Vitiligo-associated protection against basal cell carcinoma: Clinical observations
Alex Rooker, Marcel W. Bekkenk, Elisabeth H. Jaspars, Rosalie M. Luiten, Walbert J. Bakker

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
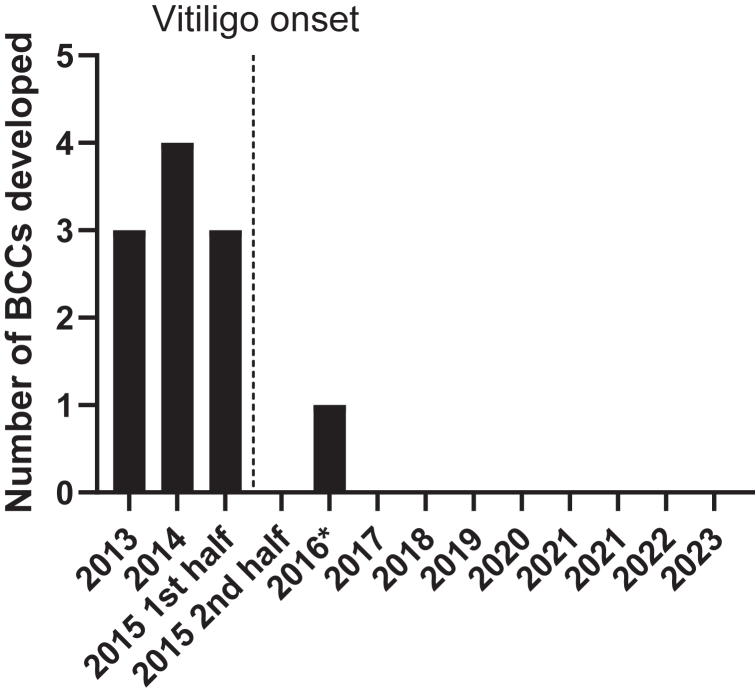 Figure 1
Figure 1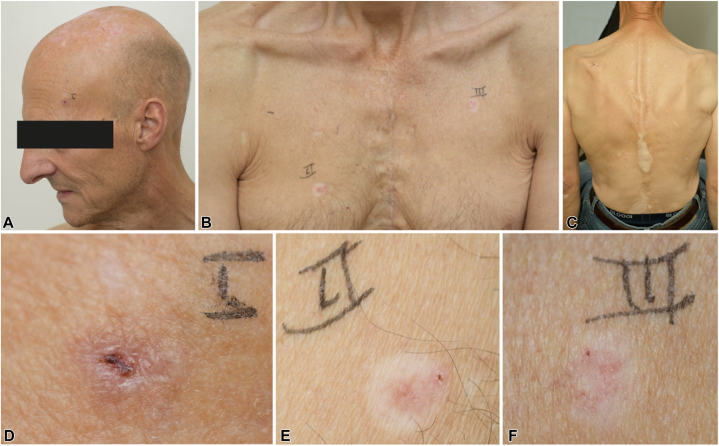 Figure 2
Figure 2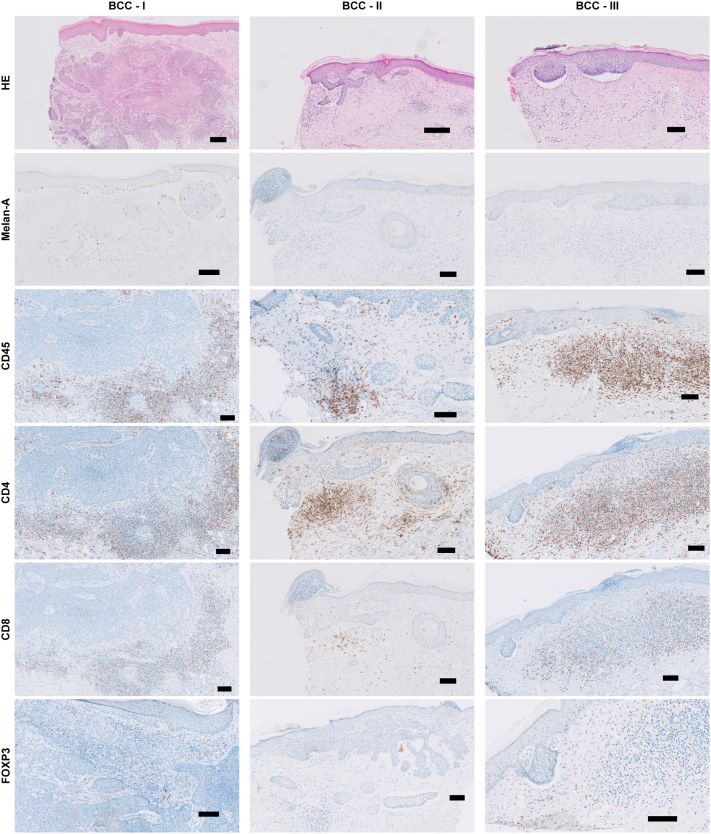 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
Topicsmelanin and skin pigmentation · Herpesvirus Infections and Treatments · Flavonoids in Medical Research
Introduction
Although patients with vitiligo partially lack skin pigmentation, these patients have a lower risk of nonmelanoma skin cancers than healthy controls, particularly basal cell carcinoma (BCC).1^,^2 In this report, we present 2 cases that underline this remarkable finding. We hypothesize that vitiligo immune reactivity against melanocytes, generally present in BCCs, could lead to BCC tumor destruction via bystander lysis. These patient cases provide clinical evidence of vitiligo melanocyte-specific immune reactions that may inhibit BCC tumor development and/or promote tumor regression, offering insights into the reduced BCC risk observed in patients with vitiligo.
Case Description
Basal cell nevus syndrome patient with vitiligo
We here describe a 36-year-old woman patient with genetically confirmed diagnosis of basal cell nevus syndrome or Gorlin syndrome since 2013, characterized by frequent and continuous development of multiple BCC lesions. In 2015, the patient developed depigmented skin lesions and was diagnosed with nonsegmental vitiligo. Remarkably, after the onset of vitiligo, she did not develop any new BCC lesions, which persisted during 9 years of follow-up until present (Fig 1). Of note, patients with basal cell nevus syndrome rarely experience a pause of more than a year between new lesions.3 The patient did develop new odontogenic keratocysts, indicating ongoing disease activity.Fig 1BCC development in the BCNS—patient with vitiligo before and after vitiligo onset. Graph depicts the number of new BCCs that developed per year. ∗BCC located under hairline. BCC, Basal cell carcinoma; BCNS, basal cell nevus syndrome.
BCC patient with vitiligo
A 61-year-old man presented at our dermatology outpatient clinic with several skin lesions (Fig 2, A, B). Since the age of 59 years, the patient had developed 3 red lesions on healthy skin and over a 2-year period the patient had experienced a total of 5 BCCs (Table I), a nodular BCC on the left temple (I), 3 superficial BCCs on the right (II) and left (III) sides of the chest and left shoulder blade (IV), and a solid growing BCC on the middle region of the back (V). His medical history includes Hodgkin disease at the age of 28 years, which was treated with total lymph node irradiation (total dose of 36 Gy) resulting in a complete remission. At the age of 48 years, diffuse large B-cell lymphoma (stage IVa) was observed with extensive localization (brain, spleen, bone marrow, thorax, and soft tissue). He was treated with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) multiagent chemotherapy and local radiotherapy resulting again in a complete remission. Despite fatigue and persisting lymphadenopathy, no relapse was found. His fatigue was due to cardiac problems, possibly induced by the chemotherapy. His dermatologic history reveals nonsegmental vitiligo starting around the age of 30 years (Fig 2, C).Fig 2. The patient with vitiligo and BCC. A nodular BCC situated on the left temple (A) and 2 superficial BCCs located on the right and left side of the chest (B). Depigmented lesions on the back indicate vitiligo (C). The nodular tumor—I is pigmented (D). In contrast, the superficial BCC—II on the right side of the chest (E) and superficial BCC—III on the left side of the chest (F) show a depigmented halo and signs of regression. BCC, Basal cell carcinoma.Table ICharacteristics of excised BCC lesionsTumorLocationTypeMelanocytes in lesion∗Macroscopic haloClinical regressionBCC-ILeft templeNodularYesNoNoBCC-IIRight side of the chestSuperficialNoYesYesBCC-IIILeft side of the chestSuperficialNoYesYesBCC-IVLeft shoulderSuperficialndndndBCC-VMiddle region of the backSuperficialYesndndBCC, Basal cell carcinoma; nd, not determined.∗Melanocyte presence was determined by immunohistochemical staining of Melan-A.
Further examination revealed that the nodular BCC-I on the left temple and solid BCC-V on the middle region of the back presented as a typical pigmented BCC (Fig 2, D). In contrast, the 2 superficial BCCs on the right and left side of the chest (II and III) exhibited a depigmented halo (Fig 2, E, F). Remarkably, these 2 halo BCCs demonstrated signs of spontaneous regression, in contrast to the pigmented BCC.
Histologic examination of the patient using an hematoxylin-eosin stain of BCC biopsies (I-III) confirmed that the diagnosis of superficial and nodular BCCs. The BCCs (II and III) with clinical signs of spontaneous regression had a macroscopic depigmented halo, and displayed the absence of melanocytes, evidenced by the negative Melan-A staining. In contrast, in the BCC-I biopsies melanocytes were present throughout the epidermis and in the tumor (Fig 3).Fig 3. Immune infiltrate in 3 BCC lesions by immunohistochemical staining. Nodular BCC on the left temple—I, superficial BCC on the right side of the chest—II, superficial BCC on the left side of the chest—III. The following stainings were performed: Hematoxylin and eosin (H&E), Melan-A, CD45, CD4, CD8, and FOXP3. Black bars are 100 μm, except for BCC—I H&E and BCC—II H&E and Melan-A, black bars are 200 μm. BCC, Basal cell carcinoma.
To further characterize the immune microenvironment and infiltrate within the BCC lesions, immunohistochemical stainings were performed for CD45 (pan-leukocyte marker), CD3, CD4, and CD8 (T-cell markers), CD20 (B-cell marker), CD57 (natural killer cell marker), and FoxP3 (regulatory T-cell marker). An increase in CD45^+^ immune cells was observed in the tumor-surrounding stroma in all BCCs (Fig 3). B cells and natural killer cells were absent, as indicated by negative CD20 and CD57 stainings (not shown). Both CD4^+^ helper and CD8^+^ cytotoxic T cells were detected, with CD4^+^ T cells being more abundantly present than CD8^+^ T cells. FoxP3^+^ regulatory T cells were found more frequently in the nodular tumor than in superficial tumors, albeit at low numbers compared with the total CD4^+^ T-cell population, suggesting that most CD4^+^ T cells did not have a regulatory phenotype.
Discussion
Until recently, patients with vitiligo were assumed to have an increased risk of developing skin cancer and were advised to avoid sun exposure. However, epidemiologic meta-analysis data indicates that patients with vitiligo have a decreased risk of developing melanoma and keratinocyte cancers, as compared with healthy controls.1 The basal cell nevus syndrome-vitiligo case described here suggests a protective effect of vitiligo against BCC initiation, whereas the BCC-vitiligo case suggests that vitiligo may promote tumor regression.
Immunohistochemical analysis shows substantial immune cell presence in all BCCs. Interestingly, the 2 clinically regressing BCCs lacked melanocytes. Since BCCs in general contain melanocytes, it seems likely that the melanocytes were destroyed by the vitiligo immune reaction.4^,^5 It has been shown that antigen-negative cells in tumors can be destroyed by T cells via bystander lysis, through secretion of cytotoxic cytokines (eg, interferon gamma) as long as antigen-positive tumor cells are present.6 The melanocytes present in BCCs may act as antigen-positive cells, which are recognized by the melanocyte-reactive T cells that mediate vitiligo. This T-cell activation within the BCC tissue may subsequently induce bystander lysis of BCC cells, resulting in tumor regression. The absence of melanocytes in the clinically regressing BCCs is indicative of the hypothesis of bystander lysis. In support of this hypothesis, we previously observed that recognition of melanocytes by vitiligo specific CD8^+^ T cells can induce apoptosis of adjacent (bystander) keratinocytes in a skin explant model.7 We found abundant presence of CD4^+^ T cells in the tumor microenvironment (Fig 3), which have been reported to produce cytotoxic interferon gamma and induce senescence of tumor cells.8
The remaining BCC that did not show clinical regression, despite immune infiltration and melanocyte presence, might eventually have undergone clinical regression. However, all the examined BCCs were excised and only this snapshot is available.
These 2 cases, provide valuable clinical indications supporting the hypothesis that vitiligo autoimmune reactivity can inhibit BCC initiation and/or growth by the mechanism of bystander lysis.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rooker A.Ouwerkerk W.Bekkenk M.W.Luiten R.M.Bakker W.J.The risk of keratinocyte cancer in vitiligo and the potential mechanisms involved J Invest Dermatol 1442202423424210.1016/j.jid.2023.08.01237791932 · doi ↗ · pubmed ↗
- 2Teulings H.E.Overkamp M.Ceylan E.Decreased risk of melanoma and nonmelanoma skin cancer in patients with vitiligo: a survey among 1307 patients and their partners Br J Dermatol 1681201316217110.1111/bjd.1211123136900 · doi ↗ · pubmed ↗
- 3Verkouteren B.J.A.Cosgun B.Reinders M.G.H.C.A guideline for the clinical management of basal cell naevus syndrome (Gorlin-Goltz syndrome)Br J Dermatol 1862202221522610.1111/bjd.2070034375441 PMC 9298899 · doi ↗ · pubmed ↗
- 4Florell S.R.Zone J.J.Gerwels J.W.Basal cell carcinomas are populated by melanocytes and Langerhans [correction of Langerhan’s] cells Am J Dermatopathol 2312001242810.1097/00000372-200102000-0000411176048 · doi ↗ · pubmed ↗
- 5Frey L.M.Houben R.Bröcker E.B.Pigmentation, melanocyte colonization, and p 53 status in basal cell carcinoma J Skin Cancer 2011201134972610.1155/2011/349726 PMC 298975921152129 · doi ↗ · pubmed ↗
- 6Hoekstra M.E.Bornes L.Dijkgraaf F.E.Long-distance modulation of bystander tumor cells by CD 8+ T cell-secreted IFNγNat Cancer 13202029130110.1038/s 43018-020-0036-432566933 PMC 7305033 · doi ↗ · pubmed ↗
- 7van den Boorn J.G.Konijnenberg D.Dellemijn T.A.Autoimmune destruction of skin melanocytes by perilesional T cells from vitiligo patients J Invest Dermatol 129920092220223210.1038/jid.2009.3219242513 · doi ↗ · pubmed ↗
- 8Braumüller H.Wieder T.Brenner E.T-helper-1-cell cytokines drive cancer into senescence Nature 4947437201336136510.1038/nature 1182423376950 · doi ↗ · pubmed ↗