Nasal carriage rate and multiple antimicrobial resistance indices of Staphylococcus aureus among healthcare students at the Ahmadu Bello University, Nigeria
Sumayya Abdullahi, Idris N. Abdullahi, Hafeez A. Adekola, Nicholas Baamlong, Amos Dangana, Yahaya Usman, Abdurrahman E. Ahmad, Sumaiya Salisu, Mukhtar M. Abdulaziz

TL;DR
This study found high rates of drug-resistant Staphylococcus aureus in healthcare students in Nigeria, highlighting potential public health risks.
Contribution
First study in Africa to assess multiple antimicrobial resistance indices of nasal S. aureus in healthcare students and categorize subgroup variations.
Findings
31.5% of students carried S. aureus, with 23.5% being MRSA.
Medical and pharmacy students had significantly higher MDR-S. aureus carriage.
Tetracycline and ciprofloxacin showed the highest resistance among isolates.
Abstract
Healthcare students could harbour multidrug-resistant (MDR) and methicillin-resistant Staphylococcus aureus (MRSA). There is a need to understand the extent and factors associated with nasal carriage of these strains. This study determined the frequency and risk of nasal S. aureus, and multiple antimicrobial resistance indices among students at Ahmadu Bello University, Zaria, Nigeria. This comparative cross-sectional study collected nasal samples from 02 January 2024 to 31 July 2024 from healthcare students at Ahmadu Bello University, Nigeria, which were processed for S. aureus identification. Antimicrobial resistance phenotype was determined by the disk diffusion method. Structured questionnaires were used to collect participants’ sociodemographic and risk factor data. A total of 251 students participated, including 126 (50.2%) men and 125 (49.8%) women (aged 17–44 years). The nasal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
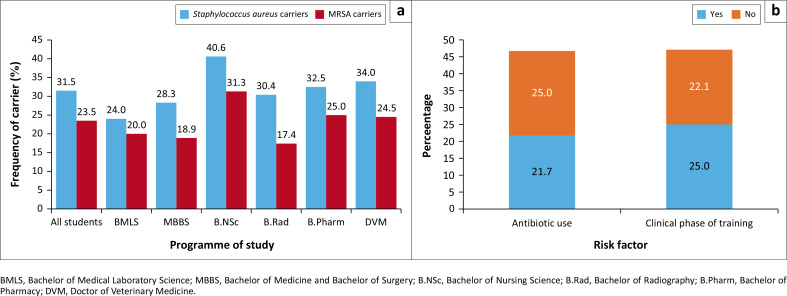 FIGURE 1
FIGURE 1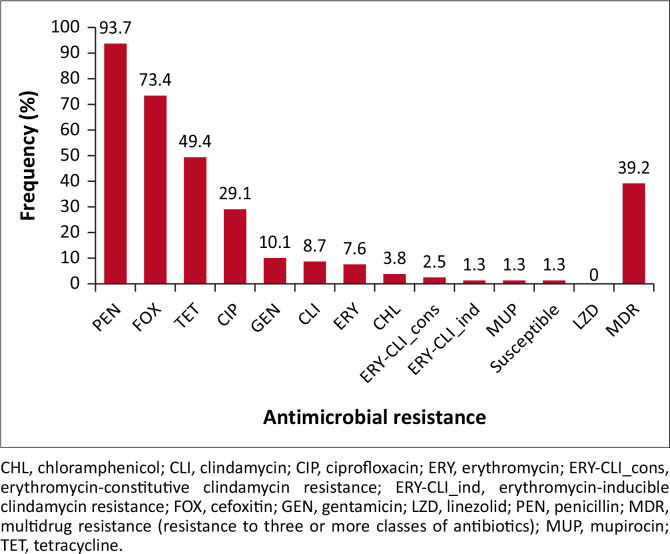 FIGURE 2
FIGURE 2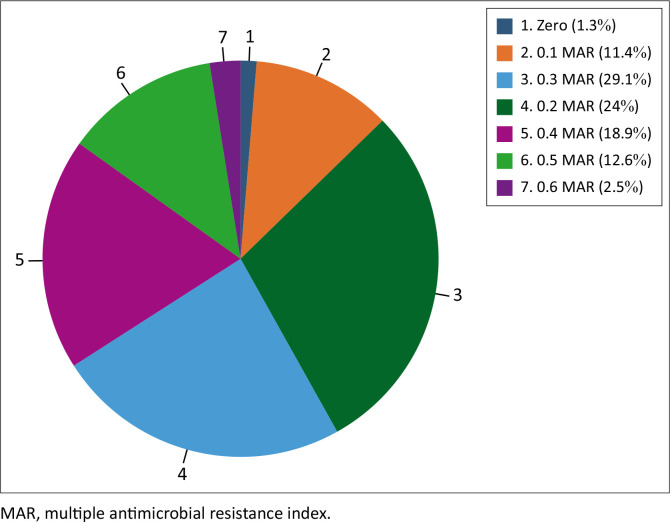 FIGURE 3
FIGURE 3| Variables |
| % |
|---|---|---|
|
| ||
| Male | 126 | 50.2 |
| Female | 125 | 49.8 |
|
| ||
| 16–21 | 75 | 29.9 |
| 22–27 | 167 | 66.5 |
| 28–33 | 6 | 1.6 |
| 34–39 | 2 | 0.8 |
| 40–45 | 1 | 0.4 |
|
| ||
| Rural | 31 | 12.4 |
| Suburb | 35 | 13.9 |
| Urban | 185 | 73.7 |
|
| ||
| Clinical | 124 | 49.4 |
| Preclinical | 127 | 50.6 |
|
| ||
| 0 | 127 | 50.6 |
| 1 | 50 | 19.9 |
| 2 | 27 | 10.8 |
| 3 | 39 | 15.5 |
| 4 | 8 | 3.2 |
|
| ||
| 1–4 | 58 | 23.1 |
| 5–8 | 126 | 50.2 |
| ≥ 9 | 67 | 26.7 |
|
| ||
| Yes | 115 | 45.8 |
| No | 136 | 54.2 |
|
| ||
| Yes | 142 | 56.6 |
| No | 109 | 43.4 |
| Variables | Culture + | Culture - | Prevalence | % | OR | CI |
|
|---|---|---|---|---|---|---|---|
|
| |||||||
| Male | 38 | 88 | 33/129 | 30.2 | Reference | - | - |
| Female | 41 | 84 | 41/125 | 32.8 | 0.8847 | 0.5243–1.485 | 0.6523 |
|
| |||||||
| 16–21 | 28 | 47 | 28/75 | 37.3 | 1.521 | 0.8544–2.708 | 0.1541 |
| 22–27 | 47 | 120 | 47/167 | 28.1 | Reference | - | - |
| 28–33 | 4 | 2 | 4/6 | 66.7 | 5.1064 | 0.9047–28.82 | 0.0648 |
| 34–39 | 0 | 2 | 0/2 | 0 | - | - | - |
| 40–45 | 0 | 1 | 0/1 | 0 | - | - | - |
|
| |||||||
| Rural | 13 | 18 | 13/31 | 41.9 | 1.752 | 0.8114–3.827 | 0.1556 |
| Suburb | 12 | 23 | 12/35 | 34.3 | 1.266 | 0.5834–2.611 | 0.5463 |
| Urban | 54 | 131 | 54/185 | 29.2 | Reference | - | - |
|
| |||||||
| Clinical | 38 | 86 | 38/124 | 30.6 | Reference | - | - |
| Preclinical | 41 | 86 | 41/127 | 32.3 | 0.9268 | 0.5494–1.556 | 0.7799 |
|
| |||||||
| 0 | 41 | 86 | 41/127 | 32.3 | 1.628 | 0.7589–3.671 | 0.2105 |
| 1 | 12 | 38 | 12/50 | 24 | Reference | - | - |
| 2 | 10 | 17 | 10/27 | 37 | 2.032 | 0.7532–5.421 | 0.1735 |
| 3 | 15 | 24 | 15/39 | 38.5 | 2.159 | 0.8906–5.661 | 0.1019 |
| 4 | 2 | 6 | 2/8 | 25 | 1.152 | 0.2120–5.923 | 0.8733 |
|
| |||||||
| 1–4 | 12 | 46 | 12/46 | 20.7 | Reference | - | - |
| 5–8 | 51 | 75 | 51/75 | 40.7 | 0.3836 | 0.1880–0.8082 | 0.0086 |
| ≥ 9 | 16 | 51 | 16/51 | 23.9 | 0.8315 | 0.3732–1.914 | 0.6696 |
|
| |||||||
| Yes | 36 | 79 | 36/115 | 31.3 | Reference | - | - |
| No | 43 | 93 | 43/136 | 31.6 | 0.9856 | 0.5805–1.656 | 0.9575 |
|
| |||||||
| Yes | 41 | 101 | 41/142 | 28.9 | Reference | - | - |
| No | 38 | 71 | 38/109 | 34.9 | 0.7585 | 0.4489–1.285 | 0.3112 |
| Variables | Culture + | Culture - | Prevalence | OR | CI |
| |
|---|---|---|---|---|---|---|---|
| % | |||||||
|
| |||||||
| BMLS | 1 | 11 | 1/12 | 8.3 | Reference | - | - |
| MBBS | 7 | 8 | 7/15 | 46.7 | 0.1039 | 0.008583–0.9554 | 0.0302 |
| BNSc | 5 | 8 | 5/13 | 38.5 | 0.1455 | 0.01148–1.109 | 0.078 |
| BRad | 2 | 5 | 2/7 | 28.6 | 0.2273 | 0.01460–2.502 | 0.2432 |
| BPharm | 9 | 5 | 9/14 | 64.3 | 0.05051 | 0.004302–0.4818 | 0.0035 |
| DVM | 7 | 11 | 7/18 | 38.9 | 0.1429 | 0.01178–1.220 | 0.0637 |
|
| |||||||
| Male | 12 | 26 | 12/38 | 31.6 | Reference | - | - |
| Female | 19 | 22 | 19/41 | 46.3 | 0.5344 | 0.2110–1.399 | 0.1794 |
|
| |||||||
| 16–21 | 11 | 17 | 11/28 | 39.2 | 1.941 | 0.2551–27.24 | 0.5809 |
| 22–27 | 19 | 28 | 19/47 | 40.4 | 2.0357 | 0.1967–21.07 | 0.5511 |
| 28–33 | 1 | 3 | 1/4 | 25 | Reference | - | - |
| 34–39 | 0 | 1 | 0/1 | 0 | - | - | - |
| 40–45 | 0 | 1 | 0/1 | 0 | - | - | - |
|
| |||||||
| Rural | 5 | 8 | 5/13 | 38.5 | 1.063 | 0.3326 – 3.432 | 0.924 |
| Suburb | 6 | 6 | 6/12 | 50 | 1.7 | 0.4865 – 5.707 | 0.4058 |
| Urban | 20 | 34 | 20/54 | 37 | Reference | - | - |
|
| |||||||
| Clinical | 15 | 23 | 15/38 | 39.4 | Reference | - | - |
| Preclinical | 16 | 25 | 16/41 | 39 | 1.019 | 0.4314 – 2.394 | 0.9674 |
|
| |||||||
| 0 | 16 | 25 | 16/41 | 39 | 1.493 | 0.3477–5.878 | 0.5966 |
| 1 | 5 | 6 | 5/11 | 45.5 | 1.944 | 0.3735–9.567 | 0.4664 |
| 2 | 3 | 7 | 3/10 | 30 | Reference | - | - |
| 3 | 6 | 9 | 6/15 | 40 | 1.556 | 0.2571–7.161 | 0.6098 |
| 4 | 1 | 1 | 1/2 | 50 | 2.333 | 0.09374–49.78 | 0.5839 |
|
| |||||||
| 1–4 | 4 | 8 | 4/12 | 33.3 | 2.167 | 0.4507–10.13 | 0.3778 |
| 5–8 | 24 | 27 | 24/51 | 47.1 | 3.852 | 0.9882–13.66 | 0.044 |
| ≥ 9 | 3 | 13 | 3/16 | 18.8 | Reference | - | - |
|
| |||||||
| Yes | 16 | 20 | 16/46 | 44.4 | 1.493 | 0.6279–3.588 | 0.3861 |
| No | 15 | 28 | 15/43 | 34.9 | Reference | - | - |
|
| |||||||
| Yes | 17 | 24 | 17/41 | 41.5 | 1.214 | 0.5088–2.911 | 0.6743 |
| No | 14 | 24 | 14/38 | 36.8 | Reference | - | - |
| Number of strains | Antimicrobial resistance phenotypes | MRSA | MAR index | MDR |
|---|---|---|---|---|
| 1 | Susceptible | No | 0 | No |
| 8 | PEN | No | 0.1 | No |
| 1 | FOX | Yes | 0.1 | No |
| 17 | PEN-FOX | Yes | 0.2 | No |
| 5 | PEN-TET | No | 0.2 | No |
| 1 | PEN-GEN | No | 0.2 | No |
| 8 | PEN-FOX-TET | Yes | 0.3 | No |
| 1 | PEN-FOX-CLI | Yes | 0.3 | No |
| 5 | PEN-FOX-CIP | Yes | 0.3 | No |
| 1 | PEN-FOX-ERY | Yes | 0.3 | No |
| 2 | PEN-TET-CIP | No | 0.3 | Yes |
| 2 | PEN-TET-CLI | No | 0.3 | Yes |
| 1 | PEN-FOX-TET-GEN | Yes | 0.4 | Yes |
| 3 | PEN-FOX-TET-CLI | Yes | 0.4 | Yes |
| 8 | PEN-FOX-TET-CIP | Yes | 0.4 | Yes |
| 3 | PEN-FOX-TET-ERY | Yes | 0.4 | Yes |
| 1 | PEN-FOX-TET-CLI-MUP | Yes | 0.5 | Yes |
| 2 | PEN-FOX-TET-GEN-CIP | Yes | 0.5 | Yes |
| 2 | PEN-FOX-TET-ERY-GEN | Yes | 0.5 | Yes |
| 1 | PEN-FOX-ERY-CLI-CIP | Yes | 0.5 | Yes |
| 2 | PEN-FOX-ERY-CLIcons-CHL | Yes | 0.5 | Yes |
| 1 | PEN-FOX-TET-CHL-CIP | Yes | 0.5 | Yes |
| 1 | PEN-FOX-TET-ERY-CIP | Yes | 0.5 | Yes |
| 1 | PEN-FOX-TET-ERY-CLIind-GEN-CIP | Yes | 0.6 | Yes |
| 1 | PEN-FOX-TET-ERY-CLIcons-CIP | Yes | 0.6 | Yes |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntimicrobial Resistance in Staphylococcus · Antibiotic Resistance in Bacteria · Antibiotic Use and Resistance
Introduction
Staphylococcus aureus is a member of the nasal microbiota, and a leading source of healthcare- and community-associated infections in people, especially the methicillin-resistant S. aureus (MRSA) strains, resulting in morbidity and death.^1^ Staphylococcus aureus and MRSA may colonise a variety of places, including the skin and mucosal surfaces of humans and animals, and can contaminate environmental surfaces, food, and water.^1,2,3,4,5^ It is often present in healthy individuals without producing illness, but it is a risk factor for developing staphylococcal infections.^6^ In the healthcare setting, MRSA is of substantial concern, as it can be transmitted across patients, healthcare workers, students, and visitors.^7,8^
When MRSA is transmitted to immunocompromised patients, it can cause a variety of illnesses, ranging from minor skin infections to serious disorders such as endocarditis, osteomyelitis, and sepsis.^9^ Often, the overuse and misuse of antimicrobial agents selects for the emergence of MRSA and multidrug-resistant (MDR)-S. aureus (strains that are resistant to three or more classes of antimicrobial agents).^10^ These can complicate the use of antimicrobial chemotherapy against infectious diseases caused by S. aureus when the strains present with the MDR phenotype.^10^
Healthcare centres generally have sick individuals (humans or animals).^11^ Hence, students who receive clinical training in these settings could be at high risk of contracting clinically resistant S. aureus strains.^12^ Conversely, students colonised with MRSA in their nasal passages have the potential to transmit these strains to sick people and animals (for veterinary students) in healthcare centres during clinical posting and ward rounds,^8,13^ consequently increasing the burden or morbidity to the patients. Nevertheless, MRSA can also be acquired from both the community and animals (zoonosis).^1,2^
Healthcare students can harbour MDR and MRSA in their nostrils and can be the source of transmission to hospitalised patients and other individuals in healthcare facilities. It has been shown that nasal colonisation by S. aureus among these categories of students could be very high.^8^ Collectively, this indicates the need for stringent infection prevention and control measures among medical and health sciences students. It is important to note that these colonisation rates could vary, depending on the duration of contact with hospital settings, and on the type or form of contact with patients. Hence, the need to undertake the present study to determine the level of the indicated epidemiological parameters among various groups of healthcare students (either preclinical or clinical phases).
There are numerous studies, including many from most African countries and cities, that have identified the ecology of MRSA in medical students, as indicated in a systematic review and meta-analysis.^13^ In the global meta-analysis, a pooled prevalence of 28% nasal MRSA carriage in medical students was estimated.^13^ Furthermore, the study found out that a higher pooled prevalence was obtained in students at the clinical phase of training (33%) than in those at the preclinical phase of training (25%).^13^ However, there are very scarce data on subgroup analyses of MRSA carriage rates among students from the other major healthcare disciplines, and the multiple antimicrobial resistance (MAR) indices of the isolates.
This comparative cross-sectional study aims to determine the nasal carriage of S. aureus, its antimicrobial resistance phenotypes and MAR indices, and to assess the factors that could be associated with nasal S. aureus and MDR-S. aureus carriage among medical, veterinary, and health sciences students at Ahmadu Bello University, Zaria, Nigeria.
Methods
Ethical considerations
All study protocols were submitted for ethical review and were approved by the human research ethical committee of Ahmadu Bello University Teaching Hospital (approval no.: NHREC/TR/ABUTH-NHREC/01/02/23). All data generated were treated with the utmost confidence and analysed anonymously. All participants gave written informed consent before enrolment into the study. Samples and data collection from participants were performed according to Helsinki’s declaration as revised in 2024. Data collected were stored in a password-protected computer, only accessible by the principal investigator.
Study area
This study was conducted from 02 January 2024 to 31 July 2024 at the Ahmadu Bello University and Ahmadu Bello University Teaching Hospital, Kaduna State, Nigeria. The university and teaching hospital serve as the main tertiary institution and reference hospital in the Northwest Geopolitical Zone of Nigeria. Moreover, they are the oldest and largest institutions for the training of medical and other healthcare professionals in Northern Nigeria.
Study design, sample size, data collection
This was a cross-sectional study, and the sample size was calculated from the only available previous cross-sectional study on a healthy population of medical students in Nigeria.^14^ Using the 14% prevalence of nasal S. aureus from the study of Adesida et al.,^14^ a minimum sample size of 190 was calculated. However, for statistical credence, 251 healthy students who consented to participate were enrolled. Sociodemographic variables and other data such as prior use of antibiotics, household or hostel room density, and prolonged contact with animals were collated from the participants through structured, paper-based questionnaires administered by the researchers (interviewers).
Sample collection
Nasal samples from both nostrils of eligible participants were collected by some of the investigators in batches and preserved in Amies transport media (HiMedia Laboratories, Maharashtra, India). Within 4 h of collection, the nasal samples were transported to the laboratory on cold packs (2 °C – 8 °C) by some of the investigators, where they were processed for S. aureus recovery. Isolation and identification of isolates were carried out based on the colonies’ colour, size, shape, tube coagulase test, strong mannitol fermentation, and gram staining at the microbiology laboratory of Ahmadu Bello University Teaching Hospital, Zaria, Nigeria.
Laboratory experiments
The nasal swabs were inoculated onto mannitol salt agar (HiMedia Laboratories, Maharashtra, India). After incubation (24 h at 37 ºC), a colony was collected from each sample. The colony was reisolated to obtain a pure S. aureus culture for identification. A rapid in-house tube coagulation reaction and production of bright (strong) yellow colours from mannitol fermentation were used to identify the S. aureus strains. Ecologically, S. aureus is the only coagulase-positive Staphylococcus that readily colonises the nostrils of humans.^15^ Other coagulase-positive staphylococci are specifically adapted to dogs, cats, and horses.^16^ Furthermore, other coagulase-positive staphylococci (such as Staphylococcus delphini, Staphylococcus ursi, Staphylococcus coagulans, and Staphylococcus cornubiensis) do not ferment mannitol, while Staphylococcus pseudintermedius and, Staphylococcus intermedius weakly ferment mannitol after a prolonged incubation of > 24 h.^17^ Hence, the use of tube coagulation tests in addition to strong mannitol fermentation was considered sufficient to identify S. aureus in healthcare students.
The susceptibility of all identified S. aureus strains to different antimicrobial agents was performed using Kirby-Bauer’s disk diffusion method on Mueller-Hinton agar (Oxoid, Manchester, United Kingdom). This was done using the following Oxoid^®^ antibiotic discs (µg/disc): penicillin (1), cefoxitin (30), mupirocin (200), gentamicin (10), clindamycin (2), erythromycin (15), ciprofloxacin (5), chloramphenicol (30), tetracycline (30), and linezolid (10). The 2024 European Committee on Antimicrobial Susceptibility Testing criteria were used for breakpoint interpretation.^18^ Methicillin resistance was determined by the identification of the cefoxitin resistance phenotype on the Mueller-Hinton agar plate. For epidemiological purposes, the MAR index was defined as the number of antibiotics to which an isolate was resistant, divided by the total number of antibiotics tested. Staphylococcus aureus strains with MAR indices of greater than two (> 2) were used to indicate areas with high antibiotic pressure, as previously described.^19^ Furthermore, an isolate was considered MDR if it was resistant to ≥ 3 classes of the antimicrobial agents tested.^20^
Data analysis
EpiInfo® (Centers for Disease Control and Prevention, Atlanta, United States) was used to digitise data collected on paper questionnaires. Categorical sociodemographic variables were expressed as frequencies and compared with the detection rates of nasal S. aureus using the Chi-square (χ^2^) test. Furthermore, bivariate analyses were performed to determine the association between risk factors and sociodemographic variables with S. aureus and MDR-S. aureus carriage rates by MedCalc Version 23.0.2 (MedCalc, Ostend, Belgium). All analysis outputs with p < 0.05 at 95% confidence interval were considered statistically significant.
Results
The 251 medical and health science students were enrolled in different undergraduate programmes. The age range of the participants was from 17 years to 44 years with a mean ± standard deviation of 23.1 ± 3.5. About 50.2% were men and 124 of the students were in the clinical phase of training (exposed to healthcare settings). Most of the students in their clinical phase were in their first year (n = 50, 40.3%), followed by those in their third year (n = 39, 31.5%) (Table 1).
One hundred and eighty-five (73.7%) of the students were residing in urban settlements, 31 (12.4%) resided in rural areas, and 35 (13.9%) in suburban settlements. One hundred and twenty-six of the students resided in houses with a density of 5–8 individuals (50.2%). One hundred and fifteen (45.8%) consumed antibiotics within the last 3 months before their enrolment into the study (Table 1).
Prevalence of Staphylococcus aureus and methicillin-resistant Staphylococcus aureus among healthcare students
The nasal carriage rate of S. aureus and MRSA among the 251 participants was 31.5% (n = 79) for S. aureus and 23.5% (n = 59) for MRSA (Figure 1a). Specifically, the prevalence of S. aureus was highest among the Bachelor of Nursing Science students (13/32, 40.6%), followed by Doctor of Veterinary Medicine (18/53, 34%), Bachelor of Pharmacy (3/40, 32.5%), Bachelor of Radiography students (7/23, 30.4%), Bachelor of Medicine, Bachelor of Surgery (MBBS) (15/53, 28.3%), and Bachelor of Medical Laboratory Science students (12/50, 24%). Furthermore, the prevalence of MRSA was highest among the Bachelor of Nursing Science (10/32, 31.3%), followed by Bachelor of Pharmacy (10/40, 25%), Doctor of Veterinary Medicine (13/53, 24.5%), Bachelor of Medical Laboratory Science (10/50, 20%), MBBS students (10/53, 18.9%), and Bachelor of Radiography students (4/23, 17.4%). Students in the clinical phase had a relatively higher frequency of nasal MRSA (31/124, 25%) than those in the preclinical phase (28/127, 22.1%) (odds ratio = 1.1786, p = 0.5814) (Figure 1b). There was no statistically significant association between the nasal carriage rate of S. aureus (χ^2^ = 2.97, p = 0.705) and MRSA (χ^2^ = 6.695, p = 0.2443) with the programme of study of the participants (p > 0.05) (Figure 1b).
(a) Prevalence of nasal Staphylococcus aureus and methicillin-resistant S. aureus carriage and (b) association between the phase of study and antibiotic use with the prevalence of nasal methicillin-resistant S. aureus among among health sciences students of the Ahmadu Bello University; Zaria, Nigeria, January 2024 to July 2024.
Prevalence and factors associated with nasal Staphylococcus aureus carriage
The frequency of nasal S. aureus carriage in female students (33/126, 32.8%) was relatively higher than in male students (41/125, 30.2%). Students within the age range of 28–33 years had the highest prevalence of nasal S. aureus (4/6, 66.7%), followed by those 16–21 years old (28/75, 37.3%), and those 22–27 years old (47/167, 28.1%). None of the students within the 34–45 range had S. aureus carriage (Table 2). Students aged 28–33 years had the highest odds of nasal S. aureus carriage (odds ratio = 5.106, 95% confidence interval: 0.9047–28.82) (Table 2). Students who resided in rural areas had the highest prevalence of nasal S. aureus (13/31, 41.9%), followed by those in the suburbs (12/35, 34.3%) and those in urban settlements (54/185, 29.2%). Students in the preclinical phase of their training had a relatively higher frequency of nasal S. aureus carriage (41/127, 32.3%) than those in the clinical phase (38/124, 30.6%). Of those in the clinical phase of their training, those who had been on clinical and/or laboratory posting for 3 years (15/39, 38.5%) had the highest prevalence of S. aureus, while the lowest was recorded among students who had been on posting for 1 year (12/50, 24%) (Table 2). Students who resided in houses with densities of 5–8 individuals (51/75, 40.7%) had the highest prevalence of S. aureus, followed by those who resided in houses with ≥ 9 individuals (16/51, 23.9%) (Table 2). Students who resided in houses with a density of 5–8 individuals had statistically significant odds of nasal S. aureus carriage (odds ratio = 0.3836, 95% confidence interval: 0.19–0.81, p = 0.0086) (Table 2).
Students who used antibiotics within the last 3 months before their enrolment into the study had a closely similar frequency of nasal S. aureus carriage (31.6%) compared with those with no antibiotic use 3 months before enrolment in the study (31.3%). Students who had prolonged contact with pets or livestock had a relatively lower frequency of nasal S. aureus carriage (41/142, 28.9%), than those who did not (38/109, 34.9%) (Table 2).
Factors associated with nasal carriage of multidrug resistant-Staphylococcus aureus
The frequency of multidrug resistant-S. aureus was highest among Bachelor of Pharmacy students (9/14, 64.3%), followed by MBBS (7/15, 46.7%), Doctor of Veterinary Medicine (7/18, 38.9%), and Bachelor of Nursing Science students (5/13, 38.5%). The frequency of nasal MDR-S. aureus in female students (19/41, 46.3%) was relatively higher than in male students (12/38, 31.6%). Students within the age range of 22–27 years had the highest prevalence of nasal MDR-S. aureus (19/47, 40.4%), followed by those 16–21 years (11/28, 39.2%), and those 28–33 years, (1/4, 25%) (Table 3). Students who resided in suburban areas had the highest prevalence of nasal MDR-S. aureus (6/12, 50%), followed by those living in rural areas (5/13, 38.5%), and those in urban settlements (20/54, 37%). Students in the clinical phase of their training had a closely similar frequency of nasal MDR-S. aureus carriage (15/38, 39.4%) to those in the preclinical phase (16/41, 39%). Of those in the clinical phase of their training, those that had been on clinical/laboratory posting for 4 years (1/2, 50%) had the highest frequency of MDR-S. aureus, while the lowest was recorded in students who had been on posting for 2 years (3/10, 30%) (Table 3). Students who resided in houses with densities of 5–8 individuals (24/51, 47.1%) had the highest frequency of MDR-S. aureus, followed by those that resided in houses with 1–4 individuals (4/12, 33.9%). Students who used antibiotics within the last 3 months before their enrolment into the study had a relatively higher frequency of nasal MDR-S. aureus carriage (44.4%), compared with those with no antibiotic use 3 months before enrolment in the study (34.9%). Students who had prolonged contact with pets or livestock had a relatively higher frequency of nasal MDR-S. aureus carriage (17/41, 41.5%) than those who did not (14/38, 36.8%). Both MBBS and Bachelor of Pharmacy students had statistically significant high frequencies of nasal MDR-S. aureus (both p < 0.05). Furthermore, students who resided in houses with a density of 5–8 individuals had the highest odds of nasal MDR-S. aureus carriage (odds ratio = 3.85, 95% confidence interval: 0.99–13.66, p = 0.0044) (Table 3).
Antimicrobial resistance rates in Staphylococcus aureus isolates
Out of the 79 S. aureus strains identified, the pattern of resistance to tested antimicrobial agents, in descending frequency, was as follows: penicillin (93.7%), cefoxitin (73.4%), tetracycline (49.4%), ciprofloxacin (29.1%), gentamicin (10.1%), clindamycin (8.7%), erythromycin (7.6%), chloramphenicol (3.8%), erythromycin-constitutive clindamycin (2.5%), erythromycin-inducible clindamycin resistance (1.3%), high-level mupirocin (1.3%). All strains were susceptible to linezolid, and one strain (1.3%) was completely susceptible to all the antibiotics tested (Figure 2). About 39.2% of strains presented the MDR phenotype, of which one strain presented an erythromycin-inducible clindamycin resistance (Figure 2). Over 30% of the S. aureus strains had similar MDR phenotypes (Table 2).
Antimicrobial resistance rates in 79 Staphylococcus aureus strains obtained from the participants in Zaria, Nigeria, January 2024 to July 2024.
Eight (10.1%) of the S. aureus strains were solely resistant to penicillin, and one (1.3%) to cefoxitin, with a MAR index of 0.1 (Table 4). Two strains had the highest antimicrobial resistance profile, with a MAR index of 0.6 for resistance to penicillin-cefoxitin-tetracycline-clindamycin-gentamicin-ciprofloxacin and penicillin-cefoxitin-tetracycline-erythromycin-clindamycin-ciprofloxacin (Table 4). Strains with a MAR index of 0.2 were the most predominant (29.1%), followed by strains with a MAR index of 0.3 (24%), 0.4 (18.9%), 0.5 (12.6%), and 0.6 (2.5%) (Figure 3).
Levels and frequency of multiple antimicrobial resistance indices of Staphylococcus aureus isolates in Zaria, Nigeria, January 2024 to July 2024.
Discussion
An overall prevalence of 31.5% for carriage of S. aureus and 23.5% for carriage of MRSA were obtained in this study. Subgroup analysis showed that nursing science students had the highest prevalence of both S. aureus and MRSA carriage. To our knowledge, this is the first epidemiological study on the MAR indices of nasal S. aureus colonisation rate in Nigeria. The 31.5% prevalence of S. aureus recorded in this study is similar to the results of studies done among healthcare students identified in medical and health science students in Plateau and Delta states of Nigeria in 2018 (37.3%) and 2024 (38.5%).^21,22^ However, the finding from the present study is similar to the nasal S. aureus carriage reported in other countries such as Nepal in 2011 (35%), and Poland in 2018 (30%).^23,24^ A relatively lower prevalence of 16.8% was reported in medical students at Kaduna State University (Nigeria) in 2024, and 14% at Babcock University (Nigeria) in 2020.^25,26^ Furthermore, lower prevalence values were reported in China (23.1%), Thailand (29.7%), Ethiopia (27.1%), Turkey (21.4%), Germany (22.3%) and Saudi Arabia (25.3%) from 2011 to 2022.^27,28,29,30,31,32^ Much higher nasal S. aureus carriage was reported by Ogefere and Ogunleye (54.7%)^33^ and Solomon et al. (66.6%),^34^ both in 2019 in Nigeria, and 50% by Rosales-González et al.^12^ in 2024 in Spain. The variations observed in the nasal S. aureus carriage from these studies could be because of differences in the study protocols, sample size, laboratory methods for S. aureus identification, and levels of antibiotic use by the students.
In the present study, there were higher odds of nasal S. aureus carriage with age and household density of the students. A similar finding was reported in China in 2017, where medical students of the age group 20–30 years were found to have a higher nasal S. aureus carriage.^35^ It was previously reported that the nasal S. aureus carriage tends to increase with age and population density.^36^ Households and communities in congested conditions are more likely to be exposed to S. aureus colonisation, with an increased transmission rate.^37,38^
Although not statistically significant, there was a trend for higher S. aureus colonisation in the nasal cavity in female students, and those who resided in rural settlements. A similar study in Madagascar previously reported higher S. aureus nasal carriage in female medical students and healthcare workers in 2016.^39^ The higher rate in female students could be because of biological reasons or differences in susceptibility to S. aureus colonisation as a result of circulating steroid hormones.^40^ The higher S. aureus rate among students who were rural residents could be because of the relatively higher contact rate of the students with animals in the rural areas, and poor personal and environmental hygiene that could facilitate the increased transmission of S. aureus.^41^ This is similar to the findings of Ansari et al.^42^ in 2016, who reported a higher nasal S. aureus carriage rate in medical students who were rural residents than in their urban counterparts.
The overall prevalence of MRSA recorded in this study is 22.7%, and comparable to 26.2% (Delta state of Nigeria), and 27.1% (Ethiopia).^22,31^ However, a higher prevalence of nasal MRSA (48.8%) was reported by Solomon et al.,^34^ while a lower value (12.2%) was reported by Rosales-González et al.^12^ Several factors have been linked to increased S. aureus carrier status, including sinusitis, antimicrobial treatments, prolonged contact with animals, smoking, and contact with healthcare professionals.^29,43,44^
Although not statistically significant, nasal MRSA carriage was higher in students with antibiotic usage in the previous 3 months. This was similar to studies in Ethiopia (2023) and Malaysia (2012) that found that recent antibiotic usage was associated with higher nasal carriage of MRSA.^45,46^ Furthermore, students who reported prolonged contact with animals (pets or livestock) had a relatively higher frequency of nasal MDR-S. aureus carriage than those who did not. This finding is not unexpected, as occupational or companionship contact with animals is a major risk factor for MDR-S. aureus.^47^
It is important to remark that the prevalence of MDR-S. aureus was statistically significantly higher in pharmacy and MBBS students. Similar findings were reported by Obajuluwa, Parom and Kubau (2024) in Nigeria.^25^ Moreover, MDR-S. aureus was significantly associated with households with 5–8 individuals. These reflect the degree of contact with patients in the clinical phase of training, as students who had 4 years in clinical posting had the highest MDR-S. aureus carriage. This finding indicates that once healthcare students start interacting directly with patients in a clinical setting, their likelihood of carrying MDR-S. aureus is much higher compared to before their clinical exposure as a result of the increased contact with other potential MDR-S. aureus carriers in healthcare settings, such as healthcare professionals (especially physicians and nurses), patients, and contaminated environment surfaces and equipment. Furthermore, high household density can facilitate the transmission of MDR strain because of increased contact with many individual carriers within the same rooms and houses. The strong antibiotic selective pressure among congested populations produces a suitable condition that could facilitate the emergence and efficient dissemination of many MDR bacteria, such as MDR-S. aureus.^48^
Generally, up to 30% of the human population is asymptomatic and permanently colonised with S. aureus in their nostrils.^49^ However, MDR-S. aureus strains, especially MRSA, can be translocated from the nose to other parts of the body, causing infection or facilitating transmission to other humans, animals, and the environment through nasal secretion droplets during sneezing, coughing, kissing, or handshaking.^50,51,52^
Most of the S. aureus isolates were resistant to penicillin and ciprofloxacin. This could be explained by the widespread and indiscriminate use of these classes of antibiotics in the treatment of S. aureus.^49^ Similar findings were found in many other studies in Nigeria (2011 to 2024).^24,25,34,53^ The presence of mupirocin-resistant S. aureus (1.4%) may render mupirocin less effective as a nasal decoloniser or as topical treatment for superficial skin infections.^54^
Fortunately, linezolid resistance was not detected in any of the S. aureus strains and very low resistance (only one student) to chloramphenicol was recorded. However, tetracycline resistance was high. This suggests that our research participants had prior contact with livestock, as tetracycline resistance is more frequent in livestock breeders than in healthy humans with no occupational contact with livestock.^55^ This is because tetracycline is a very common antimicrobial agent used in livestock husbandry, prophylaxis, and as a first-line treatment of most bacterial infections. Consequently, bacteria (including S. aureus) found in farm settings (including farmers) exhibit high selective pressure against tetracycline.^55^
Remarkably, one strain presented a characteristic erythromycin-inducible clindamycin resistance. This phenotypic feature could be useful as a marker for the surveillance of S. aureus CC398 lineage.^55^ However, this finding is subject to further molecular confirmation, such as the screening for the ermT and ermC genes.^55,56^
Multidrug resistance was high in the S. aureus carriers, as some isolates presented resistance against five or six classes of antibiotics (MAR index ≥ 5). Therefore, MDR-S. aureus may limit the available chemotherapeutic options against staphylococcal and many other Gram-positive bacterial infections.^53^ This shows that most of the S. aureus strains originated from areas with high antibiotic pressure.^16^
Recommendations
First, it is recommended to consider the improvement of infection prevention and control measures in the wards, clinics, laboratories, pharmacies, and veterinary hospitals where healthcare students undertake training. Furthermore, the implementation of active hospital and antimicrobial resistance surveillance systems should include all medical, and other groups of healthcare students as potential reservoirs of nasal MDR-S. aureus and MRSA.
Second, it will be interesting to determine the clonality of MRSA strains with similar antimicrobial resistance profiles from different students. Hence, pulse-field gel electrophoresis and/or whole phylogenomic analysis could provide insight into the potential transmission route of these strains.
Limitations
This study is not without limitations. First, the use of phenotypic identification of antimicrobial resistance using disk diffusion may not account for some antimicrobial agents that could be phenotypically susceptible when tested by the disk diffusion method but could still carry the antimicrobial resistance genes. For instance, linezolid resistance is best identified by the determination of minimum inhibition concentrations through broth dilution tests or E-tests. Second, the use of automated bacterial identification systems such as Bactec and Vitek II compact, and advanced equipment such as the Matrix-assisted laser desorption ionisation-time of flight (mass spectrometry could have allowed the possibility to determine the performance characteristics of combined tube coagulase test and strong mannitol fermentation in the identification of S. aureus.
Conclusion
High levels of nasal MRSA and MDR-S. aureus were obtained from this study. The predominance of strains with high MAR indices indicates that strains were from locations with much antibiotic pressure. Furthermore, many strains with similar antimicrobial resistance profiles could indicate potential interhost transmission within human clusters either at the community level or clinics and laboratories where these students were performing their postings. Collectively, these students could serve as vectors of transmission of MDR and virulent strains to the patients or the community. Based on this, it could be inferred that the medical and health science students are a potential source of MRSA strains at Ahmadu Bello University, Zaria, Nigeria.^7^
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1González-Machado C, Alonso-Calleja C, Capita R. Prevalence and types of methicillin-resistant Staphylococcus aureus (MRSA) in meat and meat products from retail outlets and in samples of animal origin collected in farms, slaughterhouses and meat processing facilities. A review. Food Microbiol. 2024;123:104580. 10.1016/j.fm.2024.10458039038886 · doi ↗ · pubmed ↗
- 2Liu A, Garrett S, Hong W, Zhang J. Staphylococcus aureus infections and human intestinal microbiota. Pathogens. 2024;13(4):276. 10.3390/pathogens 1304027638668232 PMC 11053856 · doi ↗ · pubmed ↗
- 3Roy MC, Chowdhury T, Hossain MT, et al. Zoonotic linkage and environmental contamination of Methicillin-resistant Staphylococcus aureus (MRSA) in dairy farms: A one health perspective. One Health. 2024;18:100680. 10.1016/j.onehlt.2024.10068039010963 PMC 11247269 · doi ↗ · pubmed ↗
- 4Algammal AM, Hetta HF, Elkelish A, et al., Methicillin-resistant Staphylococcus aureus (MRSA): One health perspective approach to the bacterium epidemiology, virulence factors, antibiotic-resistance, and zoonotic impact. Infect Drug Resist. 2020;13:3255–3265. 10.2147/IDR.S 27273333061472 PMC 7519829 · doi ↗ · pubmed ↗
- 5Santos GAC, Dropa M, Rocha SM, Peternella FAS, Razzolini MTP. Staphylococcus aureus and methicillin-resistant Staphylococcus aureus (MRSA) in drinking water fountains in urban parks. J Water Health. 2020;18(5):654–664. 10.2166/wh.2020.04233095190 · doi ↗ · pubmed ↗
- 6Taylor TA, Unakal CG. Staphylococcus aureus infection [homepage on the Internet]. Stat Pearls – NCBI Bookshelf. Available from: https://www.ncbi.nlm.nih.gov/books/NBK 441868/28722898 · pubmed ↗
- 7Samuel P, Kumar YS, Suthakar BJ, et al. Methicillin-resistant Staphylococcus aureus colonization in intensive care and burn units: A narrative review. Cureus. 2023;15(10):e 47139. PMCID: .38021721 10.7759/cureus.47139 PMC 10650970 · doi ↗ · pubmed ↗
- 8Oliveira EMN, Carvalho ARB, Ferreira AM et al., Colonization of methicillin-resistant Staphylococcus aureus among healthcare students: An integrative review. Sao Paulo Med J Revista paulista de medicina. 2021;139(6):607–614. 10.1590/1516-3180.2020.0564.r 2.2204202134787295 PMC 9634839 · doi ↗ · pubmed ↗