Intraoperative closure of a large colonic perforation using dual adjustable instrument and channel endoscopy
Kazuya Sumi, Yuki Kawasaki, Hisaki Kato, Taro Tanabe, Masayuki Isozaki, Noboru Yokoyama, Haruhiro Inoue

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
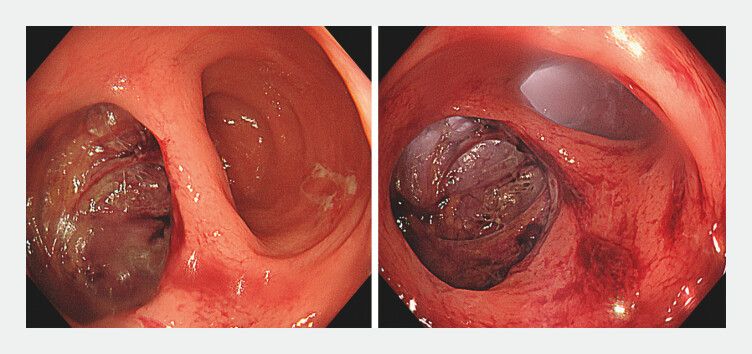 Fig. 1
Fig. 1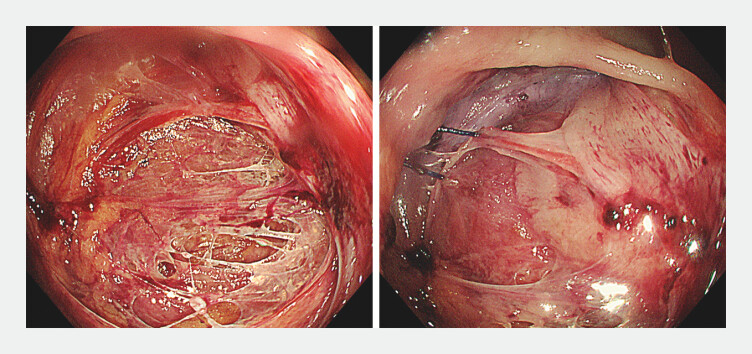 Fig. 2
Fig. 2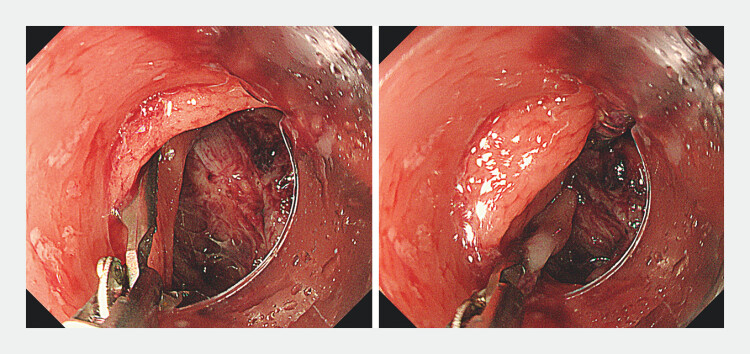 Fig. 3
Fig. 3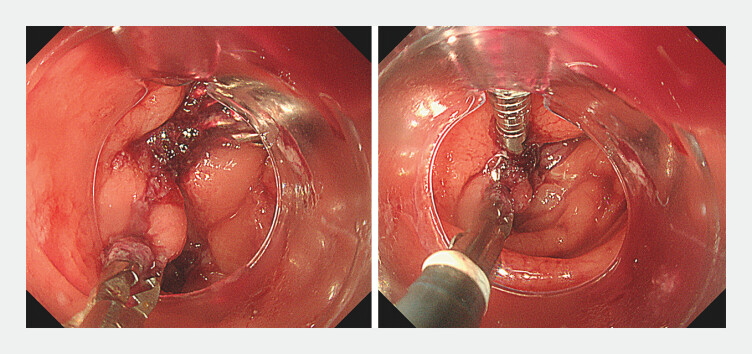 Fig. 4
Fig. 4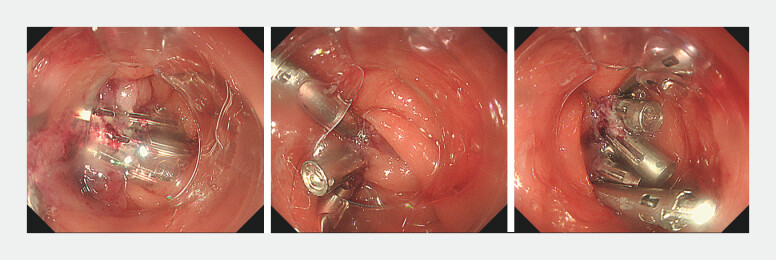 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Diverticular Disease and Complications · Colorectal Cancer Surgical Treatments
Various techniques have been reported for closing perforations and defects following endoscopic procedures 1 2 3 4 5 , with dual-channel endoscopy being one of them. However, its availability is limited, and the fixed orientation of the forceps channel restricts its flexibility. Dual adjustable instrument and channel endoscopy (DAICE) is a novel approach for closing large defects. DAICE converts the standard endoscope into an adjustable dual-channel system with an external channel hood (ECH; Top Corporation, Tokyo, Japan) aligned to the defect.
A woman in her 60s who had undergone the Hartmann’s procedure for sigmoid colon diverticular perforation was admitted for colostomy closure and anastomosis. A full-thickness upper rectal tear on the mesenteric side was noted during transanal anastomosis ( Fig. 1 ). Given the anatomical location, direct surgical closure was deemed technically unfeasible ( Fig. 2 ). Consequently, intraoperative endoscopic closure was planned.
A defect comparable in size to the colon lumen was noted.
Surgical closure was attempted but ultimately could not be performed. The sutures used during the procedure were found.
Closure with an over-the-scope clip was not feasible owing to the large defect size and the fixed channel orientation hindered proper clip engagement on the deeper edge of the defect. To overcome this, DAICE was developed by attaching an ECH to the standard endoscope, allowing positional adjustment. One side of the defect was grasped using a rat tooth forceps and brought closer to the opposite side. The clips were inserted through the external channel, starting from the posterior edge, to close the defect ( Fig. 3 , Fig. 4 ).
An external channel hood was applied to perform dual adjustable instrument and channel endoscopy. One side of the defect was grasped with forceps and brought toward the opposite side, allowing approximation and closure of the defect using clips.
The position of the external channel hood was adjusted to align with the orientation of the closure.
The procedure was completed after confirming no air leaks and complete closure without luminal stenosis ( Fig. 5 , Video 1 ).
The large perforation was successfully closed by dual adjustable instrument and channel endoscopy.
Using an external channel hood and adjusting it to align with the closure (dual adjustable instrument and channel endoscopy), the large surgical perforation was successfully closed endoscopically.Video 1
DAICE is effective for closure, and is versatile and applicable in various scenarios. The 2.8-mm guide tube of the external channel is compatible with a range of devices, enabling its various clinical applications. The ECH can be attached easily, and the procedure can be performed with conventional endoscopes, eliminating the need for dual-channel endoscopy, thereby reducing cost.
Endoscopy_UCTN_Code_CPL_1AJ_2AG
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abe S Saito Y Tanaka YA novel endoscopic hand-suturing technique for defect closure after colorectal endoscopic submucosal dissection: a pilot study Endoscopy 20205278078510.1055/a-1120-853332207119 · doi ↗ · pubmed ↗
- 2Tanabe M Inoue H Shimamura Y Loop 9 closure technique for mucosal defects after colorectal endoscopic submucosal dissection (with video)Endosc Int Open 202412 E 947E 95439131734 10.1055/a-2362-5617 PMC 11309795 · doi ↗ · pubmed ↗
- 3Shiomi D Tanabe M Uragami N Clinical utility of a novel anchor pronged clip for mucosal defect closure after colorectal endoscopic submucosal dissection (with video)Endosc Int Open 202412 E 1127 E 113339398446 10.1055/a-2409-3622 PMC 11466516 · doi ↗ · pubmed ↗
- 4Masunaga T Kato M Sasaki M Modified double-layered suturing for a mucosal defect after colorectal endoscopic submucosal dissection (Origami method) (with video)Gastrointest Endosc 20239796296936642200 10.1016/j.gie.2023.01.005 · doi ↗ · pubmed ↗
- 5Cai Q Zhang L Lan W Twin grasper-assisted endoscopic mucosa-inverting closure for large perforations after endoscopic full-thickness resection: a new endoscopic technique Endoscopy 202254 E 576E 57710.1055/a-1695-301434933359 · doi ↗ · pubmed ↗