Strategies for rehabilitation management with implants in patients with down syndrome: a scoping review
Jessika Dethlefs-Canto, Solange Baeza-Vallejos, Daniela Ormeño-Sepúlveda, Alexis Bustos-Ponce

TL;DR
This review explores effective strategies for using dental implants in Down Syndrome patients, emphasizing the need for tailored approaches to improve oral health outcomes.
Contribution
The paper provides evidence-based strategies for implant rehabilitation in Down Syndrome patients, highlighting management and success factors.
Findings
Delayed implant loading (3-12 months) resulted in better outcomes compared to immediate loading.
Overdentures with locator or bar systems were effective and easier to maintain for DS patients.
Clinical success rates were higher in simple cases and lower in studies with multiple implants.
Abstract
Down Syndrome (DS), caused by an extra chromosome 21, has a prevalence of 24.7 per 10,000 live births in Chile, the highest in Latin America. Individuals with DS commonly present orofacial and dental anomalies, complicating oral health management. Many depend on removable prostheses, which represent challenges in hygiene, handling, and adaptation. Dental implants are a promising alternative, offering improved stability and functionality. However, successful rehabilitation requires addressing specific anatomical, physiological, and behavioral considerations. This scoping review compiles evidence-based strategies to guide implant treatment in this population. Registered on the Open Science Framework (https://osf.io/bstwk/), this review followed the PRISMA-ScR protocol, addressing the question: "Which are the management strategies and survival rates of dental implants in patients with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
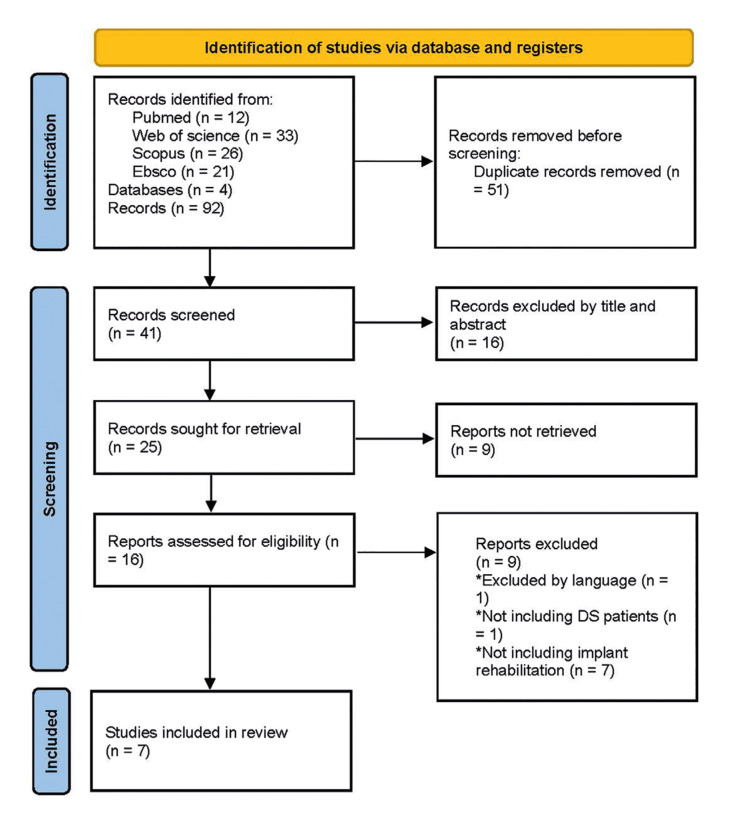 Figure 1
Figure 1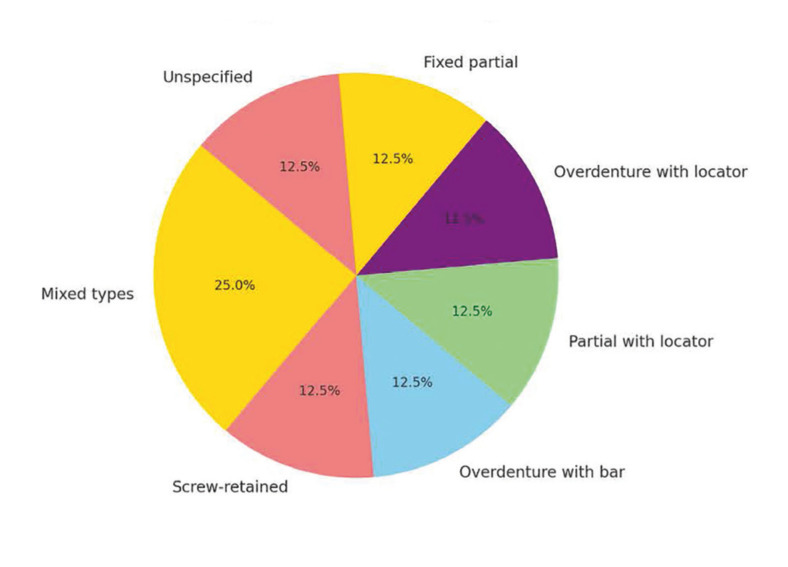 Figure 2
Figure 2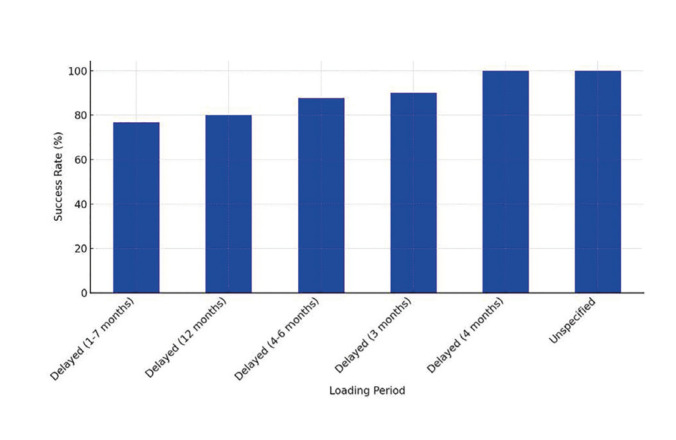 Figure 3
Figure 3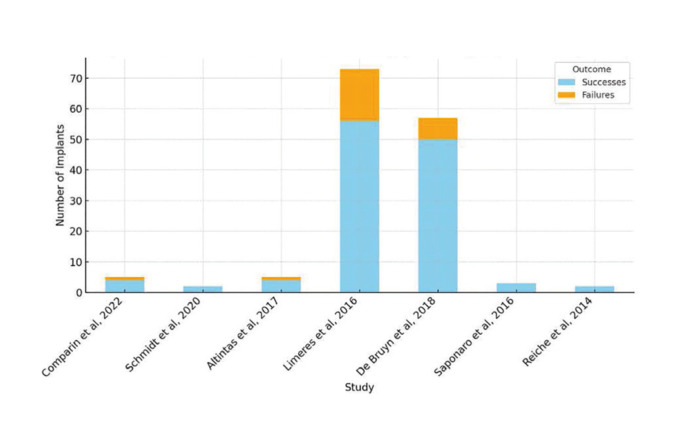 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDisability Education and Employment
Introduction
Down Syndrome (DS) is caused by the presence of an extra chromosome 21, resulting in a series of recognizable clinical characteristics (1). It is the most common cause of intellectual disability of genetic origin, with a prevalence of 1 in 700 live births (2). In Chile, the prevalence of DS is estimated at 26/10,000 births, the highest rate in Latin America (3).
This syndrome presents a wide range of pathologies that affect almost every system in the body, including the cardiovascular, hematological, musculoskeletal, nervous, endocrine, and digestive systems. It is associated with many orofacial and dental alterations, such as hypodontia, malocclusion, bruxism with associated dental wear, reduced vertical dimension, chronic periodontal disease, hypotonic orofacial musculature, reduced salivary flow, and a high incidence of caries. These conditions influence dental treatment, and in many cases, the use of tooth replacements or complete rehabilitations is necessary due to tooth loss or agenesis (4,5).
Most patients with DS successfully use removable dentures, however, some have intellectual disabilities, which can make rehabilitation with removable dentures challenging due to difficulties with hygiene, management, and adaptation. In these cases, fixed dental prostheses provide a rehabilitative alternative, and in some patients, dental implants are the only viable anchorage option (4,6).
Considering the benefits that implant treatment offers as a therapeutic alternative, it is important for professionals to understand the particularities and considerations of these patients. The present review aims to look over the strategies currently used and recommended by professionals in the literature for the management of DS patients with implants, in order to provide considerations that allow dentists to promote the inclusion of individuals with different abilities and their access to the high-quality treatments offered by modern dentistry, especially considering the increase in life expectancy of DS patients over 60 years old.
Material and Methods
The protocol of the present study was based on the framework of Peters et al. according to The Joanna Briggs Institute and is available on the Open Science Framework platform (https://osf.io/kpcm5/). The reporting was based on the PRISMA Extension for Scoping Reviews (PRISMA ScR) (Fig. 1). The PCC question was formulated as follows:
Figure 1PRISMA Flowchart.
-
People: Down Syndrome Patients
-
Concept: Oral Implant Rehabilitation Management Strategies
-
Context: Oral Rehabilitation in disabled patients
According to the research question:
What are the management strategies and survival rates of dental implants in patients with Down syndrome?
The researchers (J.D.; D.O.) conducted a search strategy in parallel and independently on the platforms PubMed, Scopus, Science Direct, and Web of Science. The search terms in titles and abstracts included the terms (dental implant[MeSH Terms]) and ("down syndrome"[MeSH Terms]) using the boolean connector "AND." Obtaining 7 articles in total. Last search was conducted on October 2024.
Inclusion Criteria:
-
Studies in English.
-
Full-text studies published between 2014 and 2024.
-
Case reports.
-
Case series studies (retrospective and cohort) and clinical trials.
-
Studies conducted in patients with down syndrome rehabilitated with dental implants.
Exclusion Criteria:
-
Book chapters.
-
Letters to the editor.
-
Systematic reviews.
Results
- Use of anaesthesia
The use of anaesthesia in patients DS depends on their level of cooperation and the complexity of the procedure. General anaesthesia is common in uncooperative patients or in complex clinical conditions (7,8). On the other hand, local anaesthesia is effective for cooperative patients and simpler procedures (9,10). Sedation is used as an intermediate approach in mixed cases, providing adequate control in specific situations.
- Loading periods
Studies show that delayed loading (between 3 and 12 months) offers better results than immediate loading (9,11) (Fig. 2).
Figure 2. Success Rates by Loading Period.
The study by Comparin et al. (2022) highlights a higher failure rate for immediately loaded implants, underlining the importance of allowing adequate time for osseointegration (7).
- Rehabilitation and prosthetics
Overdentures with locator or bar systems were found to be successful and easier to maintain for both patients and their caregivers. Screw-retained fixed partial dentures offered greater stability, but required rigorous adherence to oral hygiene practices (7,11,12) (Fig. 3).
Figure 3. Prosthetic Type Distribution Among Studies.
- Hygiene strategies and behavioural management
Hygiene education was a key element in preventing peri-implantitis, according to several studies. In addition, the use of behavioural techniques, such as ritualised routines, improved patient cooperation during treatment (9,11).
- Clinical outcomes
Success rates varied significantly according to case complexity and patient compliance (Fig. 4). The highest success rates were reported by Saponaro et al. (2016) and Schmidt et al. (2020), reaching 100% (10,11). On the other hand, studies with higher numbers of implants placed, such as Limeres et al. (2016), showed higher failure rates (2) (Table 1).
Figure 4. Implant Success and Failure Rates Per Study.
Discussion
All the studies refer to implants as a treatment with potential for success and survival. The literature reports success rates of 74-85% (7). Shariq Najeeb et al. (2017) compare the success rate of implants over 10 years, reporting a 96% success rate in the general population. However, in their systematic review, patients with DS show a 26% failure rate at six years, suggesting a higher risk of implant loss in this population. The authors associate these results with studies indicating that patients with DS may have reduced bone density. Therefore, they recommend coating the surface of the implants to improve osseointegration outcomes, which could benefit patients with DS (13). Given that these patients often struggle with removable prostheses due to difficulties in placement, removal, hygiene, limited comfort due to increased lingual pressure, muscle hypotonia, xerostomia, bruxism, and palate characteristics, implants are an option that should be considered and presented as a possibility that not only restores function but also preserves bone (7,12).
The reviewed studies emphasize the importance of providing hygiene instructions to both patients and their caregivers, as well as conducting maintenance sessions to ensure proper hygiene practices. Shariq Najeeb et al. (2017) highlight poor oral hygiene in DS patients, which contributes to implant failure and increased susceptibility to peri-implantitis (13). Corcuera et al. (2016) conducted a study comparing survival rates and marginal bone loss (MBL) in DS patients, patients with cerebral palsy (CP), and those without systemic conditions. They found that the first two groups had higher implant failure rates and MBL, with DS patients showing a greater prevalence of both indicators compared to CP patients. Considering that both conditions are characterized by poor oral hygiene and parafunctional habits, the results suggest that immune deficiencies may play a larger role in implant success. However, the study was conducted on a small population, so larger studies are needed to confirm this correlation (14). These findings are supported by other studies indicating that the etiology of periodontal disease in DS patients differs from those without systemic conditions, suggesting that immune deficiencies contribute to the rapid progression of this disease (12).
Regarding management strategies for implant placement and connection surgeries, most studies highlight the use of general anesthesia. Rehabilitation in the reviewed works was achieved under local anesthesia with protocolized behavioral management techniques. For general anesthesia, prior knowledge of the risks is essential. In DS patients, anesthesiologists must consider occipito-atlanto-axial instability, which occurs in approximately 15% of cases. This instability, caused by joint laxity, skeletal abnormalities, or both, can lead to neurological conditions, including quadriplegia (15). Another technique used in the reviewed literature was intravenous sedation, applied in one study for connection surgery and in another for implant surgery. It is important to note that DS patients are more susceptible to decreases in peripheral oxygen saturation after intravenous sedation (16). Yoshikawa et al. determined that DS patients posed the greatest risk of poor sedation outcomes compared to CP patients and those with intellectual disabilities. Poor oxygenation during sedation is associated with sleep apnea and airway obstruction due to macroglossia, necessitating careful monitoring of these patients (2). Whenever possible, dental treatment should be performed with the patient awake using local anesthesia. However, the decision on the type of anesthesia for each treatment should be individualized, considering the patient’s ability to cooperate (11).
Regarding clinical management of awake patients in the dental chair, only two studies reported strategies for addressing DS patients. Schmidt et al. performed procedures using protocolized behavioral management techniques. These techniques were considered promising due to DS patients need for consistent routines and familiar procedures, which are frequently described as characteristic behaviors in this population. Techniques included voice control, verbal explanations, and presenting materials and instruments (e.g., impression materials and trays) to the patient. Patients were allowed to touch the materials and trays, continuing with these techniques in subsequent sessions (11).
Implants in DS patients were mostly loaded late, varying from 1 to 12 months post-surgery. Not all failed implants were immediate-load, but all attempted immediate-load implants failed. Most implant failures in DS patients occurred during the osseointegration phase. This requires excluding variables such as the time between implant placement and loading, type of prosthetic rehabilitation, tongue pressure on implants, and other factors described in patients with intellectual disabilities, including poor oral hygiene and parafunctional habits like bruxism (2). While some studies have documented immediate loading in DS patients, the data suggest that bruxism may contribute to early failure of immediate-load implants, leading to recommendations to avoid this approach. However, most failures reported by Posse et al. occurred before loading, suggesting other factors at play (13). Baus-Dominguez et al. (2019) found a relationship between MT1 and MT2 genes and implant failure or peri-implantitis. Expression of these genes plays a crucial role in early osteogenic cell differentiation. The authors observed lower expression of these genes in DS patients with failed osseointegration or peri-implantitis compared to those without such issues. This is attributed to reduced metallothioneins, which are critical for antioxidant activity and cell differentiation in new bone formation (4).
In addition, in the case of patients with DS, there are several other aspects that need to be taken into account in the decision process for dental implants. One of these is that the extent of the intellectual disability associated with DS may differ considerably between individuals. This can pose a further challenge in the treatment of these patients. Another important consideration is that, among persons with disabilities, individuals with (12).
This heightened anxiety demands great flexibility on the treating clinician’s part. It is also the reason why it may still be necessary to carry out certain treatment steps, like the insertion of dental implants in combination with other oral surgical measures, under sedation or general anesthesia in patients with Down syndrome, even if the clinician is experienced in behavior management. reclining position on the dental chair, may be found in Windman’s false-alarm theory. According to this theory, in some individuals, the limbic system, which is involved in the pre-attentive processing of stimuli and, thus, also functions as a biologic alarm system, is insufficiently inhibited by higher-order cortical structures. In consequence, the limbic system registers fear too frequently. This also happens in objectively unthreatening “false alarm” situations. Affected individuals may thus perceive a threat and respond with fear even in the absence of objectively threatening stimuli (16).
The degree of intellectual disability in Down syndrome patients is variable, ranging from mild (IQ: 50 to 70) to moderate (IQ: 35 to 50) to severe (IQ: 20 to 35) (12).
The patient had mild mental impairment but was very enthusiastic about dental implants and reported that she wished to be attractive with her new prosthesis (12). In the present report, dental implants were placed under local anesthesia, because the patient had a mild mental disability and was very cooperative during the examinations.
This study has several limitations, including a small sample size and the lack of long-term follow-up data to assess the stability and success of dental implants in Down syndrome (DS) patients. The heterogeneity of the included studies and the limited representation of individuals with severe intellectual disabilities restrict the generalizability of the findings. Additionally, there is a need for research addressing the role of genetic factors, such as the expression of MT1 and MT2 genes, in implant outcomes. Future studies should focus on larger, multicenter cohorts, explore long-term outcomes, and investigate personalized treatment strategies tailored to the varying degrees of intellectual disability. Furthermore, incorporating advanced technologies, evaluating caregiver support, and conducting comparative analyses of implant loading protocols could improve outcomes and enhance the quality of care for this population.
Conclusions
Dental implants are a viable option for patients with Down syndrome (DS), although they have higher failure rates (26% over six years) due to low bone density, poor hygiene and parafunctional habits. Delayed loading has shown better results than immediate loading, and overdentures with locator or bar systems are easier to maintain than screw-retained fixed prostheses, which require strict hygiene.
Clinical management should be adapted to the degree of intellectual disability and consider anaesthetic risks such as occipito-atlanto-axial instability. Hygiene education and caregiver support are essential to prevent complications such as peri-implantitis. An interdisciplinary and personalised approach ensures better functional outcomes and a better quality of life for these patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Antonarakis SE Skotko BG Rafii MS Strydom A Pape SE Bianchi DW Down syndrome Nat Rev Dis Primers 2020693202974310.1038/s 41572-019-0143-7PMC 8428796 · doi ↗ · pubmed ↗
- 2Limeres Posse JLópez Jiménez J Ruiz Villandiego JC Cutando Soriano A Fernández Feijoo J Linazasoro Elorza M Survival of dental implants in patients with Down syndrome: A case series J Prosthet Dent 201611688042746032910.1016/j.prosdent.2016.04.015 · doi ↗ · pubmed ↗
- 3Ojeda ME Moreno R Alta prevalencia de síndrome de Down en el Hospital Regional Rancagua, Chile. Período 1997-2003 Rev Med Chile 200513935421616343210.4067/s 0034-98872005000800010 · doi ↗ · pubmed ↗
- 4Baus Domínguez MGómez Díaz R Corcuera Flores JR Torres Lagares D Ruiz Villandiego JC Machuca Portillo G Metallothioneins in Failure of Dental Implants and Periodontitis Down Syndrome Patients Genes (Basel)2019107113154003710.3390/genes 10090711 PMC 6770985 · doi ↗ · pubmed ↗
- 5Ramakrishnan Sr H Halder S Rustum Baig M Treatment Intricacies in Mandibular Implant-Supported Rehabilitation of a Patient With Down Syndrome: A Clinical Report Cureus 202214 e 311483648389910.7759/cureus.31148 PMC 9724041 · doi ↗ · pubmed ↗
- 6Da Hora Sales PH Pessoa Barros AW Camello de Lima FJ Tavares Carvalho AA Carneiro Leão J Is Down syndrome a risk factor or contraindication for dental implants?. A systematic review J Prosthet Dent 202312953173433277310.1016/j.prosdent.2021.06.031 · doi ↗ · pubmed ↗
- 7Lopes Comparin L Pasquini Filho R Deliberador Tde Souza G Tatim TMüller PR Sinus lift technique and dental implants for rehabilitation for a Down syndrome patient with tomographic 3-years follow-up Spec Care Dentist 202242524303503727110.1111/scd.12697 · doi ↗ · pubmed ↗
- 8De Bruyn H Glibert M Matthijs L Filip M Christiaens V Marks L Clinical Guidelines for Implant Treatment in Patients with Down Syndrome Int J Periodontics Restorative Dent 20193936192959022310.11607/prd.3284 · doi ↗ · pubmed ↗