Treatment outcomes of symptomatic internal iliac artery aneurysms
Lily P Wu, Jessica Dei-Asamoa, Olutobi A Sanuade

TL;DR
This case report details successful surgical outcomes for three patients with rare internal iliac artery aneurysms in Ghana.
Contribution
The study provides new insights into surgical treatment outcomes for IIIAA in a Ghanaian context.
Findings
All three patients had uneventful post-operative recoveries and improved mobility.
Post-operative CT scans showed no complications in any of the patients.
Open surgical repair was effective for treating IIIAA in this cohort.
Abstract
Isolated internal iliac artery aneurysm (IIIAA) is a rare condition, with limited information available about its symptoms and surgical treatment outcomes, particularly in Ghana. This case report presents the 4-year surgical treatment outcomes of three patients (aged 42, 58, and 22 years) with IIIAA, each exhibiting different clinical presentations. All patients experienced pelvic pain and difficulty walking but had uneventful post-operative recoveries. They made significant progress with physiotherapy and were able to mobilise with a Zimmer frame before discharge. Currently, all three patients are mobilising unaided, and post-operative Computed Tomography (CT) scans show no complications. This report highlights the importance of early diagnosis to minimise complications and improve the prognosis for IIIAA, which often presents asymptomatically and can manifest with a wide range of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
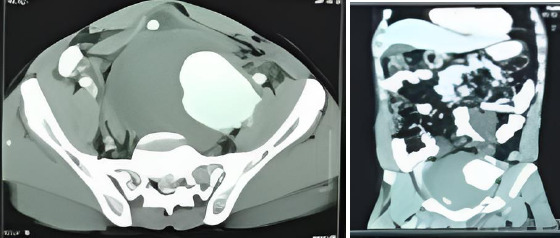 Figure 1a
Figure 1a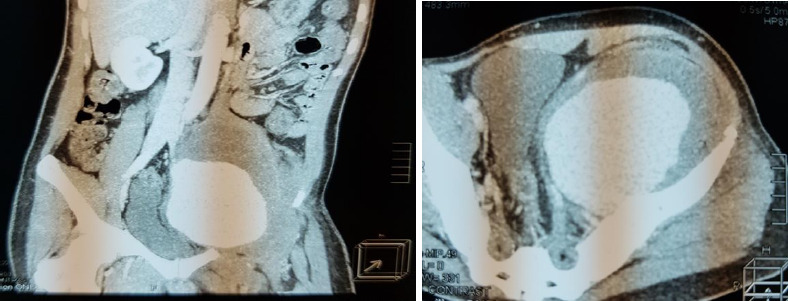 Figure 1b
Figure 1b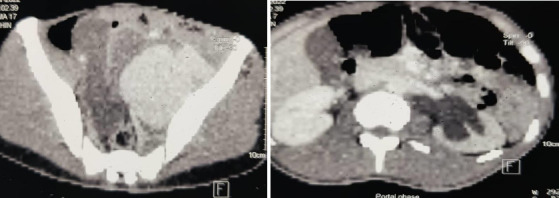 Figure 1c
Figure 1c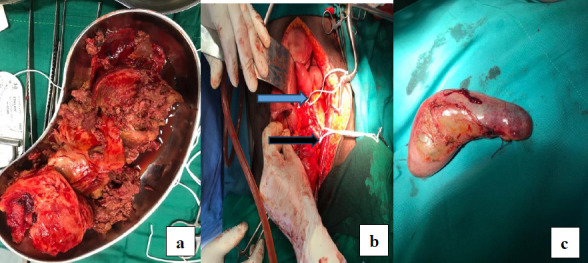 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4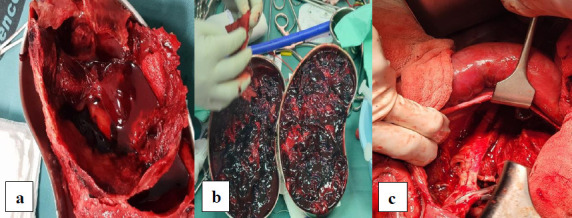 Figure 5
Figure 5 Figure 6
Figure 6| Tests | Case 1 Findings | Case 2 Findings | Case 3 Findings |
|---|---|---|---|
|
| HB 11.4 g/dL (10-14), WBC 10.46 x 10^9/L (2.50-8.50), PLT 338 x 10^9/L (150-450) | HB 10.8 g/dL (10-14), WBC 12.07 x 10^9/L (2.50-8.50), PLT 286 x 10^9/L (150-450) | HB 7.9 g/dL (10-14), WBC 13.86 x 10^9/L (2.50-8.50), PLT 438 x 10^9/L (150-450) |
|
| Cr 155.0 µmol/L (71-133), Urea 8.2 mmol/L (2-7), Na 138 mmol/L (135-150), K 5.5 mmol/L (3.5-5.5) | Cr 105.0 µmol/L (71-133), Urea 6.2 mmol/L (2-7), Na 138 mmol/L (135-150), K 5.0 mmol/L (3.5-5.5) | Cr 115.0 µmol/L (71-133), Urea 11.2 mmol/L (2-7), Na 122 mmol/L (135-150), K 5.5 mmol/L (3.5-5.5) |
|
| Negative | Negative | Negative |
|
| Negative | Negative | Negative |
|
| Negative | Negative | Negative |
|
| No bacteria growth | No bacteria growth | No bacteria growth |
|
| Normal | Normal | Normal |
|
| Normal | Normal | Normal |
|
| Normal | Normal | Normal |
|
| 8.9 cm left IIAA, severe hydronephrosis, hydroureter, non-functional left kidney | 7.8 cm left IIAA, left hydronephrosis, hydroureter, functional left kidney | 8 cm left IIAA, ilio-femoral DVT |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic aneurysm repair treatments · Vascular Procedures and Complications · Vascular anomalies and interventions
Introduction
Most iliac artery aneurysms are associated with abdominal aortic aneurysms (AAA). Up to 10-15% of AAA co-exist with iliac artery aneurysm.1 Iliac artery aneurysm (IAA) is a dilatation of the common, internal, or external iliac arteries or various combinations of them, without the involvement of the infra-renal abdominal aorta. Isolated internal iliac artery aneurysms (IIIAA) are uncommon, making up 0.3-0.5% of all intra-abdominal aneurysms. IIIAA is defined as focal dilatation of the internal artery alone with a threshold for surgical treatment set at 3.5 cm.1,2
IIIAA is a disease of the elderly (aged 65-75 years) with a male-to-female ratio of between 5-16:1.2,3 Risk factors and aetiologies associated with Isolated Internal Iliac artery aneurysms include infection (viral and bacterial), trauma and arterial wall disorders due to connective tissue diseases like Marfan and Ehlers-Danlos syndrome etc. However, the predominant aetiological factor is degeneration, hence its predilection for the aged. Some organisms responsible for the infective causes of IIIAA are Salmonella spp., Staphylococcus aureus, Escherichia coli and Tuberculosis.4 Infective causes of IIIAA is most often found in relatively young people below the age of 50 years.
Symptom manifestation of IIIAA is usually late and include pelvic pain from nerve root compression or pressure on surrounding structures. Other symptoms include pyelonephritis from urosepsis secondary to ureteric obstruction which can also manifest at flank pain. IIIAA is an uncommon cause of deep vein thrombosis (DVT).5,6 We report the surgical treatment outcomes of three cases of IIIAA, all male patients presenting with different complications of IIIAA. Written informed consent was obtained from the patients for publication of this case report and accompanying images.
Case Presentation
Case 1
A 42-year-old tailor presented with severe left hydronephrosis, hydroureter, and a non-functional left kidney. A CT angiogram revealed a large fusiform left internal iliac aneurysm (8.9 cm). The patient, a nonsmoker with no history of hypertension, hypercholesterolemia, or connective tissue disease, experienced severe pelvic pain and was unable to walk for two months prior to his clinic visit. The laboratory and radiological examinations performed are shown in Table 1.
On examination, he appeared acutely ill with a Body Mass Index (BMI) of 24.1 kg/m^2^. His vital signs included a blood pressure of 128/78 mmHg, a pulse rate of 98 bpm, and a temperature of 36.8°C. His left lower limb was held in flexion and external rotation at the hip, appearing larger than the right limb. Measurements showed a mid-thigh circumference of 45 cm, calf circumference of 32 cm, and ankle circumference of 22 cm on the left, compared to 40 cm, 30 cm, and 20.5 cm on the right. Peripheral pulses were present in both lower limbs but were weaker on the left. The left lower limb was tender with intact sensation but reduced motor function (3/5).
The patient was admitted and treated with intravenous (IV) antibiotics (amoxicillin clavulanic acid and ciprofloxacin) for four days pre-operatively and continued post-operatively for two weeks. Pain management included IV paracetamol and intramuscular pethidine. Pre-operative work-up and imaging were conducted (Figure 1a). Definitive surgery involved an open primary repair with a total nephrectomy due to the non-functional kidney (Figure 2).
Pre-operative CT angiogram of Case 1
Pre-operative CT angiogram of patient 2
Pre-operative CT angiogram of patient 3
intra-operative pictures of patient 1 showing laminar thrombus in a kidney dish (a), aneurysmal sac (b) with a proximal sling on CIA (blue arrow) and distal sling on EIA (black arrow) and a non-functional left kidney post nephrectomy(c) sample
The peritoneal cavity was explored through a midline incision, and the aneurysm was identified. The left common iliac (CIA) and external iliac arteries (EIA) were mobilised and clamped after administering IV heparin. The aneurysm was opened, the thrombus was evacuated, and the aneurysmal sac was excised. The left internal iliac artery (IIA) stump was ligated, and the distal branches were sutured. The total operating time was three hours, with an estimated blood loss of one litre. The patient received two units of whole blood and two units of fresh frozen plasma intra-operatively.
Postoperatively, the patient had an uneventful recovery, with an 18-day hospital stay. On postoperative day eight, antibiotics were switched to oral, and the Pneumovac was removed on day ten. He made good progress with physiotherapy, mobilising with a Zimmer frame before discharge. His haemoglobin was 10.1 g/dL at discharge, with normal full blood count and renal function.
Follow-up at two weeks and three months post-discharge showed he was doing well. Now, three years post-operative, he mobilises unaided, and post-operative CT scans show no complications.
Case 2
A 58-year-old male from Liberia was referred to Ghana to see a Vascular Surgeon due to difficulty walking, pelvic pain, and a CT angiogram finding of a 7.8 cm fusiform left internal iliac aneurysm with left hydronephrosis and hydroureter. He was a known hypertensive but well-controlled on anti-hypertensive medication.
On examination, he appeared acutely ill with a BMI of 23.8 kg/m^2^. His blood pressure was 145/84 mmHg, pulse rate 86 bpm, and temperature 37.2°C. His left lower limb was held in flexion and external rotation at the hip, appearing larger than the right limb. Measurements showed a mid-thigh circumference of 47.5 cm, calf circumference of 34 cm, and ankle circumference of 22.5 cm on the left, compared to 41.5 cm, 31 cm, and 21.5 cm on the right. Peripheral pulses were present in both lower limbs but were weaker on the left. The left lower limb was tender with intact sensation but reduced motor function (2/5).
The patient was admitted and treated with IV antibiotics (amoxicillin clavulanic acid and ciprofloxacin) for four days pre-operatively and continued post-operatively for one week. Pain management included IV paracetamol and intramuscular pethidine. Pre-operative work-up and imaging were conducted (Figure 1b). He underwent an endovascular repair with a hybrid operation involving plugging of the right common iliac artery, insertion of an aorto-uni-iliac stent graft on the left, and a left-to-right fem-fem crossover with a reinforced 8mm PTFE graft (Figure 3).
intra-operative on table angiogram of patient 2 showing a large left IIA, aorto-uni-iliac stent, right CIA plug and a fem-fem crossover
Post-operatively, the patient had an uneventful recovery, with a hospital stay of 15 days. Antibiotics were switched to oral on the first postoperative day. He made good progress with physiotherapy, mobilising with a Zimmer frame before discharge. His haemoglobin was 10.7 g/dL at discharge, with normal full blood count and renal function. Follow-up at two weeks and three months post-discharge showed he was doing well. Now, two years postoperative, he mobilizes unaided, and post-operative CT scans show no complications. He is currently on surveillance with serial CTA every six months and reviewed electronically via Zoom or WhatsApp.
Case 3
A 22-year-old male was referred to the Vascular Unit with a diagnosis of left deep vein thrombosis (DVT), confirmed by a venous duplex scan. Despite being treated with anticoagulation (IV unfractionated heparin) for two weeks at another hospital, his condition worsened, leading to increased pain, swelling, and immobility in his left leg. He had no known risk factors for DVT, no family history, and was a non-smoker. A CT angiogram revealed an 8cm fusiform aneurysm in the left internal iliac artery, compressing the left external iliac vein and causing ilio-femoral DVT (Figure 1c).
On presentation, he was acutely ill, with a body mass index (BMI) of 23.2kg/m^2^, a blood pressure of 134/92mmHg, and a pulse rate of 115 beats per minute. His left lower limb was significantly larger than the right. On the left lower limb, his mid-thigh circumference was 48cm, his calf circumference was 35cm and his ankle circumference was 23.5cm compared to 39cm, 30cm and 20cm respectively on the right. The left lower limb was tender; sensation was intact but motor function was reduced (2/5) (Figure 4).
A picture of patient 3 pre-operative showing limb posture and circumference discrepancy
He was admitted and treated with antibiotics (IV amoxicillin clavulanic acid and IV ciprofloxacin) for four days before surgery and one week post-operatively. The pain was managed with IV paracetamol and intramuscular pethidine. Pre-operative investigations included a transfemoral insertion of an IVC filter to prevent embolisation.
The surgical procedure involved a midline laparotomy to access the aneurysm, which was excised after clamping the common iliac and external iliac arteries. The defect in the common iliac artery was repaired with 5.0 Prolene, and an iatrogenic injury to the external iliac artery was also repaired with 6.0 Prolene (Figure 5).
Intra-operative pictures of Case 3 showing laminar thrombus (a), aneurysmal sac in a kidney dish (b) and the remaining cavity in the left iliac fossa (c)
The peritoneal cavity was lavaged with warm saline, and a Pneumovac was inserted for drainage. The surgery lasted six hours, with an estimated blood loss of 3 litres. The patient received blood and plasma transfusions intra-operatively.
Post-operatively, the patient recovered well. He was switched from IV to oral antibiotics and made significant progress with physiotherapy, mobisliing with a Zimmer frame before discharge. His hospital stay lasted 20 days, and by discharge, his haemoglobin level was 10.4g/dl, with normal blood counts and renal function. At follow-up visits two weeks and three months later, he was doing well. Three years post-operation, he is fully mobile without assistance, and post-operative CT scans show no complications or adverse events (Figure 6).
Postoperative computerized tomography of patient 3 showing successful aneurysmal excision and patent left iliac arteries. (NB: Arrow points to left internal iliac artery stump)
Discussion
This study is the first in Ghana to report symptoms and surgical outcomes of isolated iliac artery aneurysms (IIIAAs). We examined three male patients, aged 22–58, who presented with complications of IIIAA. Our findings emphasize the importance of timely diagnosis and prompt surgical intervention for IIAA complicated by progressive deep vein thrombosis (DVT). This study also aims to raise awareness among health professionals about the potential for positive outcomes in IIAA cases in Ghana if proper guidelines are followed.
Even though evidence shows that IIAA is a relatively uncommon vascular disease, especially among young people,7 all the patients in this study were below 65 years old. This suggests a possibility of an earlier onset of IIIAA in Ghana. Previous studies have noted that IIIAA is more prevalent in males,7 which aligns with our study, but further research is needed to explore why this condition disproportionately affects men.
Clinically, all three patients presented with pelvic pain and difficulty walking, symptoms commonly associated with IIAA from nerve compression and pressure on surrounding structures.8 Other clinical presentations included left internal iliac aneurysm, left leg DVT, and left hydronephrosis and hydroureter. While urinary tract infections (UTIs) are a known complication of IIIAA, none of the patients in this study had UTIs. However, DVT, as seen in patient 3, has been previously documented as a complication.9
All patients had larger left lower limbs with reduced motor function, consistent with research showing that over 61% of IIIAA cases affect the left side.7,10 None had significant atherosclerosis risk factors, highlighting the atypical nature of these cases. As the internal iliac artery is deep in the pelvis, previous research showed that most IIIAAs show no symptoms until they become large or rupture.2 This shows the need for early diagnosis and effective management strategies to prevent severe outcomes.
All three patients underwent open surgical repair, which is one of the standard treatment options for IIIAA alongside endovascular repair and hybrid techniques.7 Despite the high mortality risk associated with untreated IIIAA, 8,9 all patients in this study had favourable outcomes. They were discharged after an average 14-day hospital stay, fully mobilised, and had no post-operative complications, as confirmed by CT scans. These results underscore the effectiveness of open surgical repair for managing IIIAA in Ghana.
Conclusion
IIIAA is a low-incidence disease that is often asymptomatic and can present with a wide range of clinical findings. Treatment with open surgical repair is effective in getting positive outcomes in asymptomatic patients. Since patients usually present with no symptoms, the need for early diagnosis to minimize complications and worse prognosis is important. Also, further research is needed to explore the reasons for the higher prevalence of IIAAs among men as well as relatively younger people in Ghana.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Perini P Mariani E Fanelli M Ucci A Rossi G Massoni CB Freyrie A Surgical and Endovascular Management of Isolated Internal Iliac Artery aneurysms: A Systematic Review and Meta-Analysis Vasc Endovasc Surg 202155325426410.1177/153857442098181233353481 · doi ↗ · pubmed ↗
- 2Wanhainen A Verzini F Van Herzeele I Editor's choice—European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms Eur J Vasc Endovasc Surg 20195718933052814210.1016/j.ejvs.2018.09.020 · doi ↗ · pubmed ↗
- 3Richardson JW Greenfield LJ Natural history and management of iliac aneurysms J Vasc Surg 198882165 e 1713294450 · pubmed ↗
- 4Dix FP Titi M Al-Khaffaf H The isolated internal iliac Artery Aneurysm: A review. 2005 Eur J Vasc Endovasc Surg 2005301119112910.1016/j.ejvs.2005.04.03515939637 · doi ↗ · pubmed ↗
- 5Atsuta Y Inaba M Goh K Azuma N Isolated iliac artery aneurysm caused by fibromuscular dysplasia: report of a case Surg Today 2003336396411288410710.1007/s 00595-003-2551-1 · doi ↗ · pubmed ↗
- 6Kanazawa ST Yamazaki Y Aoki E Sakurai Y Mycotic aneurysm of the internal iliac artery caused by Klebsiella pneumoniae VASA 1996251841878659223 · pubmed ↗
- 7Sandhu RS Pipinos II Isolated iliac artery aneurysms Semin Vasc Surg 20051842092151636057810.1053/j.semvascsurg.2005.09.007 · doi ↗ · pubmed ↗
- 8Fernández MJN Castro AMN Karla Elisabeth Moncayo León KEM Deep vein thrombosis in lower extremities of an exceptional cause: Isolated internal iliac artery aneurysm and ilio-iliac arteriovenous fistula Vasc Med 20202521941953219562410.1177/1358863 X 20907689 · doi ↗ · pubmed ↗