VSD device closure in situs inversus with dextrocardia: technical challenges and solutions: a case report
Abhimanyu Uppal, Bhushan Shah, Rambabu Sharma, Ashok Garg

TL;DR
This case report describes a successful percutaneous closure of a heart defect in a child with a rare condition involving mirrored internal organs.
Contribution
The paper presents a novel approach to device closure in a rare anatomical condition using tailored technical modifications.
Findings
Percutaneous VSD closure in SI-DC is feasible with adjusted fluoroscopic angles and wire techniques.
The procedure was performed safely without excess contrast or radiation due to meticulous planning.
A Konar-MFO device was successfully deployed via a retrograde approach in a mirror-image anatomy.
Abstract
Situs inversus with dextrocardia (SI-DC) is rarely associated with congenital heart defects. Traditionally, ventricular septal defect (VSD) in such patients has been managed surgically. Percutaneous VSD device closure in SI-DC, albeit a suitable alternative, has been seldom reported. The present report describes the unique challenges of mirror-image cardiac anatomy and suggests technical modifications for successful percutaneous closure. A 4-year-old boy, previously diagnosed with SI-DC and a moderate-size perimembranous VSD, presented with a history of poor weight gain and dyspnea. A 2D echocardiogram indicated that the septal defect was suitable for device closure. The procedure was adapted to account for the altered cardiac anatomy by adjusting the fluoroscopic angles and wire-torquing maneuvers. A Konar-multifunction occluder device MFO® 7-5mm was successfully deployed via…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
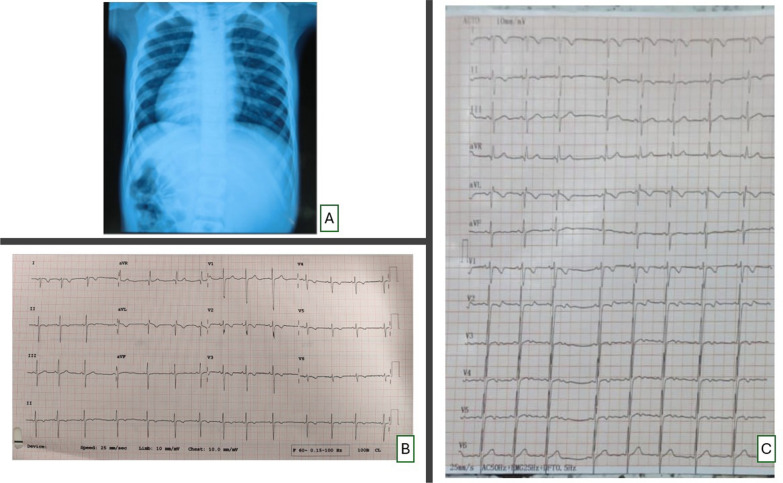 Figure 1
Figure 1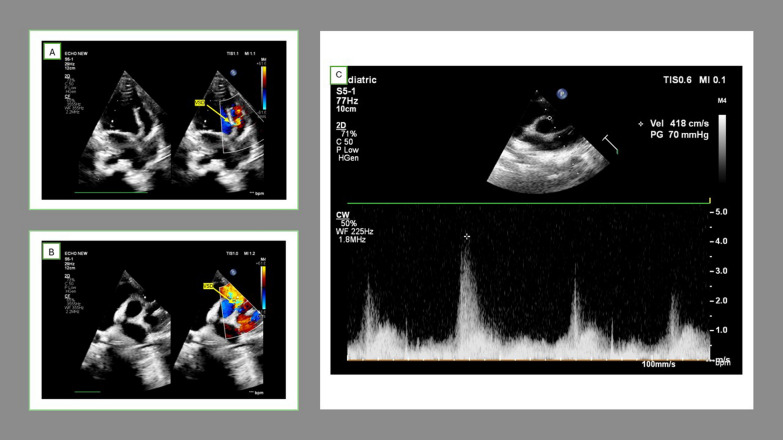 Figure 2
Figure 2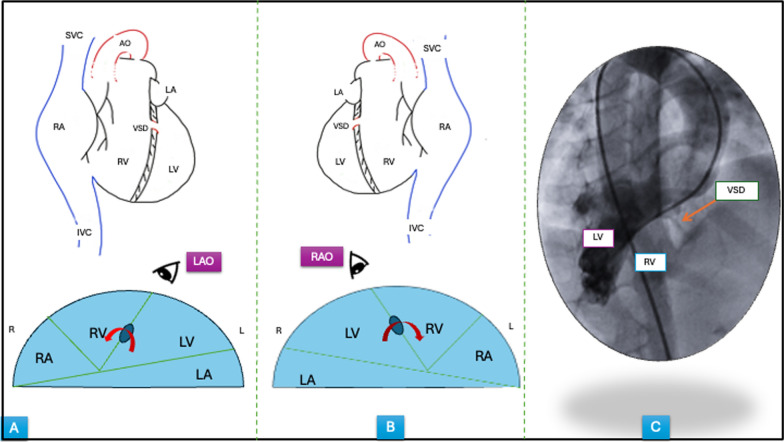 Figure 3
Figure 3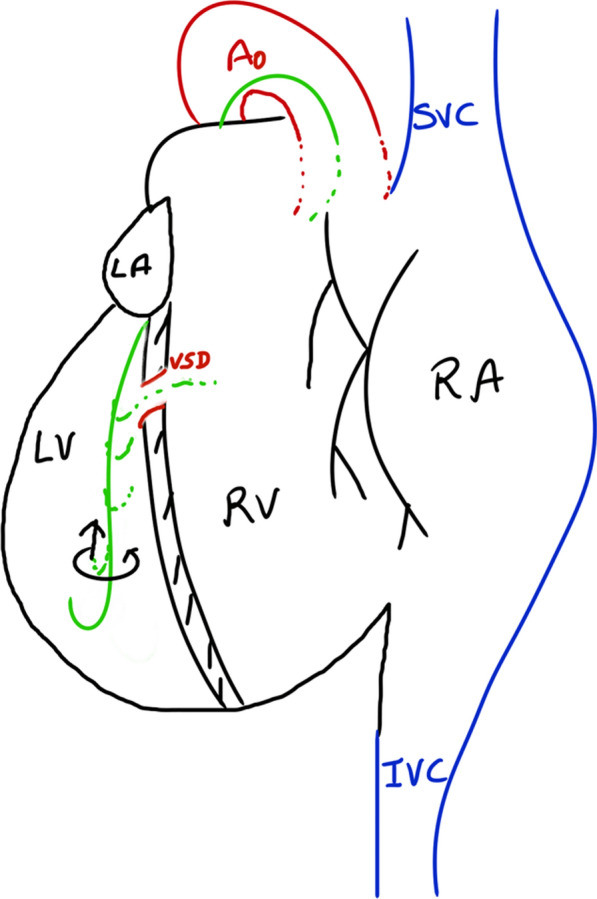 Figure 4
Figure 4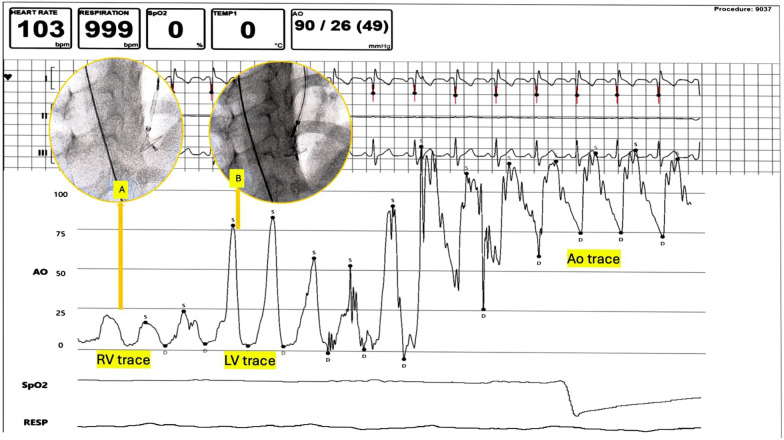 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Congenital Anomalies and Fetal Surgery · Pediatric Hepatobiliary Diseases and Treatments
Introduction
Dextrocardia is a rare congenital abnormality with an estimated incidence ranging from 1 in 8000 to 25,000 live births [1]. SI-DC associated with a perimembranous (PM) ventricular septal defect (VSD) is even rarer [2]. Most cases reported in the literature have undergone surgical closure [3, 4]. However, VSD patch closure in this scenario is challenging for surgeon due to the altered spatial orientation of cardiac structures. This requires the surgeon to improvise the approach angle, potentially increasing the risk of conduction tissue damage [5].
A percutaneous device closure approach in this scenario is ideal, as it avoids surgical scars and offers a shorter hospital stay, among other benefits. However, literature on technical modifications for successful VSD device closure in SI-DC patients, is limited [6, 7]. There is a potential for excess contrast use and radiation exposure since the interventionist faces an unfamiliar cardiac anatomy.
In the present case report, we share our experience of closing a perimembranous VSD using retrograde technique with a Konar multifunction occluder (MFO) device in the setting of SI-DC. We aim to provide insights into technical modifications for proper device deployment and use of echocardiographic and hemodynamic guidance to avoid excess contrast and radiation exposure.
Case report
A 4-year-old boy presented with history of poor weight gain and dyspnea with easy fatiguability while playing and running. Incidental murmur at birth had led to the diagnosis of SI-DC with perimembranous VSD. Past medical history was suggestive of recurrent respiratory infections and diaphoresis during infancy for which oral diuretics were started. Patient was subsequently lost to follow-up before presenting to our institute with aforementioned complaints.
On examination, the patient had a blood pressure of 94/60 mmHg in the right upper limb with a pulse rate of 100 beats per minute. The child was underweight for his age (16.0 kg; expected weight ≈ 18–19 kg) with a height of 98cm (within two standard deviations for his age). Cardiovascular examination revealed the apex beat in the right 5th intercostal space at mid-clavicular line with a harsh grade 4 pansystolic murmur, best heard at the lower right sternal border.
Except for mild anemia (Hb level of 10.1 gm/dL), all other relevant blood investigations were within normal range.
A chest X-ray indicated mirror-image dextrocardia with cardiomegaly (cardiothoracic ratio = 0.67), with notable bilateral pulmonary plethora (Fig. 1A).Fig. 1. Chest X-ray and 12-lead ECG of the patient. A: Chest X-ray postero-anterior view showing mirror-image dextrocardia with cardiomegaly and prominent pulmonary arterial markings. B: Twelve lead electrocardiogram of the patient with leads placed in conventional locations. Inverted P and T waves in leads I and aVL, upright P, QRS, and T waves in lead aVR, and progressively decreasing R wave amplitude from V1 to V6 all suggest dextrocardia with situs inversus. C. Twelve lead electrocardiogram of the patient with precordial leads positioned in mirror image positions on right side of chest. Normal R wave progression is seen from V1 to V6
A conventional 12-lead ECG showed inverted P and T waves in leads I and aVL, upright P, QRS, and T waves in lead aVR, and progressively decreasing R wave amplitude from V1 to V6 (Fig. 1B). Normal R wave progression was noted when precordial leads were repositioned in their corresponding mirror-image locations on the right side of chest (Fig. 1C).
Two-dimensional echocardiography (2D ECHO) with color Doppler confirmed situs inversus with dextrocardia, a dilated left atrium, and left ventricle (left ventricle end diastolic diameter, LVEDD = 40.5 mm, z-score = + 2.17) with a PM-VSD (3 mm toward the right ventricle, RV exit and 5 mm at the left ventricle, LV entry site) with a left-to-right shunt. This shunt was best visualized in the right parasternal short-axis view at the 2 o'clock position (mirror image of the usual 10 o’clock location for PM-VSDs) (Fig. 2A, B). The VSD was restricted by septal tricuspid adhesions and a peak gradient of 70 mmHg was noted across VSD (Fig. 2C). The defect was separated from aortic valve by a distance of 3 mm.Fig. 2. Echocardiogram of the patient showing tunnel shaped perimembranous VSD. A four chamber view showing color flow turbulence across the defect. B Parasternal short axis view showing VSD jet at 2’ o clock location. C Pressure gradient across VSD noted in parasternal short axis view. Abbreviations LV, left ventricle, RV, right ventricle, PA, Pulmonary artery, VSD, ventricular septal defect
Combined with the patient’s medical history, the final diagnosis was SI-DC with PM VSD with significant left to right shunt that needed closure.
After obtaining informed consent from parents, patient was considered for closure. The procedure was performed under local anesthesia and conscious sedation. Cardiac catheterization suggested a significant left-to-right shunt with a suitable pulmonary vascular resistance/systemic vascular resistance (PVR/SVR) ratio (Table 1).Table 1. Catheterization data. Hemodynamic recordings and oximetry readings of various cardiac chambersPressure (mmHg)Oximetry (% saturation)Right atrium mean675.5Right ventricular systolic pressure3988Pulmonary artery40/15/2190Pulmonary capillary wedge pressure (mean)7100Left ventricular systolic pressure110100Aorta108/70/8499QP/QS = 2.35, Pulmonary vascular resistance to systemic vascular resistance ratio = 0.09
Following catheterization study, VSD device closure was performed in the same sitting via transfemoral arterial access with plan to proceed via retrograde device deployment technique.
In SI-DC, the left–right relationship of cardiac structures is reversed while the anterior–posterior relations remain unchanged. The base to apex axis of interventricular septum points from posterior to anterior in a rightward direction [4]. Therefore, the septal defect would be best profiled in a right anterior oblique view (opposite to the conventional left anterior oblique view) while maintaining the usual cranial angulation (Fig. 3A–C).Fig. 3. Schematic drawings of normal vs. mirror image anatomy and LV angiogram. Normal heart, A and situs inversus, dextrocardia heart, B Upper panels show the reversed right to left relationship of cardiac structure in mirror-image anatomy, and lower panels show preserved anterior–posterior relationship. The best fluoroscopic angles to visualize the defect in interventricular septum are shown in lower panels. C LV angiogram done for the patient in RAO with cranial projection (40°–20°). Abbreviations SVC, superior vena cava, IVC, inferior vena cava, LV, left ventricle, RV, right ventricle, LA, left atrium, RA, right atrium, VSD, ventricular septal defect, PA, pulmonary artery, Ao, aorta, LAO, left anterior oblique, RAO, right anterior oblique
To facilitate crossing the VSD from the LV side in SI-DC, we had to modify our technique of wire crossing by making a counterclockwise torque (instead of clockwise torquing) such that the wire faced the leftward-located RV and crossed the VSD (Fig. 4).Fig. 4. Modified wire-torquing Schematic drawing of situ inversus with dextrocardia heart showing use of counter-clockwise torque (arrows) during withdrawal of guidewire (green) to engage and cross the VSD. Abbreviation VSD, ventricular septal defect
With this pre-procedure planning, a 5F pigtail catheter was advanced through right femoral arterial access and an LV angiogram was performed in RAO-CRAN 40°–20° projection to delineate the VSD. The defect was then crossed with a Terumo 0.035 (260 cm) wire which was then stationed into a branch of the left pulmonary artery. The remaining steps were the same as standard retrograde VSD closure procedure.
Pigtail catheter was exchanged for 5F Lifetech Steerease®the delivery sheath. A Konar MFO device 7-5 mm (2 mm larger than the smallest diameter measured on echo) was mounted on a 3F delivery cable and advanced through delivery system.
The device deployment steps were done under hemodynamic and echocardiographic guidance. Since MFO is a very low-profile device, continuous hemodynamic pressure recordings can be obtained through side-arm of delivery system even when the device is slenderized inside the sheath. The low-pressure disk of the device was unsheathed in the RV cavity, while the delivery sheath was connected to the pressure tracing monitor. At this point, RV pressure tracings were noted on the monitor. The sheath-device assembly were withdrawn together, and when the pressure tracings were noted to transition to LV pressures, the remaining part of the device was unsheathed (Fig. 5). The optimal device position was reconfirmed by bedside echo. Post-device release, LV angiogram confirmed optimal device position (Fig. 5, Video).Fig. 5VSD deployment under hemodynamic guidance. The right disk of MFO device is unsheathed in RV cavity (inset A) and the entire delivery system is withdrawn with close monitoring of pressure tracings. As soon as LV tracing is noted, the entire device is deployed (inset B). Abbreviations RV, right ventricle, LV, left ventricle, Ao, aorta, VSD, ventricular septal defect, MFO, multifunction occluder
The total contrast volume used was 35 ml (upper limit of contrast defined by creatinine clearance for this patient was 95 ml). The fluoroscopic time, air kerma, and DAP for this procedure were 6.4 min (average: 5.5–8.5 min for this procedure at our institute), 172 mGy (average: 161-250mGy) and 8.70 Gy-cm^2^ (average: 7.5–9.5 mGy-cm^2^). The procedure was completed in 25 minutes without any intra-procedural complications.
The patient had an uneventful recovery and was discharged after 24 h of observation. He continues to be in our regular outpatient follow-up for last 6 months. The patient had improvement in dyspnea post-intervention and has gained 3.8 kg weight in the last 6 months. Serial ECHO examinations suggested that the VSD device has remained in situ, without any residual shunt or aortic/tricuspid valvulopathy. No conduction system disturbances were noted over the last six months of follow-up.
Discussion
SI-DC complicated by VSD is a rare clinical scenario conventionally treated by open surgery [3, 4]. This cardiac malposition may pose difficulties for the surgeon and carries a potential risk of complications like conduction system damage. [5]
A percutaneous approach, while ideal, requires careful pre-procedure planning to avoid multiple contrast injections and excess radiation exposure when attempting to close the defect in an unorthodox cardiac position. Device deployment steps must be tailored to the unfamiliar cardiac anatomy.
As described earlier, in SI-DC the base-to-apex axis of the interventricular septum faces rightward in the chest cavity, with a reversed right-left relationship of cardiac structures. Technical modifications required include: (1) changing the fluoroscopic projection to RAO-CRAN for the LV angiogram, (2) applying counterclockwise torque (instead of the usual clockwise) to advance the guidewire across the VSD into the left-oriented RV, and (3) using hemodynamic and echocardiographic assistance during device deployment. The procedure time can be further reduced by choosing the retrograde technique of device deployment. Previous reports of device closure in this scenario have used conventional arteriovenous (AV) loop formation method [6] or relied on contrast injections for device positioning. [7] Conventional AV loop method can be challenging in SI-DC anatomy as described previously [6]. Device deployment under hemodynamic and echocardiographic guidance can obviate the need for excess contrast and radiation use as described in present case.
For small- to moderate-sized VSDs, our institutional protocol is to use Amplatzer duct occluder II and Konar MFO devices. In this case, we used the Konar MFO device- a self-expandable, double-disk device made from a layer of nitinol wire mesh. The device has a 2.4-mm-long hub with a screw attached to retention disks on either side, allowing it to be deployed retrogradely or antegradely [8].
To the best of our knowledge, use of this device for VSD closure in SI-DC setting has not been reported yet.
Conclusion
Device closure of VSD in atypical scenarios such as SI-DC is both safe and feasible if meticulous pre-procedural planning is undertaken with consideration of the altered cardiac anatomy. Modification of fluoroscopic angles and wire torquing maneuvers along with use of hemodynamic guidance form the crux of a safe and successful intervention in this scenario.
Supplementary Information
Additional file 1.Additional file 2.