Investigation of the Effect of Preconditioning with Ultrasound on Fat Graft Survival
Arif Yılmaz, Bilge Kağan Yılmaz, Çiğdem Karaca, Necmettin Karasu

TL;DR
This study investigates how therapeutic ultrasound affects the survival of fat grafts in rats, finding that massage-like effects may improve survival more than ultrasound energy alone.
Contribution
The study introduces the idea that the mechanical massage effect of therapeutic ultrasound, rather than the ultrasound energy itself, may enhance fat graft survival.
Findings
Therapeutic ultrasound increased fat graft vascularization but did not improve survival rates.
The preoperative–postoperative massage group showed statistically significantly higher fat graft survival rates.
Macroscopic measurements showed no statistically significant differences between groups.
Abstract
The use of fat grafts in plastic, reconstructive, and aesthetic surgery has been increasing. Although fat grafting has many advantages, there is limited evidence regarding its survival rates. Current studies focus on improving fat graft survival rates. This study aimed to evaluate the effect of therapeutic ultrasound (TERUS) application on fat graft survival. The study involved 42 adult male Wistar Albino rats, which were randomly divided into seven groups of six rats each: Group 1 served as the control group and received only fat grafting; Group 2 received preoperative daily TERUS for one week, followed by fat grafting; Group 3 underwent preoperative daily massage for one week, followed by fat grafting; Group 4 received preoperative daily TERUS for one week, followed by fat grafting and postoperative daily TERUS for one week; Group 5 underwent preoperative daily massage for one week,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
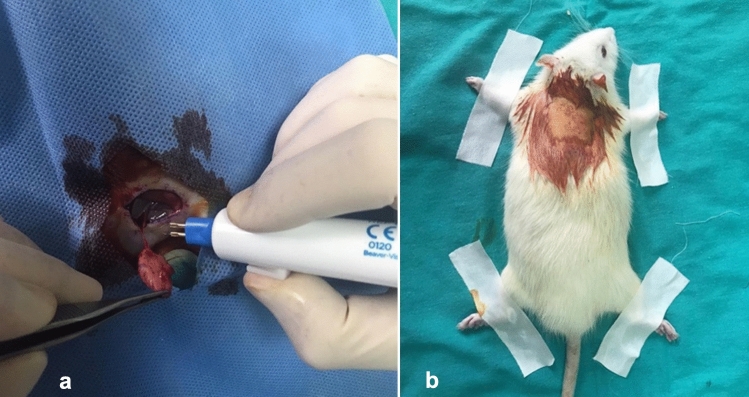 Figure 1
Figure 1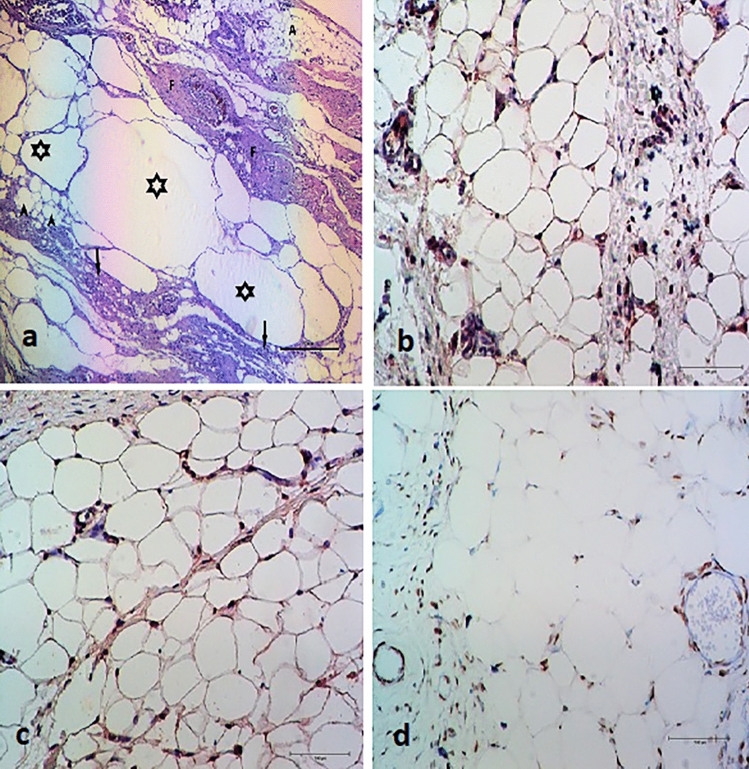 Figure 2
Figure 2- —Afyon Kocatepe University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBody Contouring and Surgery · Mesenchymal stem cell research · Reconstructive Surgery and Microvascular Techniques
Introduction
Fat grafting is a widely utilized technique in plastic, aesthetic, and reconstructive surgery and has seen increasing popularity in recent years. It has various indications, including volume restoration for facial depressions and age-related changes for aesthetic purposes, volume augmentation in breast reconstruction following cancer surgery, and scar tissue regeneration due to its stem cell content [1].
The viability of fat grafts is highly variable across applications. Since the first use of fat grafting in the 1890s, there has been growing interest in improving graft viability through advancements in technology and medicine [2]. Many methods have been explored, including the use of endogenous substances such as platelet-rich plasma, growth factors (e.g., epidermal growth factor) and vascular endothelial growth factor, exogenous substances (e.g., botulinum toxin), and preconditioning of the recipient field; however, no universally accepted consensus has yet been established [3–6].
Preconditioning refers to any procedure performed to increase the success of an operation and is commonly employed in flap surgeries. It can involve botulinum toxin injection, invasive methods such as microporation, or non-invasive approaches such as therapeutic ultrasound (TERUS) [4, 6–9]. TERUS is a device used in physical therapy and rehabilitation to provide deep tissue heating. Studies have demonstrated that TERUS decreases inflammation and increases blood flow in the treated area. By increasing cell membrane permeability,
TERUS facilitates the diffusion of extracellular calcium ions into cells [10]. In addition, TERUS can decrease fat tissue and tighten skin by stimulating collagen synthesis when used at variable intensities [11–13]. It has also been employed in various animal studies focusing on tendon healing, scar healing, and enhancing the viability of skin flaps [9, 14, 15].
This study aimed to investigate the effect of TERUS on fat graft viability, considering its potential to reduce inflammation and increase vascularity.
Materials and Methods
Animals
This study was conducted with the approval of Afyon Kocatepe. The experiment complied with European Union Directive 2010/63/EU for the Protection of Experimental Animals and the regulations of the Afyon Kocatepe University Experimental Animals Ethics Committee. All applicable institutional and/or national guidelines for the care and use of animals were followed.
The study was designed as a single-blind randomized trial. Forty-two adult male Wistar Albino rats, with an average weight of 256.9 ± 54.4 g, were used in the study. Animals weighing less than 200 g and more than 500 g were excluded. The animals were housed individually in standard cages under controlled environmental conditions and provided with free access to standard pellet food and water.
Experimental Groups
The animals were randomly divided into seven groups, with six rats in each group:
Group 1: Control (only fat grafting).
Group 2: Daily TERUS application with the device on for one week prior to surgery, followed by fat grafting.
Group 3: Daily massage using the TERUS probe (device off) for one week prior to fat grafting.
Group 4: Daily TERUS application for one week preoperatively, followed by fat grafting and an additional week of daily TERUS postoperatively.
Group 5: Daily massage using the TERUS probe (device off) for one week preoperatively, followed by fat grafting and an additional week of daily massage postoperatively.
Group 6: Daily TERUS application with the device on for one week postoperatively after fat grafting.
Group 7: Daily massage using the TERUS probe (device off) for one week postoperatively after fat grafting.
In Groups 3, 5, and 7, the handpiece of the TERUS device was used to evaluate the massage effect. For standardization purposes, daily massage was performed with the TERUS device turned off. These groups were formed with the aim of assessing the massage effect of the ultrasound probe.
For all groups, the donor area was the right inguinal region, and the recipient site was the subcutaneous tissue of the parascapular region.
Surgical Procedures
The surgical procedures were performed as described by Temiz et al. [16]. After shaving the hair in the surgical area, disinfecting with povidone iodine (Batikon-Genesis Ilac A.S.), and covering the site with sterile blue scrubs, the rats were secured with tape. Under general anesthesia (50 mg/kg ketamine (Ketalar-Pfizer Inc.) and 5 mg/kg xylazine (Rompun® 2%, Bayer Türk Kimya Sanayi Ltd. Sti., Istanbul, Turkey), fat grafts were harvested from the right inguinal fat pad and implanted into the subcutaneous tissue of the parascapular region, superficial to the muscle fascia. The rats were positioned supine, with their extremities fixed. A parallel incision was made along the inguinal ligament, and blunt dissection was used to expose the femoral peduncle. The fat graft was dissected from the surrounding tissues (Fig. 1a). The epigastric artery and vein were identified and cauterized to isolate the fat tissue. The weight of the graft was measured, and its volume was calculated using Archimedes’ principle. The grafts were kept in wet gauze. The incision in the inguinal region was closed with absorbable sutures.Fig. 1a. Inguinal fat graft excision, b. fat graft implantation area in the parascapular region.
The rats were then positioned prone, and their extremities were fixed to prepare the recipient region. After disinfection, a 1.5-cm skin incision was made in the parascapular region, and sufficient subcutaneous tissue was dissected to insert a 1.5x1.5-cm sterile silicon layer (Fig. 1b). The silicone layer was used to ensure equal and standardized subcutaneous dissection in all subjects. After removing the silicone layer, the fat graft was inserted into the prepared subcutaneous pouch, and the skin incision was closed. The rats were returned to their cages for rest and recovery.
At the end of the eight-week follow-up period, general anesthesia was administered again. The rats were placed in the prone position, and the dorsal interscapular region was shaved. After disinfecting the site with povidone iodine, a 1.5-cm skin incision was made in the parascapular region, and the fat grafts were excised. Following the completion of all surgical procedures, the rats were sacrificed in accordance with ethical regulations.
TERUS Application
Before applying TERUS, the size and shape of the ultrasound handpiece were traced onto plaster, which was then was cut to match the shape. TERUS was applied to the recipient area of each rat using the BTL-4000 device (Smart & Premium, BTL Türkiye, Ankara, Turkey). The dorsum of the animals was shaved to match the shape of the cut plaster, and the area where the ultrasound probe would be applied was marked with a pen. TERUS was applied to the marked dorsal region in a circular motion without exerting pressure on the skin. The application was performed with an intensity of 1 W/cm^2^, a carrier frequency of 3 MHz, and a duty factor of 100%. In the massage groups, the massage effect was investigated using the same circular motions but with the device turned off.
Histopathological Analysis
The fat tissues obtained were fixed in 10% neutral formalin for four days. After fixation, the tissues were labeled and washed under running water for one day. The samples were subsequently kept in 70%, 80%, 90%, and pure alcohol solutions in sequence. Next, they were immersed in a xylene + alcohol mixture for 45 minutes, followed by two separate immersions in xylene for 45 minutes each. The samples were then infiltrated with liquid paraffin for one hour and embedded in paraffin blocks. From these blocks, 5-micron-thick slices were sectioned. The slices were mounted onto ordinary slides for routine examination and onto slides coated with polylysine for immunohistochemical examination. The slices on ordinary slides were stained with hematoxylin–eosin (HE) after deparaffinization. Slides with polylysine were stained with perilipin (bs-3789R 1/50), PECAM-1 (H-3) (sc-376764, 1/100) antibodies after deparaffinization. The slides were examined under a light microscope.
To evaluate apoptosis, additional 5-micron-thick slices were mounted onto polylysine slides and stained using the TUNEL method, following the protocol of the ApopTag® Plus Peroxidase In Situ Apoptosis Kit (S7101). These slides were also examined under a light microscope.
The slices stained with HE were scored histopathologically. Cyst formation, inflammation, and fibrosis were evaluated under a light microscope at 10x magnification, and a score was assigned based on the severity of the changes observed: 0 = no change, 1 = minimal, 2 = minimal to moderate, 3 = moderate, and 4 = moderate to severe. The data were subsequently analyzed statistically.
For image analysis, the Nikon NIS 4.2 Image Analysis Software was used. The HE-stained samples were examined at 10x magnification using a Nikon E-60 light microscope. An H-score was used to evaluate the immunohistochemically stained samples. Fat cells were counted in every sample under 20x magnification, with a total of 500 fat cells counted per sample. The cells were categorized as +1, +2, or +3 based on staining intensity, while unstained cells were assigned a score of 0.
The H-score was calculated using the formula: H-score = (I + 1) × number of stained cells [17].
The weights and volumes of the rats and fat grafts were measured and statistically analyzed according to the formulas provided below.
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$${\text{Percentage of fat graft survival}} = \frac{{{\text{Volume of fat graft excised at week eighth}}}}{{{\text{volume of fat graft at the beginning}}}} \times {\text{100}}.$$\end{document} \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\frac{{{\text{Volume}}}}{{{\text{Weight}}}}{\text{change}\, \text{percentage}} = \frac{{\left( {{\text{last}}\frac{{{\text{volume}}}}{{{\text{weight}}}}} \right) - \left( {{\text{first}}\frac{{{\text{volume}}}}{{{\text{weight}}}}} \right)}}{{{\text{first}}\frac{{{\text{volume}}}}{{{\text{weight}}}}}} \times 100$$\end{document} \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$${\text{Change in weight percentages of rats}} = \frac{{\text{last weight - first weight}}}{{\text{first weight}}} \times 100$$\end{document}Statistical Analysis
Data were analyzed using IBM SPSS Program version 21.0 (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. New York, USA). The conformity of the data to the normal distribution was evaluated using the Shapiro–Wilk test and Q–Q graphics, while the Levene test was used to evaluate variance homogeneity. One-way analysis of variance (ANOVA) was used for intergroup comparisons meeting parametric assumptions. Welch’s ANOVA was applied for non-normally distributed data. Tukey HSD test was used for multiple group comparisons. Crosstabs and Chi-square tests were used for qualitative variable comparisons. Statistical significance was set at p < 0.05 in all tests.
Results
Macroscopic Findings
Two rats died due to anesthesia complications and were excluded from the study. No complications, such as infection, abscess, hematoma, or seroma, were observed. The overall results for the rats and grafts are listed in Table 1.Table 1. Overall results of the rats and graftsnMinimumMaximumMeanStd. DeviationPreop rat weight (g)40190.20464.00256.961154.40071Preop fat graft volume (cc)40.21.80.5378.13076Preop fat graft weight (g)40.30.81.5025.14528Postop rat weight (g)40298.68485.20359.214247.28509Postop fat graft volume (cc)40.12.45.2864.07522Postop fat graft weight (g)40.12.41.2431.06391Cysts40.004.001.91671.31747Fibrosis401.004.002.0833.87423Inflammation401.004.002.1667.91026Perilipin40143.00323.00234.750052.90713PECAM CD3140149.00302.00219.666742.04827TUNEL40196.00321.00274.400036.71713Fat graft survival percentage4022.22100.0055.820117.78145Fat graft volume/weight change percentage40− 57.50112.5013.506032.93991Rat weight change percentage404.5768.9242.048916.36281Valid n (listwise)40Abbreviations: preop: preoperative, postop: postoperative
There was no statistically significant difference in the average volume/weight change percentages between the groups (p = 0.614). Similarly, no statistically significant difference was observed in the average fat graft survival percentages between the groups (p = 0.451). There was also no statistically significant difference in the weight percentages of the groups (p = 0.311) (Table 2).Table 2. Comparative results of variablesSum of squaresdfMean squareFSig.Preop rat weightBetween groups27593.53464598.9221.755.144Within groups75986.762292620.233Total103580.29635Preop fat graft volumeBetween groups.0416.007.352.903Within groups.55829.019Total.59835Preop fat graft weightBetween groups.0536.009.374.889Within groups.68629.024Total.73935Postop rat weightBetween groups9758.81561626.469.689.660Within groups68496.984292361.965Total78255.79935Postop fat graft volumeBetween groups.0106.002.253.954Within groups.18829.006Total.19835Postop fat graft weightBetween groups.0076.001.264.949Within groups.13629.005Total.14335CystsBetween groups16.21762.7031.760.143Within groups44.533291.536Total60.75035FibrosisBetween groups7.91761.3192.032.093Within groups18.83329.649Total26.75035InflammationBetween groups8.86761.4782.129.080Within groups20.13329.694Total29.00035PerilipinBetween groups76600.617612766.76917.325**.000Within groups21370.13329736.901Total97970.75035PECAM CD31Between groups38484.90066414.1507.950.000Within groups23397.10029806.797Total61882.00035TUNELBetween groups19318.30063219.7176.648.002**Within groups6296.50013484.346Total25614.80019Fat graft survival percentageBetween groups1879.4916313.248.989.451Within groups9186.80729316.786Total11066.29835Fat graft volume/weight change percentageBetween groups5108.4126851.402.751.614Within groups32867.902291133.376Total37976.31435Rat weight change percentageBetween groups1924.9606320.8271.250.311Within groups7445.99129256.758Total9370.95035Abbreviations: Preop: preoperative, postop: postoperative, df: degrees of freedom, sig: significance
Histological and Immunohistochemical Findings
No statistically significant correlation was found between cyst formation and fibrosis (p = 0.361) or between cyst formation and inflammation (p = 0.347) across the groups. In addition, there were no statistically significant differences among the groups regarding cyst formation (p = 0.199), fibrosis (p = 0.070), or inflammation (p = 0.318) (Fig. 2, Table 2).Fig. 2. Staining of the excised fat graft,** a**. hematoxylin–eosin,** b**. PECAM,** c**. perilipin,** d**. TUNEL. (asterisk: fat cysts, arrowheads: fat vacuoles, arrows: mononuclear cells, F: areas of fibrosis, A: nucleated live adipocytes)
Statistically significant differences were observed between the groups in the average PECAM values (p < 0.001). This difference was specifically noted between the following group comparisons: Groups 1 vs. 3 (p < 0.001), Groups 1 vs. 4 (p < 0.001), Groups 2 vs. 4 (p = 0.014), Groups 3 vs. 6 (p = 0.022), and Groups 4 vs. 6 (p = 0.002). There were also statistically significant differences in the perilipin averages of the groups (p < 0.001) (Table 3). This difference was noted in the following group comparisons: Groups 1 vs. 3 (p < 0.001), Groups 1 vs. 5 (p < 0.001), Groups 1 vs. 7 (p < 0.001), Groups 2 vs. 5 (p < 0.001), Groups 2 vs. 7 (p < 0.001), Groups 3 vs. 6 (p < 0.001), Groups 4 vs. 5 (p = 0.002), Groups 4 vs. 7 (p = 0.001), Groups 5 vs. 6 (p < 0.001), and Groups 6 vs. 7 (p < 0.001) (Table 3).Table 3PECAM and perilipin percentages of the groupsPECAM percentages (%)Group 1Group 2Group 3Group 4Group 5Group 6Group 7P valuen5566666Mean ± SD168.0206.0252.50272.40220.60192.0219.60±15.19±30.53±38.20±23.13±39.29±17.11±22.10<0.001Min-Max149.0168.0208.0248.0171.0168.0199.0− 189.0− 239.0− 295.0− 302.0− 269.0− 209.0− 255.0Perilipin percentages (%)Mean ± SD178.60212.80258.67217.80294178.40298.20<0.001±20.59±34.71±32.53±28.65±25.9±25.89±16.22Min-Max143.0159.0212.0172.0255.0151.0273.0− 193.0− 249.0− 301.0− 242.0− 323.0218.0316.0SD: standard deviation
Lastly, no statistically significant correlation was observed between perilipin and PECAM variables across the groups (r = 0.3202, p = 0.057). Similarly, there was no statistically significant correlation between perilipin and TUNEL variables across the groups (r = 0.3853, p = 0.093).
Disussion
Fat grafts are increasingly used in plastic, aesthetic, and reconstructive surgery. Their advantages include low cost, easy accessibility, and biocompatibility. However, they also have major disadvantages, such as varying survival rates and unpredictable postoperative volumes [1, 3].
Several factors affect fat graft viability. The amount of viable fat cells at the time of graft transfer and the vascularity of the donor site significantly impact graft survival. Sezgin et al. preconditioned the fat graft donor areas of rats with microneedling, which increased tissue perfusion. The authors demonstrated longer survival of fat grafts in areas preconditioned by microneedling [4]. In light of this study, we utilized TERUS as a preconditioning method to increase the fat graft survival, as TERUS enhances tissue vascularity. While TERUS did increase vascularity in our study, fat graft survival was decreased in Groups 4 and 6. We attributed this outcome to the fat melting effect of TERUS, consistent with findings from the study conducted by Zhou et al. [18].
An ischemic flap model in rats was designed in a study by Yücel et al., which showed that TERUS reduced flap necrosis by increasing vascularity [9]. Our study investigated fat graft survival in rats preconditioned with TERUS. Based on data gathered, a correlation was identified between increased PECAM values in Groups 2, 4, and 6 and enhanced vascularity due to TERUS. This vascularity increase aligns with findings in the existing literature [19].
TERUS has been shown to reduce fat tissue and tighten skin by stimulating collagen synthesis when used at variable intensities. Both its thermal and non-thermal effects contribute to fat tissue reduction. The thermal effect of TERUS decreases fat tissue through coagulation necrosis [11–13]. Previous studies have demonstrated fat tissue reduction with TERUS-like ultrasonographic devices [12]. In our study, despite the increase in vascularity indicated by PECAM values, a significant increase in live fat tissue was not observed. Our findings on fat tissue are consistent with the literature [18].
Both massage groups and TERUS groups were shown to have increased vascularity in a study by Noble et al. [20]. In our study, the vascularity increase observed in TERUS device-off groups was attributed to the massage effect. In addition, an increase in perilipin levels in TERUS device-off groups was associated with increased vascularity. However, Park et al. reported that endothelial progenitor cells migrated to ischemic tissue and initiated neovascularization, forming vascular cords by the 14th day and fully functional vessels by the 21st day [21]. In our study, although an increase in vascularity was observed histopathologically, a decrease in fat graft viability was determined. This reduction may be due to the non-functionality of the new vessels and the use and duration of TERUS.
Conclusion
In this study, we investigated the effect of TERUS on fat graft survival. TERUS application was shown to increase vascularity; however, it also reduced fat graft volume, negatively affecting fat graft survival. We consider that the decrease in fat graft survival in the group with postoperative TERUS was due to the diminishing effect of this application on fat tissue. Preconditioning with TERUS can be used to enhance vascularity in fat graft operations, but its postoperative use decreases fat graft survival. We also observed that fat graft survival improved with massage application, as significant differences were observed between the control and massage groups. Further studies on TERUS and fat grafts are necessary, particularly with larger sample sizes.