Granular Cell Tumor of the Colon: A Rare Diagnosis in an Uncommon Location
Saar Peles, Alik Manoogian, Michael Roth, Zachary Field

TL;DR
A rare granular cell tumor in the colon was diagnosed in a 51-year-old woman, highlighting the importance of considering this tumor type in similar cases.
Contribution
This paper presents a rare case of colonic granular cell tumor and emphasizes its diagnostic challenges and management considerations.
Findings
A 10-mm submucosal granular cell tumor was identified in the colon with a yellow-white appearance.
Immunohistochemistry confirmed the diagnosis with strong positivity for S100, SOX10, and inhibin.
The tumor lacked high-risk features but will be monitored for potential malignant transformation.
Abstract
Granular cell tumors (GCTs) are rare neoplasms of Schwann cell origin that typically exhibit benign behavior but can rarely undergo malignant transformation. Gastrointestinal involvement is uncommon, and colonic localization is particularly rare. We report the case of a 51-year-old African American woman referred for evaluation of iron-deficiency anemia. Colonoscopy revealed a 10-mm submucosal lesion at the hepatic flexure with a characteristic yellow-white appearance. Histopathologic examination showed polygonal cells with abundant granular eosinophilic cytoplasm and small, uniform nuclei. Immunohistochemical staining was strongly positive for S100, SOX10, and inhibin, confirming the diagnosis of a GCT. There was no evidence of necrosis or mitotic activity. Although the lesion lacked high-risk histologic features, given the tumor’s submucosal origin and its uncertain malignant…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1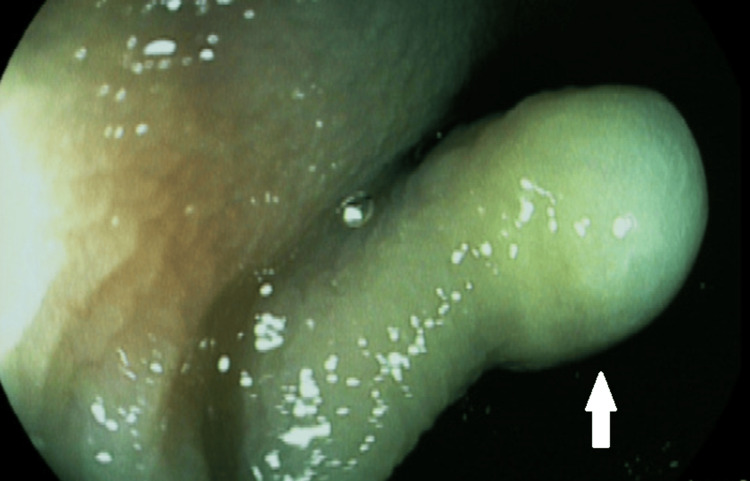 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTumors and Oncological Cases
Introduction
Granular cell tumors (GCTs) are rare neoplasms of Schwann cell origin, characterized by polygonal cells with eosinophilic, granular cytoplasm on electron microscopy and diffuse S100 positivity on immunohistochemistry [1]. While the majority of GCTs are benign, malignant transformation occurs in approximately 1%-2% of cases [2]. These tumors can arise in various anatomical sites, though their occurrence in the gastrointestinal (GI) tract is uncommon. Within the GI tract, they most commonly occur in the esophagus, followed by the stomach and duodenum [1]. Colonic GCTs are exceedingly rare and are most commonly detected incidentally during routine colonoscopy or other screenings [1]. Here we present a rare case of a colonic GCT.
Case presentation
A 51-year-old African American woman with a previous history of menorrhagia presented to a gastroenterology clinic for referral by her hematologist for management and evaluation of iron-deficiency anemia. The patient underwent an esophagogastroduodenoscopy (EGD) and an index colonoscopy, with the EGD notable for mildly atrophic gastric mucosa and an otherwise normal examination. Gastric biopsies were positive for Helicobacter pylori gastritis, and duodenal biopsies were normal. Colonoscopy noted normal terminal ileum, a 5-mm nodule in the cecum (biopsies with submucosal adipose tissue suggestive of submucosal lipoma), a 10-mm nodule at the hepatic flexure (biopsied with cold forceps, indicating GCT in Figures 1, 2), two sessile polyps in the sigmoid colon (hyperplastic polyps), one 6-mm polyp in the rectum (tubular adenoma), and nonbleeding internal hemorrhoids. As shown in Figure 2, the mass did not have any pit patterns under i-SCAN (Pentax Medical, Tokyo, Japan), a software that allows modifications of sharpness, hue, and contrast to enhance mucosal imaging, used in endoscopic studies, indicating that it was not a polyp.
Granular cell tumor seen during colonoscopy
Granular cell tumor under i-SCAN
Immunohistochemical staining was performed to further characterize this cellular proliferation. Discovered on GI stromal tumor 1 was negative, ruling out a GI stromal tumor. Smooth muscle actin was also negative, excluding a leiomyoma. CD68 was negative as well. S100, Sox10, and inhibin immunohistochemical stains were strongly and diffusely positive within the polygonal granular cells, and a diagnosis of GCT was made. No mitotic figures were identified, and there was no necrosis present. While there were no high-risk features present, suggestive of malignancy, because of the diagnostic uncertainty, and as malignant cases appear to be more prevalent in the patient’s demographic of African-American women, the patient and physician did elect to remove the tumor endoscopically.
She was successfully treated with bismuth quadruple therapy and is continuing with oral iron replacement, with plans for endoscopic resection in the near future.
Discussion
GCTs are soft tissue neoplasms thought to arise from Schwann cells and can be found in any part of the body. They most often follow a benign course but may rarely become malignant (1%-2%). They have an abundant eosinophilic cytoplasm and are S100 positive due to their neural origin [1].
Designating GCTs as benign or malignant presents many diagnostic challenges for both gastroenterologists and pathologists. While pathologists may generally categorize GCTs as benign, in daily practice, this becomes more complicated, as GCTs have malignant potential [3]. While tumors with metastasis can be easily classified as malignant, malignancy can be identified without metastases, similarly to other soft tissue tumors. As malignant GCTs are not well understood, this presents challenges in daily practice for managing such tumors.
Fanburg-Smith et al. proposed classifying GCTs based on six histopathological criteria to prognosticate and identify tumors with potentially more aggressive behavior [4]. The six criteria are necrosis, spindling, vesicular nuclei with large nucleoli, increased mitotic activity (>2 mitoses/10 high-power fields at 200× magnification), high nuclear to cytoplasmic (N:C) ratio, and pleomorphism. Neoplasms that display only focal pleomorphism are considered benign; neoplasms that meet one or two criteria are classified as atypical; neoplasms that meet three or more criteria are considered histologically malignant [4]. Some of the proposed criteria, including pleomorphism and an elevated nuclear-to-cytoplasmic ratio, are prone to interobserver variability and demonstrate limited reproducibility among pathologists. This inconsistency can complicate the diagnostic process and blur the distinctions between various diagnostic subgroups. As a result, Nasser et al. attempted to refine the classification criteria based on just two criteria: the presence of necrosis and/or mitosis [5]. While neither of these classification systems has been well validated on a large scale, likely due to the rarity of GCTs, they can be used to prognosticate tumors into lower and higher risk. This is critical, as malignant GCTs have a 60% survival rate within three years, with most cases reported in African-American women [6].
Smaller GCTs have been successfully resected en bloc using endoscopic submucosal resection (ESD) and endoscopic mucosal resection (EMR) [7]. However, endoscopists must keep in mind that, as the name in EMR implies, this technique resects the mucosa, while GCTs originate from the submucosa. As a result, ESD may be a more effective strategy to ensure complete tumor resection. For larger tumors (3-5 cm), endoscopic submucosal excavation has also been used successfully.
Conclusions
GCTs of the colon are an exceptionally rare finding on colonoscopy and often present as small, yellow-white, well-circumscribed, mucosa-covered masses. They are typically benign and asymptomatic but may present with bowel habit changes, hematochezia, or abdominal discomfort. On pathology, they are characterized by polygonal cells with eosinophilic, granular cytoplasm on electron microscopy and diffuse S100 positivity on immunohistochemistry.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Granular cell tumor of the gastrointestinal tract: histologic and immunohistochemical analysis of 98 cases Hum Pathol An S Jang J Min K 8138194620152588292710.1016/j.humpath.2015.02.005 · doi ↗ · pubmed ↗
- 2Granular cell tumors of the esophagus: report of five cases and review of diagnostic and therapeutic techniques Dis Esophagus De Rezende L Lucendo AJ Alvarez-Argüelles H 4364432020071776065910.1111/j.1442-2050.2007.00692.x · doi ↗ · pubmed ↗
- 3Solitary, multiple, benign, atypical, or malignant: the "Granular Cell Tumor" puzzle Virchows Arch Machado I Cruz J Lavernia J Llombart-Bosch A 52753846820162663719910.1007/s 00428-015-1877-6 · doi ↗ · pubmed ↗
- 4Malignant granular cell tumor of soft tissue: diagnostic criteria and clinicopathologic correlation Am J Surg Pathol Fanburg-Smith JC Meis-Kindblom JM Fante R Kindblom LG 779794221998966934110.1097/00000478-199807000-00001 · doi ↗ · pubmed ↗
- 5Malignant granular cell tumor: a look into the diagnostic criteria Pathol Res Pract Nasser H Ahmed Y Szpunar SM Kowalski PJ 16416820720112128201610.1016/j.prp.2010.12.007 · doi ↗ · pubmed ↗
- 6Granular cell tumor: report of 13 cases in a Veterans Administration Hospital Mil Med Jobrack AD Goel S Cotlar AM 093183201810.1093/milmed/usx 23729548015 · doi ↗ · pubmed ↗
- 7Endoscopic resection of colorectal granular cell tumors World J Gastroenterol Take I Shi Q Qi ZP Cai SL Yao LQ Zhou PH Zhong YS 13542135472120152673016610.3748/wjg.v 21.i 48.13542 PMC 4690184 · doi ↗ · pubmed ↗