Scope withdrawal technique to prevent transesophageal puncture during endoscopic ultrasound-guided hepaticogastrostomy
Kazuki Endo, Haruo Miwa, Ritsuko Oishi, Hiromi Tsuchiya, Yuichi Suzuki, Kazushi Numata, Shin Maeda

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
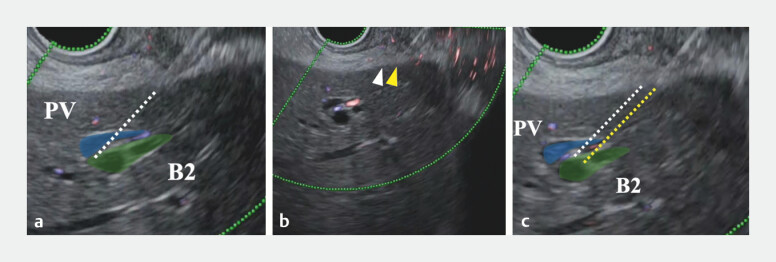 Fig. 1
Fig. 1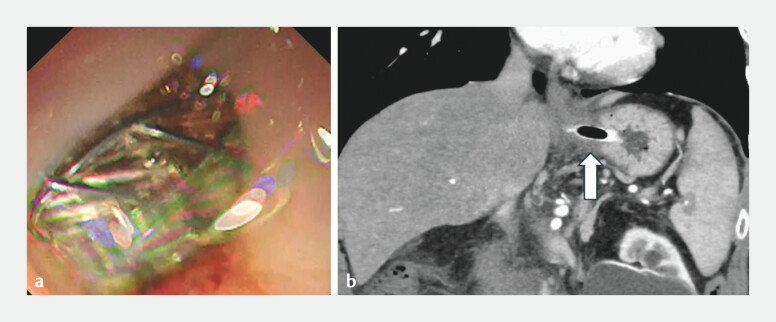 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Gallbladder and Bile Duct Disorders · Pancreatic and Hepatic Oncology Research
In endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS), puncture of the intrahepatic bile duct segment B2 is considered to make guidewire and device insertion easier than B3 puncture. However, B2 puncture carries a risk of esophageal puncture, which can lead to severe complications such as mediastinitis 1 2 . To avoid esophageal puncture, several techniques have been reported 3 4 5 ; however, there are no reports focusing on puncture techniques. Herein, we report a novel puncture technique, termed the “scope withdrawal technique,” to prevent transesophageal puncture during EUS-HGS ( Video 1 ).
Scope withdrawal technique to prevent transesophageal puncture during B2 puncture during endoscopic ultrasound-guided hepaticogastrostomy.Video 1
A 70-year-old man with pancreatic carcinoma was admitted with cholangitis caused by occlusion of a self-expandable metal stent (SEMS) in the common bile duct. Endoscopic retrograde cholangiopancreatography was performed; however, additional SEMS placement failed due to tumor invasion into the duodenum. Endoscopic nasobiliary drainage was initially performed, and EUS-HGS was carried out after the cholangitis improved.
When B2 puncture is attempted, the portal vein may obstruct the puncture route. Withdrawing the scope to avoid the portal vein and target a more peripheral bile duct increases the risk of esophageal puncture. To address this issue, we first punctured the gastric wall slightly distal to the intended puncture line using a 19G fine-needle aspiration needle (EZ Shot 3 Plus; Olympus, Tokyo, Japan). Keeping the needle in place, the scope was withdrawn to adjust the puncture line without changing the needle entry point in the gastric wall ( Fig. 1 ). After B2 puncture and guidewire insertion, a fully covered SEMS (Niti-S EUS-BD system, End Bare Single Flare, 8 mm × 10 cm; Taewoong Medical Co., Ltd., Gimpo, South Korea) was placed. The SEMS was placed just below the esophagogastric junction, and a CT scan on the day after the procedure confirmed transgastric placement ( Fig. 2 ).
Scope withdrawal technique to prevent transesophageal puncture during intrahepatic bile duct segment B2 puncture. a The gastric wall is punctured slightly distal to the intended site, penetrating only the gastric wall and stopping just before reaching the liver surface (white dotted line: puncture line). b The scope is withdrawn while keeping the needle in place (the tip of needle moves from the white arrowhead to the yellow arrowhead). c The puncture line is adjusted from the white to the yellow dotted line without changing the gastric entry point.
The position of the self-expanding metal stent (SEMS) after endoscopic ultrasound-guided hepaticogastrostomy. a The SEMS is placed just below the esophagogastric junction. b A CT scan on the day after the procedure reveals that the SEMS is deployed from the stomach.
To the best of our knowledge, this is the first report of a puncture technique to prevent esophageal puncture during EUS-HGS.
Endoscopy_UCTN_Code_TTT_1AS_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Piraka C Shah RJ Fukami NEUS-guided transesophageal, transgastric, and transcolonic drainage of intra-abdominal fluid collections and abscesses Gastrointest Endosc 20097078679210.1016/j.gie.2009.04.04919577742 · doi ↗ · pubmed ↗
- 2Bohle W Zoller WG Mediastinitis after EUS-FNA in a patient with sarcoidosis – case report with endosonographic features and review of the literature Z Gastroenterol 2014521171117425313629 10.1055/s-0034-1385071 · doi ↗ · pubmed ↗
- 3Morita S Hara K Suda T The use of clip anchoring to ensure safe transgastric puncture during endoscopic ultrasound-guided transmural drainage Endoscopy 201749 E 186E 18728558402 10.1055/s-0043-109428 · doi ↗ · pubmed ↗
- 4Okuno N Hara K Mizuno NB 2 puncture with forward-viewing EUS simplifies EUS-guided hepaticogastrostomy (with video)Endosc Ultrasound 20221131932435848655 10.4103/EUS-D-21-00154 PMC 9526104 · doi ↗ · pubmed ↗
- 5Ishikawa S Hara K Okuno N Safety and efficacy of novel oblique-viewing scope for B 2-endoscopic ultrasound-guided hepaticogastrostomy Clin Endosc 20245752753310.5946/ce.2023.12938549245 PMC 11294849 · doi ↗ · pubmed ↗