Incidence and Prevalence of Childhood Atopic Diseases in Dutch Primary Care
W. Kuan Chung, Evelien I. T. de Schepper, Laura Struik, Madelon van Tilborg‐den Boeft, Arthur Bohnen, Patrick J. E. Bindels, Evelien R. van Meel

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
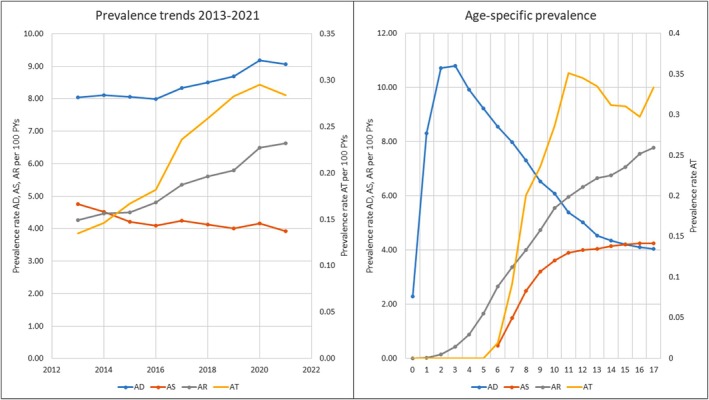 FIGURE 1
FIGURE 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAsthma and respiratory diseases · Pediatric health and respiratory diseases · Dermatology and Skin Diseases
Summary
- The prevalence of allergic rhinoconjunctivitis diagnosis and the atopic triad have increased over time.
- Improved recognition of atopic patients in primary care is needed for optimal disease management.
To the Editor,
Atopic diseases, including atopic dermatitis (AD), asthma and allergic rhinoconjunctivitis (AR), are common childhood conditions [1, 2, 3]. Although studies in open populations (via general population‐based surveys) suggest varying prevalence trends, physician‐diagnosed rates in primary care remain underexplored. Recent literature questions the assumption of an increase in atopic disease prevalence, emphasising shifts in increased disease awareness rather than true epidemiological changes [2, 4, 5]. This study examines the prevalence and incidence of atopic diseases in children within the Rijnmond Primary Care Database (RPCD) [6], including children with the atopic triad—that is, children who have been diagnosed with AD, asthma and AR at any time during childhood.
We conducted a retrospective cohort study using RPCD, a regional database covering over 500,000 primary care patients from 240 general practices in Rotterdam–Rijnmond, the Netherlands. We included children aged 0–18 years from 2013 to 2021. Atopic diseases were identified using International Classification for Primary Care (ICPC) codes combined with pharmaceutical prescription data utilising the Anatomical Therapeutic Chemical (ATC) codes. Additional study methods, including the relevant ICPC and ATC codes for case selection, and results are available in the Open Science Framework online repository: https://osf.io/4kwb2/?view_only=959223bea5534b31aef5c84e5ac6c13d.
AD and asthma were defined as at least two consultations and two prescriptions, while AR required two consultations plus either two prescriptions or a positive radioallergosorbent test (RAST). A case was considered resolved if no further ICPC or ATC records appeared for 2 years.
We analysed data from 66,382 children in 2021, of whom 22,123 had AD, asthma or AR. Median follow‐up time was 3.34 years. The incidence rates for AD and asthma remained stable over time, while AR increased from 0.89 to 1.48 per 100 PYs (p < 0.001). Corresponding prevalence rates for AR rose from 4.26 to 6.62 per 100 PYs (p < 0.001). The prevalence of the atopic triad also increased from 0.14 to 0.28 per 100 PYs (p < 0.001). The prevalence rates for all atopic diseases and the age‐specific prevalence rates are displayed in Figure 1.
The prevalence rates from 2013 to 2021 and age‐specific prevalence rates for all atopic diseases. In both charts, the Y‐axis on the left displays the prevalence rate per 100 PYs for AD, AS and AR, while the y‐axis on the right displays the prevalence rate of AT. In the upper panel, the X‐axis shows the chronological time in years. In the lower panel, the X‐axis shows the patients age in years. AD, Atopic dermatitis; AR, Allergic rhinoconjunctivitis; AS, Asthma; AT, Atopic triad; PYs, Patient years.
Age‐specific analysis (Figure 1) showed peak prevalence for AD at 3 years (median onset: 2.9 years, IQR: 1.0–7.6), asthma at 17 years (median onset: 9.6 years, IQR: 7.6–12.5) and AR at 17 years (median onset: 10.3 years, IQR: 7.3–13.6). The atopic triad peaked at age 11 (0.35 per 100 PYs, 95% CI: 0.28–0.43).
Sex‐specific analysis revealed that AD was more common in boys until age five, after which it became more prevalent in girls. Asthma and AR were more frequent in boys throughout the whole childhood. The atopic triad was more prevalent in boys (0.25 per 100 PYs) than in girls (0.19 per 100 PYs), with peak rates at age 11 for boys (0.41 per 100 PYs, 95% CI: 0.31–0.53) and age 17 for girls (0.34 per 100 PYs, 95% CI: 0.25–0.46).
Our findings indicate stable incidence and prevalence rates for AD and asthma between 2013 and 2021, while AR and the atopic triad prevalence increased. This may be due to previous underdiagnosis, increased physician awareness and environmental factors. Although we did not observe any decrease in prevalence rates during the COVID‐19 pandemic, the impact of COVID‐19 restrictions on healthcare utilisation during 2020–2021 should be considered when interpreting trends. Asthma, AR and AT were more prevalent in boys throughout childhood, whereas AD was initially more common in boys but later in girls after age 13. The atopic triad prevalence was three times higher than expected by chance, supporting findings of distinct atopic disease trajectories. Sex differences align with existing literature, suggesting hormonal and environmental factors contribute to disease persistence [7, 8].
A major strength of our study is the large sample size of the RPCD, which contains data from more than 500,000 primary care patients. However, limitations inherent to database research must be considered. Our study outcomes rely on ICPC and ATC codes, which are subject to individual GP coding variability. While overestimation is minimised by requiring multiple consultations and prescriptions, underestimation may occur in milder cases that require less healthcare. Additionally, disease duration might be underestimated for children with mild symptoms whose cases close after 2 years without follow‐up consultations. Despite this, our estimates align with previous primary care research [9]. Another limitation is the absence of data on ethnicity, family history and environmental exposures such as pets or secondhand smoke. Finally, food allergy could not be studied due to the lack of a specific ICPC code, restricting our focus to the atopic triad of AD, asthma and AR.
In conclusion, the prevalence of AR and the atopic triad is rising in primary care, while AD and asthma did not increase and remained stable. Primary care physicians play a crucial role in identifying atopic children early and ensuring appropriate treatment strategies, including emollient therapy, corticosteroids and lifestyle modifications. Further research is needed to explore risk factors and trajectories in primary care populations.
Author Contributions
W. Kuan Chung conceptualised this study, performed the extraction, analysis and interpretation of the data and drafted and revised the manuscript. Evelien R. van Meel, Evelien I. T. de Schepper, Madelon van Tilborg‐den Boeft, Arthur Bohnen and Patrick J. E. Bindels were involved in conceptualising the study, data interpretation and critically reviewing the manuscript. Laura Struik performed the data extraction. All authors read and approved the final submitted manuscript and agree to be accountable for all aspects of the work.
Ethics Statement
The study (project number 2021‐027) was approved by the Governance Board of RPCD.
Consent
Patient data are de‐identified; therefore, no patient consent was required.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. I. Asher , C. E. Rutter , K. Bissell , et al., “Worldwide Trends in the Burden of Asthma Symptoms in School‐Aged Children: Global Asthma Network Phase I Cross‐Sectional Study,” Lancet 398, no. 10311 (2021): 1569–1580.34755626 10.1016/S 0140-6736(21)01450-1PMC 8573635 · doi ↗ · pubmed ↗
- 2D. P. Strachan , C. E. Rutter , M. I. Asher , et al., “Worldwide Time Trends in Prevalence of Symptoms of Rhinoconjunctivitis in Children: Global Asthma Network Phase I,” Pediatric Allergy and Immunology 33, no. 1 (2022): e 13656.34453861 10.1111/pai.13656 PMC 9012331 · doi ↗ · pubmed ↗
- 3S. M. Langan , A. R. Mulick , C. E. Rutter , et al., “Trends in Eczema Prevalence in Children and Adolescents: A Global Asthma Network Phase I Study,” Clinical and Experimental Allergy 53, no. 3 (2023): 337–352, 10.1111/cea.14276. · doi ↗
- 4A. Volke , K. Toompere , K.‐T. Laisaar , et al., “12‐Month Prevalence of Atopic Dermatitis in Resource‐Rich Countries: A Systematic Review and Meta‐Analysis,” Scientific Reports 12, no. 1 (2022): 15125.36068263 10.1038/s 41598-022-19508-7PMC 9448775 · doi ↗ · pubmed ↗
- 5M. I. Asher , L. García‐Marcos , N. E. Pearce , and D. P. Strachan , “Trends in Worldwide Asthma Prevalence,” European Respiratory Journal 56, no. 6 (2020): 2002094.32972987 10.1183/13993003.02094-2020 · doi ↗ · pubmed ↗
- 6M. A. J. de Ridder , M. de Wilde , C. Ben , et al., “Data Resource Profile: The Integrated Primary Care Information (IPCI) Database, the Netherlands,” International Journal of Epidemiology 51, no. 6 (2022): e 314–e 323, 10.1093/ije/dyac 026.35182144 PMC 9749682 · doi ↗ · pubmed ↗
- 7M. Fröhlich , M. Pinart , T. Keller , et al., “Is There a Sex‐Shift in Prevalence of Allergic Rhinitis and Comorbid Asthma From Childhood to Adulthood? A Meta‐Analysis,” Clinical and Translational Allergy 7 (2017): 44, 10.1186/s 13601-017-0176-5.29225773 PMC 5715620 · doi ↗ · pubmed ↗
- 8J. P. Kim , L. X. Chao , E. L. Simpson , and J. I. Silverberg , “Persistence of Atopic Dermatitis (AD): A Systematic Review and Meta‐Analysis,” Journal of the American Academy of Dermatology 75, no. 4 (2016): 681–687.e 11, 10.1016/j.jaad.2016.05.028.27544489 PMC 5216177 · doi ↗ · pubmed ↗