytherapy must be considered in patients with pain because both diabetes and rheumatological diseases can impair pain levels. Similarly, the presence of urological or renal diseases can reduce renal activity; therefore, in these patients, the treatment must appropriate in order to reduce the risk of ADRs [49,50,51,52,53].
Both ADRs and inappropriate therapy represent a major concern in clinical practice because they can reduce adherence to the treatment [54,55,56,57,58,59,60,61], increasing health costs [49,62,63,64,65].
In this study, we documented that 18% of enrolled patients developed ADRs without a difference with respect to sex and without any correlation with respect to BMI, age, study, or other demographic characteristics. Moreover, we failed to report a correlation between ADRs and the DN4 score, and in all patients, the Naranjo score documented a probable association between drugs and ADRs.
The most common drugs involved in ADRs were opioids, and this is related to the low safety of these drugs. Moreover, it is important to remember that opioids are no longer recommended for the treatment of most patients with chronic pain. In fact, Nury et al. [66], reviewing data from the literature suggested that long-term opioid therapy (≥6 months) in chronic non-cancer pain may not be superior to nonopioids in improving pain or disability or pain-related functions but seems to be associated with more adverse events, opioid abuse or dependence, and possibly an increase in all-cause mortality.
We documented that opioid use induced the development of stypsis and mild CNS effects (e.g., somnolence and confusion), as described in drug labels [67,68,69,70]. Similar CNS effects were recorded during the treatment with pregabalin and antidepressants [71,72].
Pregabalin and duloxetine are commonly used in the management of neuropathic pain and represent the first line of treatment [2]. Their effects in the management of neuropathic pain can be related to the block of neural depolarization (pregabalin) and to the potentiation of the inhibitory pathway (duloxetine). These mechanisms induce the development of central side effects that could be reduced by starting with a low dosage and not using drugs that are able to induce CNS inhibition. In our study, we recorded that pregabalin was used with a high first dosage (125 or 150 mg daily) even if the total dosage was similar to the patients who did not develop ADRs. Duloxetine was co-administered with opioids that can induce CNS inhibition.
During this study, we reported fewer side effects in patients using nutraceuticals and oxygen–ozone therapy. These produce a very interesting result for physicians, especially considering the great efficacy of oxygen–ozone therapy [73,74,75,76,77,78].
Moreover, Magalhaes et al. [79], analyzing data from the literature in patients with low back pain secondary to disc herniation treated with oxygen–ozone therapy, documented both the safety and the efficacy of oxygen–ozone with evidence of the level II-3 for ozone therapy applied intradiscally and II-1 for ozone therapy applied paravertebrally (recommendation: 1C for ozone therapy applied intradiscally; 1B for ozone applied at the paravertebral muscles).
Diamagnetic therapy and acetyl-L-carnitine had no side effects, showing an excellent safety profile, according to previous experience and the label [36,80].
Our study has several limitations. Firstly, the number of patients is relatively small to draw definitive conclusions, and the number of women is high in comparison to men, even if the real-life setting is characterized by a high number of women coming to our ambulatory in comparison to men. Data were obtained in a clinical room of pain medicine where specialists in clinical pharmacology performed diagnosis and treatment, and this probably reduced the development of ADRs, also related to the comorbidity, polytherapy, level of instructions, and smoke. We used diamagnetic therapy, which is not a pharmacological treatment, but we reported it because we use it in some patients as an add-on therapy to reduce the dosage of drug treatment.
In conclusion, we documented that drugs used in the management of neuropathic pain are usually safe and, if prescribed appropriately, do not induce the development of severe ADRs or drug interactions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1IASP International Association for the Study of Pain—Terminology Available online: https://www.iasp-pain.org/resources/terminology/(accessed on 18 June 2023)
- 2MarcianòG. Vocca C. Evangelista M. Palleria C. Muraca L. Galati C. Monea F. Sportiello L. De Sarro G. Capuano A. The Pharmacological Treatment of Chronic Pain: From Guidelines to Daily Clinical Practice Pharmaceutics 202315116510.3390/pharmaceutics 1504116537111650 PMC 10144480 · doi ↗ · pubmed ↗
- 3Attal N. Bouhassira D. Translational neuropathic pain research Pain 2019160 S 23S 2810.1097/j.pain.000000000000152231008846 · doi ↗ · pubmed ↗
- 4Kawai S. Hasegawa J. Ito H. Fukuuchi Y. Nakano H. Ohtani H. Sasaki K. Adachi T. Efficacy and safety of twice-daily tramadol hydrochloride bilayer sustained-release tablets with an immediate release component for postherpetic neuralgia: Results of a Phase III, randomized, double-blind, placebo-controlled, treatment-withdrawal study Pain Pract.20232327728910.1111/papr.1319036478501 · doi ↗ · pubmed ↗
- 5Duehmke R.M. Derry S. Wiffen P.J. Bell R.F. Aldington D. Moore R.A. Tramadol for neuropathic pain in adults Cochrane Database Syst. Rev.2017201714410.1002/14651858.CD 003726.pub 4PMC 648158028616956 · doi ↗ · pubmed ↗
- 6Subedi M. Bajaj S. Kumar M.S. YCM. An overview of tramadol and its usage in pain management and future perspective Biomed. Pharmacother.201911144345110.1016/j.biopha.2018.12.08530594783 · doi ↗ · pubmed ↗
- 7Bravo L. Mico J.A. Berrocoso E. Discovery and development of tramadol for the treatment of pain Expert. Opin. Drug Discov.2017121281129110.1080/17460441.2017.137769728920461 · doi ↗ · pubmed ↗
- 8Brueckle M.S. Thomas E.T. Seide S.E. Pilz M. Gonzalez-Gonzalez A.I. Dinh T.S. Gerlach F.M. Harder S. Glasziou P.P. Muth C. Amitriptyline’s anticholinergic adverse drug reactions—A systematic multiple-indication review and meta-analysis P Lo S ONE 202318 e 028416810.1371/journal.pone.028416837018325 PMC 10075391 · doi ↗ · pubmed ↗