Cutaneous metastasis of hepatocellular carcinoma with novel dermoscopic findings
Vixey Silva, Rosemary Oaks, Heather Kopecky, Richard Miller, Brandon Shutty, Jill Browning

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1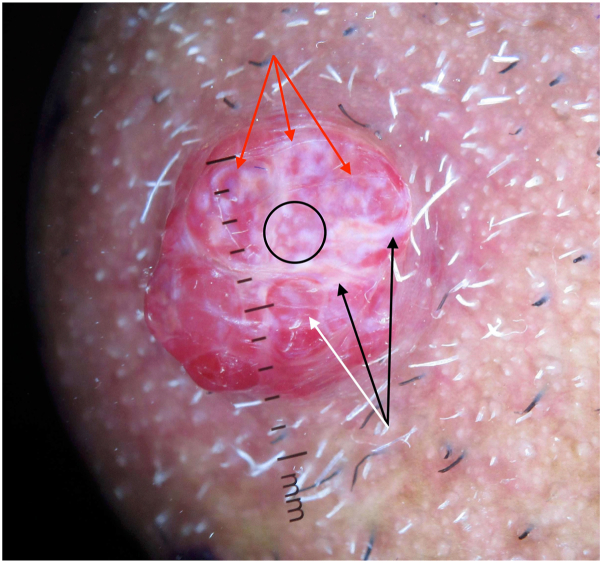 Figure 2
Figure 2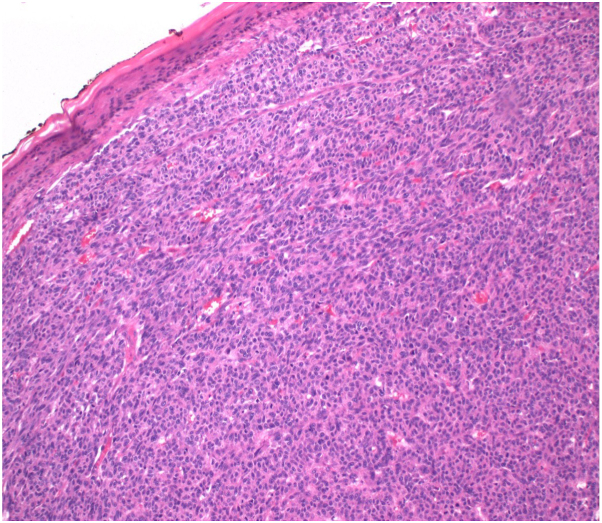 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Diagnosis and Treatment · Cutaneous Melanoma Detection and Management · Genital Health and Disease
Clinical presentation
A 66-year-old man with a history of hepatocellular carcinoma (HCC) and hepatitis B presented with a 2 cm, asymptomatic chin nodule growing rapidly for 2 months (Fig 1).Fig 1. Two centimeter, red, shiny nodule on the left chin.
Dermatoscopic appearance
Dermoscopy showed a diffuse red homogeneous lesion with a white veil, chrysalis-like shiny white lines, white dots, red lacunae, and a skin-colored collarette (Fig 2). A positive rainbow sign was present.Fig 2. Dermoscopic image under polarized light and direct contact showing a red homogeneous lesion with a white veil, multiple chrysalis-like shiny white lines (black arrows), white dots (circled), a positive rainbow sign (red arrows), and a surrounding skin-colored collarette. Red lacunae are also visualized (white arrow).
Histologic diagnosis
Histopathology revealed an atrophic epidermis with effaced rete ridges, islands of eosinophilic cells with pleomorphic nuclei, and numerous vascular spaces with extravasated red blood cells (Fig 3).Key messageCutaneous metastasis of HCC is rare, accounting for less than 0.8% of all cutaneous metastases, but its recognition is crucial for detecting internal malignancy.1 These metastases typically present as firm, painless, red or bluish papules or nodules of varying sizes on the face, scalp, chest, or shoulders, sometimes with ulceration. This case highlights novel dermoscopic findings, including crystalline structures and the rainbow sign, previously unreported in HCC metastases. These unique features, along with red lacunae, white dots, and disorganized vessels, can help differentiate cutaneous HCC metastasis from clinical mimickers such as amelanotic melanoma and vascular tumors (eg, lobular capillary hemangioma). Early recognition and accurate diagnosis are vital, as cutaneous HCC metastasis generally indicates a poor prognosis and necessitates prompt management of both primary and metastatic lesions.2Fig 3. Histopathological image revealing atrophic epidermis with effaced rete ridges, islands of eosinophilic cells with small pleomorphic nuclei, and numerous small vascular spaces.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chernoff K.A.Marghoob A.A.Lacouture M.E.Dermoscopic findings in cutaneous metastases JAMA Dermatol 1504201442943310.1001/jamadermatol.2013.850224430974 · doi ↗ · pubmed ↗
- 2Jia J.Luo J.Zou B.Non-iatrogenic implantation of cutaneous metastasis from hepatocellular carcinoma J Cancer Res Clin Oncol 149420231513151910.1007/s 00432-022-04030-035536361 PMC 11796990 · doi ↗ · pubmed ↗