Krukenberg’s Spindle-Like Corneal Changes in a Patient With Prolonged ICU Admission: A Case Report
Yuto Shiotani, Daiyu Kosen, Keiki Shimizu, Akiko Ohno-Tanaka

TL;DR
A 39-year-old man developed Krukenberg’s spindle-like corneal changes after a long ICU stay due to thyroid storm and infective endocarditis.
Contribution
This case report describes a rare variant of Krukenberg’s spindles linked to prolonged ICU care, not typical pigment dispersion syndrome.
Findings
The patient showed bilateral brownish linear corneal changes resembling Krukenberg’s spindles.
Classic causes like PDS and drug-induced keratopathy were ruled out.
ICU-related factors may have contributed to the atypical pigment dispersion.
Abstract
Krukenberg's spindles are vertical, spindle-shaped pigment deposits on the posterior cornea and are primarily associated with pigment dispersion syndrome (PDS). We present a case of Krukenberg's spindle-like corneal changes in a 39-year-old male patient following prolonged ICU management for thyroid storm complicated by infective endocarditis. The patient's complex ICU course included mechanical ventilation, veno-arterial extracorporeal membrane oxygenation (VA-ECMO), and multiple medications. Ophthalmological examination revealed bilateral, brownish, linear changes in the central corneal stroma and a normal endothelial cell count. Various conditions, including drug-induced keratopathy and systemic diseases, were excluded. The findings presented a distinctive pattern of Krukenberg's spindle-like corneal changes following a prolonged ICU stay. While morphologically resembling classic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1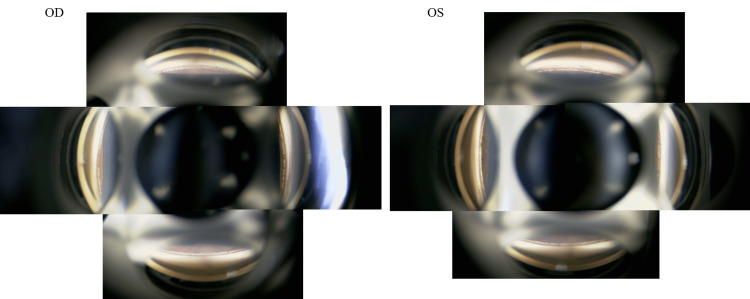 Figure 2
Figure 2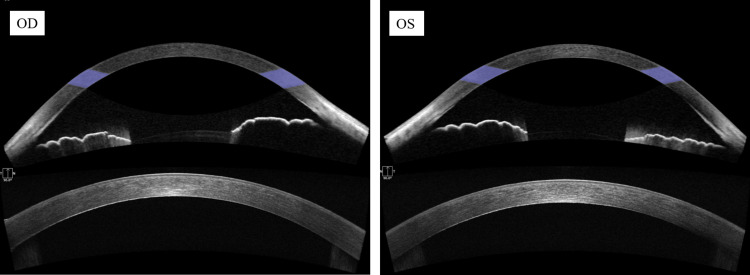 Figure 3
Figure 3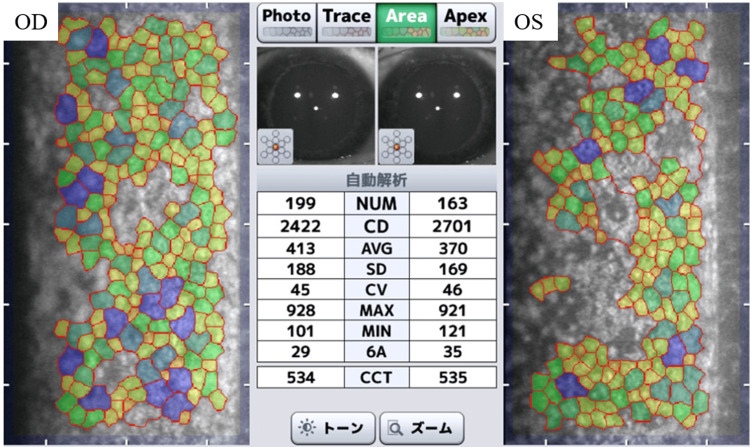 Figure 4
Figure 4| Start date | End date | Medication | Route of administration |
| July 31 | September 27 | Dimethyl isopropylazulene | Topical |
| July 31 | October 10 | Iodine and potassium iodide | Oral |
| August 2 | September 27 | Zinc oxide | Topical |
| August 3 | October 1 | White petrolatum | Topical |
| August 6 | September 4 | Heparinoid | Topical |
| August 7 | September 5 | Sodium hyaluronate | Topical |
| August 7 | November 6 | Sulfadiazine silver | Topical |
| August 11 | September 9 | Ofloxacin | Topical |
| August 12 | August 17 | Naldemedine tosilate | Oral |
| August 14 | October 24 | Gentamicin sulfate | Topical |
| August 15 | October 16 | Bisoprolol | Patch |
| August 15 | October 31 | Vidarabine | Topical |
| August 18 | November 1 | Acetaminophen | Oral |
| August 19 | November 6 | Lemborexant | Oral |
| August 20 | October 22 | Clostridium butyricum | Oral |
| August 20 | November 6 | Lansoprazole | Oral |
| August 22 | October 8 | Potassium gluconate | Oral |
| August 25 | October 4 | Warfarin potassium | Oral |
| August 25 | October 10 | Thiamazole | Oral |
| August 31 | November 6 | Trazodone hydrochloride | Oral |
| September 2 | November 6 | Sodium gualenate hydrate and sodium bicarbonate | Oral |
| September 12 | September 12 | Risperidone | Oral |
| October 11 | October 18 | Calcium lactate hydrate | Oral |
| October 11 | November 6 | Alfacalcidol | Oral |
| October 11 | November 6 | Levothyroxine sodium hydrate | Oral |
| October 12 | October 12 | Cefalexin | Oral |
| October 15 | October 15 | Glucose | Oral |
| October 15 | October 24 | Edoxaban tosilate hydrate | Oral |
| October 20 | November 6 | Sucrose and povidone-iodine | Topical |
| October 20 | November 6 | Betamethasone valerate and gentamicin sulfate | Topical |
| October 20 | November 6 | Hydrocortisone butyrate | Topical |
| July 31 | July 31 | Ceftriaxone sodium hydrate | Intravenous injection |
| July 31 | July 31 | Cefepime dihydrochloride hydrate | Intravenous injection |
| July 31 | July 31 | Epinephrine | Intravenous injection |
| July 31 | July 31 | Sodium bicarbonate | Intravenous injection |
| July 31 | July 31 | Electrolyte solution (IV fluid) | Intravenous injection |
| July 31 | July 31 | Ketamine hydrochloride | Intravenous injection |
| July 31 | July 31 | Fursultiamine hydrochloride | Intravenous injection |
| July 31 | August 1 | Rocuronium bromide | Intravenous injection |
| July 31 | August 3 | Vancomycin hydrochloride | Intravenous injection |
| July 31 | August 5 | Vasopressin | Intravenous injection |
| July 31 | August 6 | Calcium gluconate hydrate | Intravenous injection |
| July 31 | August 6 | Dobutamine hydrochloride | Intravenous injection |
| July 31 | August 11 | Noradrenaline | Intravenous injection |
| July 31 | August 12 | Midazolam | Intravenous injection |
| July 31 | August 12 | Glucose (IV fluid) | Intravenous injection |
| July 31 | August 13 | Ringer’s acetate (IV fluid) | Intravenous injection |
| July 31 | August 18 | Hydrocortisone sodium phosphate | Intravenous injection |
| July 31 | August 18 | Fentanyl citrate | Intravenous injection |
| July 31 | August 18 | Landiolol hydrochloride | Intravenous injection |
| July 31 | August 19 | Omeprazole sodium | Intravenous injection |
| July 31 | October 6 | Meropenem hydrate | Intravenous injection |
| July 31 | October 10 | Cefazolin sodium | Intravenous injection |
| August 1 | August 8 | Thiamine disulfide phosphate, pyridoxine hydrochloride, and cyanocobalamin | Intravenous injection |
| August 1 | October 11 | Ringer’s acetate (IV fluid) | Intravenous injection |
| August 2 | October 10 | Heparin sodium | Intravenous injection |
| August 7 | August 23 | Potassium chloride | Intravenous injection |
| August 9 | October 27 | Propofol | Intravenous injection |
| August 14 | August 20 | Dexmedetomidine hydrochloride | Intravenous injection |
| July 31 | August 24 | Thiamazole | Intravenous injection |
| August 18 | August 20 | Antithrombin gamma | Intravenous injection |
| August 19 | August 19 | Menatetrenone | Intravenous injection |
| August 19 | August 24 | Cefepime dihydrochloride hydrate | Intravenous injection |
| August 20 | September 16 | Magnesium sulfate hydrate | Intravenous injection |
| August 20 | August 25 | Acetaminophen | Intravenous injection |
| August 21 | August 23 | Potassium chloride | Intravenous injection |
| August 24 | October 13 | Cefmetazole sodium | Intravenous injection |
| August 25 | August 25 | Furosemide | Intravenous injection |
| August 27 | August 27 | Dibasic sodium phosphate hydrate sodium | Intravenous injection |
| August 31 | September 15 | Cefazolin sodium | Intravenous injection |
| September 8 | September 8 | Remifentanil hydrochloride | Intravenous injection |
| September 8 | September 12 | Electrolyte solution (IV fluid) | Intravenous injection |
| September 9 | September 9 | Flurbiprofen axetil | Intravenous injection |
| September 20 | September 20 | Acetaminophen | Intravenous injection |
| October 7 | October 10 | Dexamethasone sodium phosphate | Intravenous injection |
| October 11 | October 11 | Metoclopramide hydrochloride | Intravenous injection |
| October 27 | November 6 | Heparin calcium | Subcutaneous injection |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBiomedical Research and Pathophysiology · Intraoperative Neuromonitoring and Anesthetic Effects · Ophthalmology and Eye Disorders
Introduction
Corneal change can result from various causes. For example, Krukenberg’s spindles, seen in pigment dispersion syndrome (PDS), form a characteristic pattern of pigment deposition encountered in corneal changes [1-4]. While progress in critical care medicine has improved the survival rate of severely ill patients [5], there are scarce reports of corneal changes associated with a prolonged ICU stay. This report describes a unique case of bilateral, Krukenberg’s spindle-like corneal changes that developed after extended ICU management for thyroid storm complicated by infective endocarditis. Only a few corneal anomalies associated with the ICU environment have previously been described, and ophthalmological monitoring is vital in critically ill patients. To the best of our knowledge, this report is the first to describe Krukenberg’s spindle-like corneal changes associated with prolonged ICU management.
Case presentation
The patient was a 39-year-old male with a past medical history of Graves’ disease and atopic dermatitis. His ophthalmological history was unremarkable; he wore soft contact lenses, for which he had been undergoing regular eye examinations. He had no previous history of eye disease. He had been receiving routine contact lens examinations at another ophthalmology clinic, but had not visited it recently before his current hospitalization. His previous visits had revealed no ophthalmological abnormalities, although the details could not be ascertained as he had not recently undergone a detailed examination. Before his current illness, his activities of daily living had been normal, and his health had been generally good. On July 31, 2023, the patient presented to the emergency department with a fever and altered mental status. Initial tests revealed that he was experiencing a thyroid storm complicated by infective endocarditis with marked mitral valve vegetation secondary to *Staphylococcus aureus *bacteremia. Due to the severity of his condition, he was admitted to the ICU for further management. Following stabilization in the ICU and social rehabilitation, he presented to our ophthalmology department in April 2024 with a mild, subjective decrease in vision.
The patient’s ICU management was complex and required advanced circulatory management, including the use of veno-arterial extracorporeal membrane oxygenation (VA-ECMO) and an intra-aortic balloon pump (IABP) from July 31 to August 9 for the treatment of severe shock. He received several medications, including broad-spectrum antibiotics, such as vancomycin, cefazolin, and meropenem, as well as specific treatments for the thyroid storm, such as methimazole, Lugol’s solution (5% iodine and 10% potassium iodide in distilled water), hydrocortisone, and β-blockers. Following a tracheostomy, he required ongoing respiratory management and continuous hemodiafiltration (CHDF). His hospital course was further complicated by the development of septic emboli, which resulted in multiple cerebral infarctions and symmetrical peripheral gangrene in his extremities, requiring the amputation of multiple digits. Additionally, he developed pressure ulcers and an inferior vena cava thrombus related to the ECMO cannulation. Despite these complications, his condition gradually improved, and he was eventually transferred to a rehabilitation facility. His ICU management required multiple medications for supportive care and treatment of his various conditions. Table 1 shows a detailed list of all the medications administered during his ICU stay, none of which are known to cause linear corneal stromal changes.
An ophthalmological evaluation in April 2024 found the patient’s best-corrected visual acuity (BCVA) to be 20/16 in the right eye and 20/20 in the left eye with a subjective refractive error of -6.00/1.0×160° in the right eye and -5.50/1.55° in the left eye. A slit-lamp examination revealed bilateral, linear, brownish, corneal stromal changes confined primarily to the mid-to-deep stroma of the central cornea and exhibiting a fine, punctate pattern (Figure 1).
Anterior segment photographsBilateral slit-lamp photographs demonstrating symmetrical, Krukenberg’s spindle-like corneal changes. The black arrowheads highlight the brownish, linear, stromal changes in both eyes, each measuring approximately 1 mm in width and 6 mm in length. Both eyes retained overall corneal transparencyOD: right eye; OS: left eye
There was no evidence of a cataract. Gonioscopy found wide, open angles with mild pigmentation (Figure 2).
Gonioscopy imagesGonioscopic examination of anterior chamber angles. Both eyes demonstrated widely open angles with mild pigmentation and consistent structural characteristicsOD: right eye; OS: left eye
There were no signs of anterior segment inflammation, such as keratic precipitates, cells, or a flare in the anterior chamber. Fundoscopic examination found no abnormalities of the retina, optic disc, or retinal vasculature in either eye. Dynamic perimetry confirmed right homonymous hemianopia, which was consistent with the patient's previous cerebral infarctions. Anterior segment optical coherence tomography (OCT) demonstrated hyperreflective areas corresponding to the clinically observed changes. No significant change was found in the corneal shape or thickness (Figure 3).
Anterior segment OCT imagesBilateral anterior segment OCT images. Upper panel: iris configuration: no posterior iris bowing with open angles in either eye. Lower panel: corneal stromal analysis: hyperreflective areas corresponding to the changes observed with a slit lamp were visible in the deep stroma of both eyes, which had a normal corneal thickness and shapeOD: right eye; OS: left eye; OCT: optical coherence tomography
Specular microscopy revealed a normal corneal endothelial cell count of 2422 cells/mm² in the right eye and 2701 cells/mm² in the left eye (Figure 4).
Corneal endothelial cell microscopySpecular microscopy of the corneal endothelium. Both eyes showed a normal endothelial cell count (right eye: 2,422 cells/mm²; left eye: 2,701 cells/mm²). The colors in the image, which classify individual endothelial cells based on their area, with yellow to green representing smaller areas and blue representing larger areas, are useful for visually assessing the variation in cell size. Although this automated analysis revealed variations in cell size, cellular morphology was generally normalOD: right eye; OS: left eye
Laboratory tests, including a complete blood count, lactate dehydrogenase, ceruloplasmin, and serum protein electrophoresis, which were performed to exclude systemic diseases, found no abnormalities.
The patient’s extensive ICU stay and polypharmacy raised suspicion of a drug-induced corneal change. However, the causative drug could not be identified. Betamethasone phosphate ophthalmic solution was administered to decrease the stromal changes, but it produced no significant improvement. Consequently, no further treatment was administered at the time, and the patient was placed under observation. The corneal changes and visual acuity were stable at the subsequent visits.
Discussion
This case was challenging to diagnose owing to the unique findings of bilateral, central, linear, corneal, stromal changes discovered after prolonged ICU management. Krukenberg’s spindles appear as vertical, spindle-shaped pigment deposits on the corneal endothelium and are primarily associated with PDS. In PDS, posterior bowing of the iris leads to mechanical contact with the lens-zonular apparatus, which releases pigment particles [1]. PDS presents three cardinal signs: Krukenberg’s spindles in the corneal endothelium, iris transillumination defects in the mid-peripheral region, and increased pigmentation of the trabecular meshwork [6]. Idiopathic PDS with classic Krukenberg’s spindles typically occurs bilaterally in young, myopic male patients, while secondary pigment dispersion causing Krukenberg’s spindle-like deposits has been observed following trauma, uveitis, intraocular surgery, and medication [4]. In our case, the corneal changes morphologically resembled Krukenberg’s spindles in their bilaterality and preservation of the corneal endothelial cell count, both of which align with typical PDS findings. Histologically, melanin granules reaching the corneal endothelium are incorporated into endothelial cells, and cellular function and transparency remain intact despite long-term pigment deposition [7]. However, our case was marked by the absence of iris transillumination defects and trabecular meshwork pigmentation, and the anterior segment OCT demonstrated no posterior iris bowing.
The pathophysiology of pigment dispersion is well-understood. In the reverse pupillary block mechanism, the iris acts as a flap valve, creating a pressure differential that causes posterior iris bowing and increased irido-zonular contact. Mechanical friction between the iris pigment epithelium and zonular structures during pupillary movement then results in the liberation of pigment into the anterior chamber [1-4]. We hypothesized that the unique ICU environment in our case created conditions triggering these mechanisms via novel pathways. Our patient’s thyroid storm likely played a substantial role, as this extreme, thyrotoxic state enhances sensitivity to catecholamines [8], leading to sympathetic hyperactivity affecting pupillary dynamics [9]. Recent studies have supported this association by demonstrating sympathetic predominance and bilateral mydriasis during thyroid storm [10]. Additionally, the prolonged ICU stay involved other, potential, contributory factors, including complex drug interactions, patient positioning, systemic inflammation, and changes in ocular surface homeostasis that may have further promoted abnormal pupillary dynamics and pigment dispersion.
A key, contributory mechanism was the pharmacodynamic interactions producing opposite, autonomic effects. During ICU management, the patient received sympathomimetics, such as epinephrine, which can cause mydriasis through sympathetic activation by stimulating α1-adrenergic receptors in the pupillary dilator muscle [11]. Additionally, he received sedative-analgesics, including remifentanil and midazolam, which are known to have miotic effects [12]. This drug antagonism, combined with the endogenous, sympathetic drive from the thyroid storm, likely produced anomalous iris movements, which may have increased iris-lens zonule contact, thereby promoting pigment release through mechanisms consistent with the usual pathophysiology of pigment dispersion. The combination of the thyroid storm-induced autonomic dysfunction and complex, pharmacological interactions likely created the unique circumstances that caused the distinctive corneal findings in this case.
Drug-induced keratopathy was among the foremost items in the differential diagnosis of this case. Drug-induced corneal deposits are typically bilateral and symmetrical and often improve after drug discontinuation. Brown deposits are associated with the use of chlorpromazine and rifabutin, among other medications [13]. A comprehensive review of all the medications administered during the patient's ICU stay (Table 1) revealed no previously reported association with corneal changes. Additionally, a review of past studies found no association between any of these medications and PDS or pigmentary glaucoma. While some agents may affect pupillary dynamics, no direct association with Krukenberg’s spindle formation has previously been reported.
Systemic diseases known to cause corneal changes were also considered. Various systemic conditions, such as Wilson’s disease, cystinosis, and multiple myeloma, are known to cause corneal changes [14], but the findings of the present case were not congruent with these symptoms. Normal serum ceruloplasmin and copper levels ruled out Wilson’s disease. Cystinosis was excluded as there were no systemic symptoms or urinalysis and blood test results suggestive of this disease. Multiple myeloma was deemed unlikely owing to the absence of M-protein on serum protein electrophoresis as well as the normal serum free light chain ratio. Based on all these findings, the present case was considered a unique condition related to the ICU environment: a rare form of pigment dispersion phenomenon leading to Krukenberg’s spindle-like corneal changes. While not presenting the complete clinical picture of PDS, it shared features with the latter, such as Krukenberg’s spindle-like pigment deposits and a normal corneal endothelial cell count.
This case report has several limitations. Due to the absence of detailed pre-ICU ophthalmological records, we could not confirm that the corneal changes developed de novo following a prolonged ICU stay. Therefore, the possibility that these findings were due to coincidental, pre-existing changes could not be fully ruled out. However, several factors supported an ICU-related etiology: the temporal relationship with ICU admission, the absence of classic PDS features (iris transillumination defects and trabecular pigmentation), and the unprecedented combination of multiple physiological stressors during the ICU stay that provided a plausible mechanism for activating pigment dispersion pathways.
The findings of the present case emphasize the importance of conducting an ophthalmological evaluation for patients with a history of an extended ICU stay during recovery from a critical illness. While detailed ophthalmological examinations are often difficult to perform during an ICU stay, appropriate ophthalmological monitoring during the recovery period can facilitate the early detection of corneal changes and the assessment of their impact on long-term visual function. The intraocular pressure and other relevant parameters of our present patient will be monitored using a management protocol similar to that for PDS to prevent complications, such as pigmentary glaucoma. This report offers new perspectives on the relationship between severe, systemic diseases requiring ICU management and Krukenberg’s spindle-like corneal changes.
Conclusions
This report of bilateral Krukenberg’s spindle-like corneal changes following prolonged ICU management for thyroid storm complicated by infective endocarditis revealed features distinct from those of classic Krukenberg’s spindles and other known corneal pathologies. These findings suggest that complex, ICU-related factors likely caused the abnormal pigment dispersion. The distinctive ocular findings highlight the importance of conducting ophthalmological assessment after recovery in patients with an extended ICU stay.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pigment dispersion syndrome: a brief overview J Clin Transl Res Zeppieri M 3443508202236518550 PMC 9741933 · pubmed ↗
- 2Pigment dispersion syndrome and its implications for glaucoma Surv Ophthalmol Bustamante-Arias A Ruiz-Lozano RE Carlos Alvarez-Guzman J Gonzalez-Godinez S Rodriguez-Garcia A 7437606620213344462910.1016/j.survophthal.2021.01.002 · doi ↗ · pubmed ↗
- 3Pigment dispersion syndrome and pigmentary glaucoma: a review and update Int Ophthalmol Scuderi G Contestabile MT Scuderi L Librando A Fenicia V Rahimi S 165116623920192972184210.1007/s 10792-018-0938-7 · doi ↗ · pubmed ↗
- 4Pigment dispersion syndrome and pigmentary glaucoma--a major review Clin Exp Ophthalmol Niyadurupola N Broadway DC 8688823620081927848410.1111/j.1442-9071.2009.01920.x · doi ↗ · pubmed ↗
- 5Changes in hospital mortality for United States intensive care unit admissions from 1988 to 2012 Crit Care Zimmerman JE Kramer AA Knaus WA 017201310.1186/cc 12695 PMC 405729023622086 · doi ↗ · pubmed ↗
- 6Current concepts in pigmentary glaucoma Surv Ophthalmol Farrar SM Shields MB 233252371993809510510.1016/0039-6257(93)90008-u · doi ↗ · pubmed ↗
- 7Light and electron microscopy in absolute glaucoma with pigment dispersion phenomena and contusion angle deformity Am J Ophthalmol Iwamoto T Witmer R Landolt E 420434721971531521410.1016/0002-9394(71)91315-8 · doi ↗ · pubmed ↗
- 8High risk and low prevalence diseases: thyroid storm Am J Emerg Med Farooqi S Raj S Koyfman A Long B 1271356920233710490810.1016/j.ajem.2023.03.035 · doi ↗ · pubmed ↗