Quality of life and patient reported outcomes in the UK Mammo-50 randomised trial of annual versus less frequent mammographic surveillance in people with breast cancer aged 50 years and over
Andrea Marshall, Peter Donnelly, Nada Elbeltagi, Sophie Gasson, Amy Broadfield, Amy Hopkins, Sue Hartup, Lesley Turner, Annie Young, Eila K Watson, Janet A Dunn

TL;DR
A UK trial found that less frequent mammograms for older breast cancer survivors did not harm their quality of life compared to annual checks.
Contribution
This study provides evidence that less frequent mammographic surveillance does not negatively affect quality of life in older breast cancer survivors.
Findings
No differences in quality of life were found between less frequent and annual mammogram groups.
Participants' concerns were more about side effects and family issues than mammogram frequency.
Long-term follow-up showed consistent quality of life outcomes across trial arms.
Abstract
Mammo-50, a randomised phase III trial, demonstrated that for women aged 50 years or older and 3-years post breast cancer diagnosis, less frequent mammograms (2-yearly after conservation surgery; 3-yearly after a mastectomy) were non-inferior to annual mammograms in terms of detection of recurrences, or new breast primaries. It is important to assess Quality of life (QoL) in this population to ensure no detriment is associated with a less frequent mammographic surveillance schedule. A mixed methods QoL sub-study was undertaken to explore potential differences between the trial arms in terms of fear of recurrence, QoL and distress levels and to explore patient reported experiences. Participants were asked to complete a questionnaire booklet annually whilst on the trial. Longitudinal random effects regression models were fitted to assess changes in QoL over time and across trial arms.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
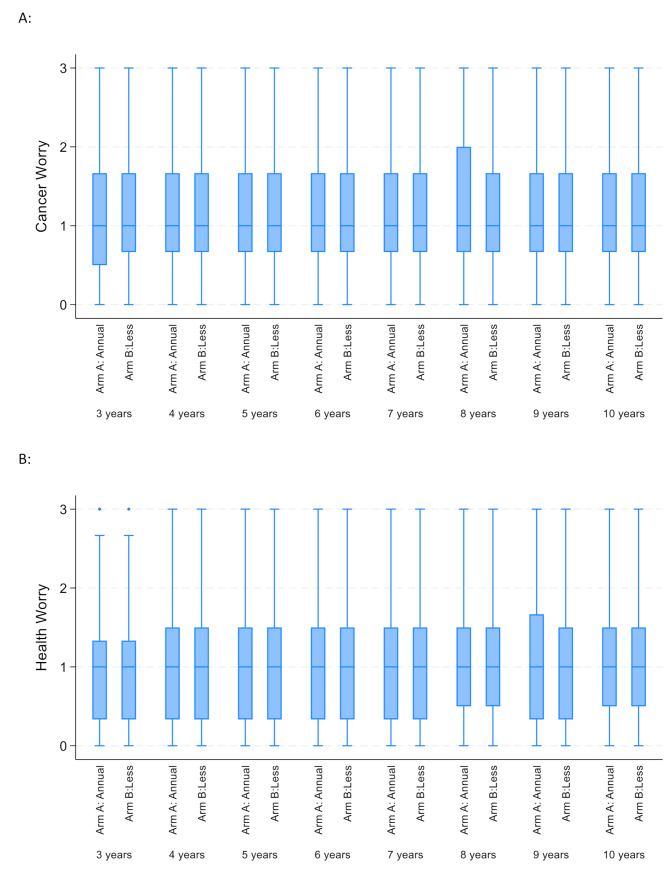 Figure 1
Figure 1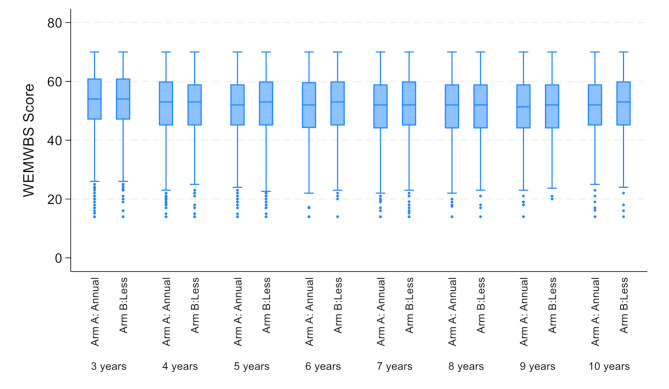 Figure 2
Figure 2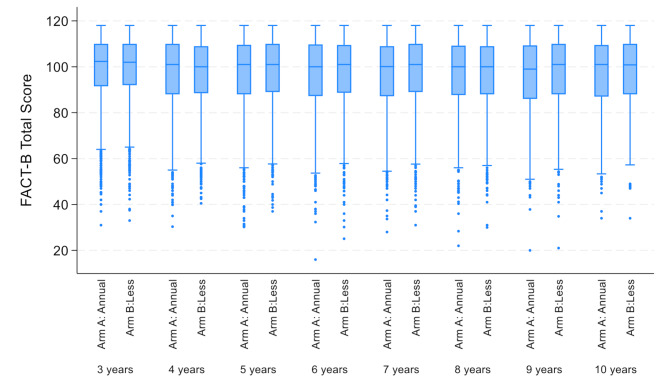 Figure 3
Figure 3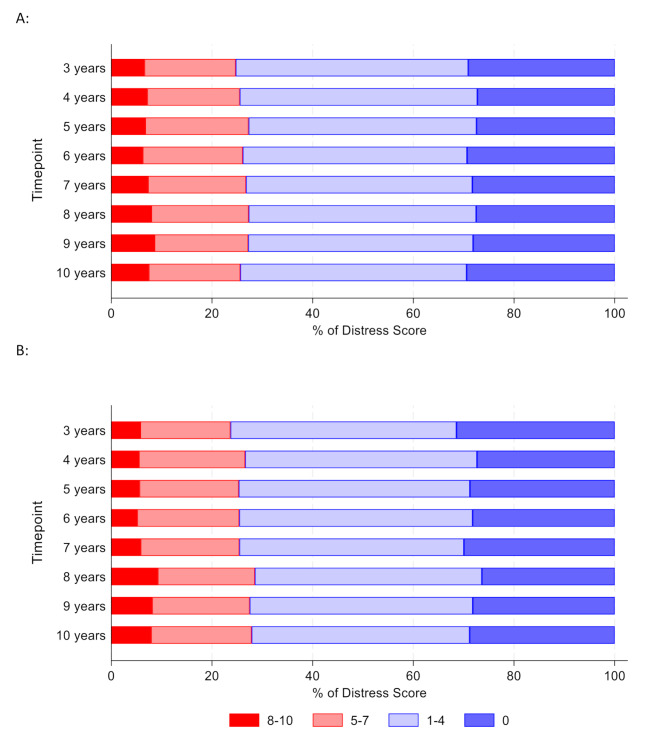 Figure 4
Figure 4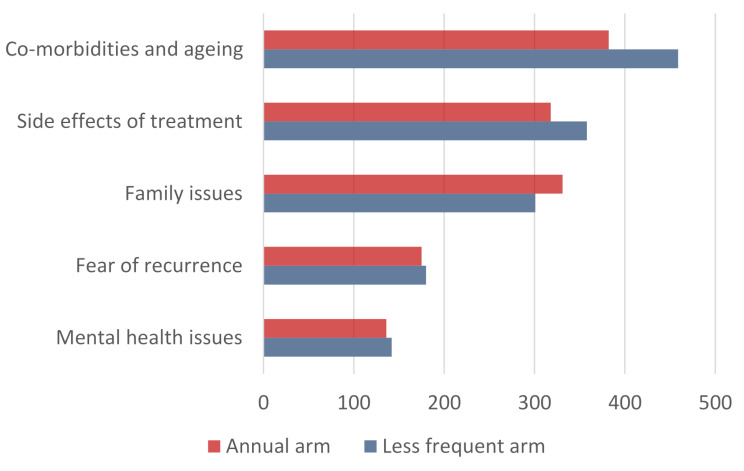 Figure 5
Figure 5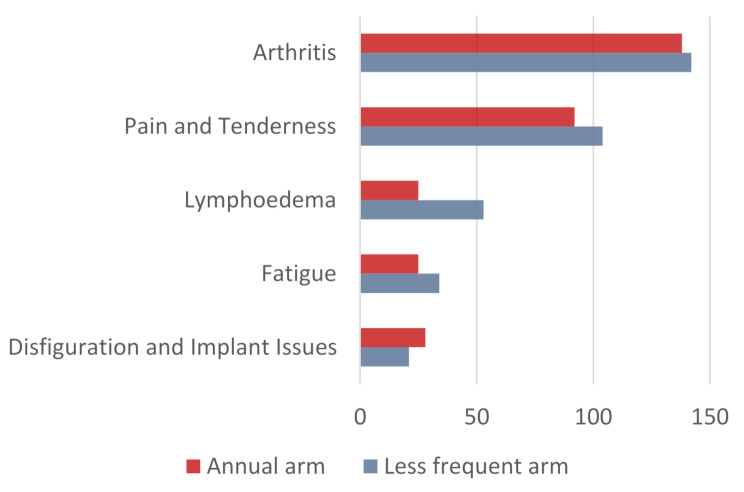 Figure 6
Figure 6- —National Institute for Health Research (NIHR) Health Technology Assessment (NIHR HTA) Programme
- —National Institute for Health Research Senior Investigator Award
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer survivorship and care · Global Cancer Incidence and Screening · Women's cancer prevention and management
Background
Breast cancer remains the most common female cancer worldwide with over 55,900 new cases diagnosed each year in the UK [1] and estimated 2,296,840 new cases diagnosed globally in 2022 [2]. In the UK around 82% of women diagnosed with breast cancer are aged 50 years or older; the 5-year survival rate in the UK is around 88% which has improved progressively in the last 30 years [1]. However as women are surviving longer after their diagnosis, follow-up surveillance and quality of life (QoL) becomes increasingly important for patients and the health care system [3].
It is widely known that treatment for breast cancer can cause many physical and emotional effects thus affecting the QoL of patients, and patient reported outcomes measures (PROMs) help to evaluate these [4, 5]. One of the most common emotional effects of breast cancer is fear of recurrence [6]. Evidence shows that long-term breast cancer survivors still experience fear of recurrence even ten years after diagnosis, which has a negative impact on women’s QoL and an increased depression risk [7, 8]. For some women, these concerns have been allayed to some extent by an annual mammogram and routine clinical examination [9, 10].
Mammo-50, a randomised phase III trial, demonstrated that for women aged 50 years or older and 3-years post breast cancer diagnosis, less frequent mammograms (2-yearly after conservation surgery; 3-yearly after a mastectomy) were non-inferior to annual surveillance mammography in terms of clinical outcomes including breast cancer specific survival and recurrence-free interval [11]. These findings indicate that it was safe to de-escalate surveillance mammography for this population of women who were at a lower risk of breast cancer recurrence [11]. However, before reducing mammographic surveillance, it is important to ensure that there is no detriment to QoL associated with a reduced mammographic surveillance schedule.
A mixed methods QoL sub-study was conducted within the Mammo-50 trial to assess whether differences between the two trial arms occurred in terms of fear of recurrence, QoL and distress levels. A secondary aim was to explore additional patient reported worries and concerns.
Methods
Mammo-50 was a pragmatic multicentre, randomised phase III trial of annual versus less frequent mammography (2-yearly after conservation surgery; 3-yearly after a mastectomy) for women aged 50 years or over at initial diagnosis of invasive or non-invasive breast cancer, and who were recurrence free 3-years post curative surgery (ISRCTN48534559, 26 February 2014) [11]. Full details of the eligibility criteria for the Mammo-50 trial are given elsewhere but all participants gave written informed consent [11]. Patients with bilateral breast cancer including DCIS, known BRCA or genetic mutation, or a previous breast malignancy were excluded from the study. For women with significant mental health problems, or where English was not their first language, it was left to the discretion of the recruiting clinician. Participation in the mixed methods QoL sub-study was optional. Women who consented were asked to complete a QoL booklet at trial entry (baseline) and then annually for seven years (up to ten years post curative surgery). Participants were encouraged where possible to continue to complete the questionnaires after a recurrence, but could withdraw from the QoL sub-study if they felt unable to continue. Demographics, treatment history and clinical outcomes were collected as part of the main trial [11].
QoL booklet
The QoL booklet was designed in collaboration with patient representatives and the Independent Cancer Patients’ Voice (ICPV) patient and public involvement (PPI) group. It included the Assessment of Survivor Concerns (ASC) scale [12], Warwick Edinburgh Mental Well-being Scale (WEMWBS) [13], the Functional Assessment of Cancer Therapy for breast cancer (FACT-B) [14] and the USA National Comprehensive Cancer Network (NCCN) Distress Thermometer and problem list [15] and also a blank page for free text data.
The ASC scale contains six questions measuring fears about recurrence and health in cancer survivors with responses on a 4 point Likert scale (‘‘not at all’’, ‘‘a little bit’’, ‘‘somewhat’’, or ‘‘very much’’) [12]. The questions are combined into a cancer worry and a health worry subscale.
The WEMWBS is a validated 14 item scale describing patients’ feelings and thoughts with responses on a 5 point scale (1 = None of the time, 2 = Rarely, 3 = Some of the time, 4 = Often, 5 = All the time). A total score is calculated by summing the 14 individual statements. The average population mean score is around 51 but varies according to the population studied [13].
The FACT-B + 4 is a 41 item questionnaire assessing five domains: physical well-being, social/family well-being, emotional well-being, functional well-being and additional concerns. The responses are on a 5-point Likert scale between 0 (Not at all) to 4 (Very much). Domain scores were calculated using the user guide document for this questionnaire with higher scores representing better quality of life [14].
The NCCN Distress Thermometer measures how distressed a patient has been feeling for the past week by circling a number between 0 and 10, 0 meaning no distress and 10 meaning high distress [15]. Scores were categorised into no distress (score = 0), low distress (scores of 1–4), moderate levels of distress (scores of 5–7) and high levels of distress (scores of 8–10). It also includes a problem list where participants identify from the list of physical, practical, family, emotional or spiritual/religious problems any concerns they may be facing and rank the top four in order of ascending difficulty. On advice from the oversight committees, the reasons for any participant reporting high levels of distress (scores of 8-10) were reported back to the clinical team at sites.
In addition, a blank page was included at the end of the QoL booklet where the participants were asked to report any further details about their worries or concerns.
Sample size
The Mammo-50 trial required 5000 women to be recruited to demonstrate a 3% non-inferiority margin assuming 5 year disease specific survival of 89% with a 2.5% one-sided significance and 90% power. For the QoL sub-study, a minimum sample of 600 participants was needed to allow the detection of a relatively small standardised difference of 0.3 in QoL with 90% power and 5% 2-sided significance level. For example, this would equate to a 7.5% change in QoL assuming a conservative standard deviation of 25%. It was agreed with the trial oversight committees and the PPI group to offer all women entering the Mammo-50 trial the opportunity to participate in the QoL sub-study.
Analysis
Descriptive statistics using median and interquartile ranges for continuous variables and frequencies and percentages for binary and categorical variables were used to summarise the characteristics of the participants. The scores for each QoL measure were summarised for each timepoint using means and standard deviations or medians and interquartile ranges as appropriate. Distress Thermometer scores at baseline were categorised and compared across participant characteristics using a chi-squared test to identify factors that influenced the level of distress. To account for the repeated collection of QoL data from the same participants, longitudinal random effects regression models were used to assess whether QoL changed over time and differed across trial arms using all available data. Characteristics, including age, oestrogen receptor (ER) status, surgery type, disease type, hormone therapy use at randomisation, chemotherapy use and human epidermal growth factor receptor (HER2) status were also considered in a multivariate regression model to assess for independent predictors of high levels of distress.
A thematic content analysis [16] of the completed free text fields for all participants was carried out by SG using NVIVO version 12 software. Keywords that encapsulated the participant’s worries and concerns were identified from the free text and resulting themes developed. The themes were validated by a second independent researcher AB. Researcher were blinded to the trial arms whilst coding and only linked back to the trial arm data once content analysis was completed.
Results
A total of 5235 women were randomised into the Mammo-50 trial between April 2014 and September 2018. 3858 (74%) participants were aged 60 years or older, 5084 (97%) were from a white ethnic background, 3279 (63%) had asymptomatic screen-detected tumour, 4202 (80%) had undergone conservation surgery, 4576 (87%) had invasive disease and 4330 (83%) had ER-positive tumours [11]. Of the 5235 women that were randomised, the majority (4751; 91%) consented to be in the QoL sub-study; 4488 (86%) women returned a baseline QoL booklet and a total of 4668 (89%) women returned at least one QoL booklet (Table 1). Given the majority of trial participants took part in the QoL sub-study, these were a representative sub-population of the main Mammo-50 trial [11].
Table 1. Form returnTimepointAnnual MammographyN (%)Less frequent mammographyN (%)Total randomisedN (%)Total randomised261826175235 Baseline (3 years post curative surgery) 2260 (86.3)2228 (85.1)4488 (85.7) 4 years 2062 (78.8)1886 (72.1)3948 (75.4) 5 years 1924 (73.5)1757 (67.1)3681 (70.3) 6 years 1742 (66.5)1594 (60.9)3336 (63.7) 7 years 1670 (63.8)1513 (57.8)3183 (60.8) 8 years 1506 (57.5)1418 (54.2)2924 (55.8) 9 years 1103 (42.1)993 (37.9)2096 (40.0) 10 years 696 (26.6)609 (23.3)1305 (24.9) Number of patients with at least one form
2351 (89.8)
2317 (88.5)
4668 (89.2) *Note data collection for year 10 ongoing
For all participants in the QoL sub-study, the median ASC cancer worry subscale score at baseline was 1 (Interquartile range 0.7–1.7) representing a “little bit” of concern (Table 2); no differences were seen between the trial arms (p = 0.60, Fig. 1A). Similarly, the median health worry subscale score at baseline was 1 (Interquartile range 0.3–1.3) representing a “little bit” of concern; no differences were seen between trial arms (p = 0.58, Fig. 1B). There was a small, yet statistically significant increase in cancer worry over time (β = 0.012; 95% CI 0.008–0.015, p < 0.001, Fig. 1A) and in health worry scores over time (β = 0.019; 95% CI 0.015–0.023, p < 0.0001, Fig. 1B).
Table 2. Summaries of quality-of-life scales at baselineCharacteristicAnnual MammographyLess frequent mammographyTotal randomised Total number with baseline form (%) 2260 (86.3)2228 (85.1)4488 (85.7) Assessment of Survivor Concerns Fear of Recurrence
Cancer worry subscale Median (IQR)1 (0.5–1.7)1 (0.7–1.7)1 (0.7–1.7) Missing (n(%))115 (5.1)132 (5.9)247 (5.5) Health worry subscale Median (IQR)1 (0.3–1.3)1 (0.3–1.3)1 (0.3–1.3) Missing (n(%))191 (8.5)189 (8.5)380 (8.5) The Warwick-Edinburgh Mental Well-being Scale (WEMWBS)
WEMWBS score Median (IQR)54 (47–61)54 (47–61)54 (47–61) Missing (n(%))32 (1.4)41 (1.8)73 (1.6) Functional Assessment of Cancer Therapy - Breast
Physical well-being subscale score Median (IQR)25 (22–27)25 (22–27)25 (22–27) Social/family well-being subscale score Median (IQR)25 (20–28)25 (20–27)25 (20–27) Emotional well-being subscale score Median (IQR)21 (18–23)21 (18–23)21 (18–23) Functional well-being subscale score Median (IQR)24 (19–26)24 (20–26)24 (20–26) Additional breast cancer concerns subscale score Median (IQR)30 (25–34)30 (25–34)30 (25–34) FACT-B Trial Outcome Index (TOI) Median (IQR)78 (68–85)78 (68–85)78 (68–85) FACT-G total score Median (IQR)93 (82–100)92 (82–100)92 (82–100) FACT-B total score Median (IQR)122 (108–133)122 (108–132)122 (108–132)Missing (n(%))72 (3.2)71 (3.2)143 (3.2)
Fig. 1. Assessment of survivor concerns (ASC) over time and by trial arm (Arm A: Annual mammography arm; arm B: less frequent mammography). A: Cancer Worry Scores; B Health Worry Scores
The median WEMWBS score at baseline was 54 (interquartile range 47–61) for both trial arms (Table 2). Patients’ mental well-being slightly worsened over time (β=-0.396; 95% CI: -0.442 to -0.351, p < 0.001), but did not differ across trial arms (β = 0.147; 95% CI: -0.377-0.670, p = 0.58, Fig. 2).
Fig. 2. Warwick Edinburgh Mental Well-being Scale (WEMWBS) scores over time and by trial arm (Arm A: Annual mammography arm; arm B: less frequent mammography)
The median FACT-B total score at baseline was 122 (interquartile range 108–132); all subscales were similar across trial arms (Table 2). Participants’ QoL as measured by the FACT-B total score significantly decreased over time (β=-0.582; 95% CI: -0.644 to -0.520, p < 0.001). However, no statistically significant differences were found between trial arms (β = 0.294; 95% CI: -0.512-1.102, p = 0.47, Fig. 3).
Fig. 3. Functional Assessment of Cancer Therapy (FACT-B) Total Scores over time and by trial arm (Arm A: Annual mammography arm; arm B: less frequent mammography)
Of the 4488 women returning a baseline QoL form, 3872 (86%) women completed the NCCN distress thermometer. A total of 1171 (30%) women had no levels of distress, 1764 (46%) had low levels of distress (score 1–4), 698 (18%) moderate levels of distress (score 5–7) and 239 women (6%) reported high levels of distress (score 8–10) at baseline (Table 3). There was a small, yet statistically significant, increase in distress scores over time (β_time_ = 0.05; 95% CI: 0.04–0.07, p < 0.001); however, the levels of distress did not significantly differ between the trial arms (β_arm_=-0.04; 95% CI: -0.16-0.08, p = 0.48, Fig. 4).
Table 3. Distress thermometer scores over timeDistress scoreBaselineN (%)4 yearsN (%)5 yearsN (%)6 yearsN (%)7 yearsN (%)8 yearsN (%)9 yearsN (%)10 yearsN (%) N randomised 44883948368133363183292420961305 N completed
3872
3354
3146
2851
2728
2532
1829
1136
0 1171 (30.2)916 (27.3)883 (28.0)821 (28.8)793 (29.1)683 (27.0)515 (28.2)331 (29.1) 1–4 1764 (45.6)1565 (46.7)1434 (45.6)1295 (45.4)1222 (44.8)1143 (45.1)814 (44.5)502 (44.2) 5–7 698 (18.0)660 (19.7)634 (20.2)572 (20.1)533 (19.5)489 (19.3)347 (19.0)216 (19.0) 8–10 239 (6.2)213 (6.3)195 (6.2)163 (5.7)180 (6.6)217 (8.6)153 (8.4)87 (7.7) Missing 616594535485455392267169
Fig. 4. Percentage of distress scores over time split by trial arm; 1 A: for the Annual mammography arm; 1B: For the Less frequent mammography arm A:
The use of hormone therapy at randomisation was the only characteristic that significantly affected participants categorised levels of distress at baseline (p = 0.007, Table 4). Those participants that had stopped hormone therapy prior to enrolment onto the Mammo-50 study reported higher levels of distress (34% with moderate to high levels of distress) compared to those that were continuing to take hormone therapy (24%) and those that never took hormone therapy (24%; Table 4). The results of the multivariate modelling for predicting high levels of distress identified disease type (β = 0.400; 95% CI: 0.106–0.694, p = 0.008) and hormone therapy at randomisation (β = 0.124; 95% CI: 0.014–0.235, p = 0.027) as the only significant factors. Higher levels of distress were associated with invasive disease and never taking hormone therapy.
Table 4. Disease and treatment characteristics for the randomised patients by distress thermometer scores at baselineCharacteristicsNo distress (0)N (%)Low (1–4)N (%)Medium (5–7)N (%)High (8–10)N (%)Chi-square P-value Total for randomised 1171 (30.2)1764 (45.6)698 (18.0)239 (6.2) ER status 0.281ER negative146 (34.5)183 (43.3)75 (17.7)19 (4.5)ER positive943 (29.4)1475 (46.0)580 (18.1)206 (6.4)Not done82 (33.5)106 (43.3)43 (17.6)14 (5.7) Surgery type 0.256WLE927 (29.7)1447 (46.3)558 (17.9)192 (6.2)Mastectomy244 (32.6)317 (42.4)140 (18.7)47 (6.3) Disease type 0.597DCIS158 (32.7)209 (43.3)89 (18.2)28 (5.8)Invasive1013 (29.9)1555 (45.9)610 (18.0)211 (6.2) Hormone therapy 0.007On-going847 (30.1)1304 (46.3)487 (17.3)178 (6.3)Stopped44 (21.9)89 (44.3)52 (25.9)16 (8.0)Never280 (32.8)371 (43.4)159 (18.6)45 (5.3) HER2 status 0.414Positive125 (31.8)177 (45.0)71 (18.1)20 (5.1)Negative879 (29.4)1382 (46.3)537 (18.0)189 (6.3)Not done167 (33.9)205 (41.7)90 (18.3)30 (6.1) Chemotherapy (CT) 0.950Yes330 (30.1)506 (46.2)193 (17.6)67 (6.1)No838 (30.3)1256 (45.3)504 (18.2)172 (6.2)Missing3 (50.0)2 (33.3)1 (16.7)0 CT containing taxane 0.972Without taxane144 (29.9)225 (46.7)82 (17.0)31 (6.4)With taxane184 (30.1)280 (45.8)111 (18.2)36 (5.9)Not specified2 (66.7)1 (33.3)00
The most common reasons from the problem list reported for causing high levels of distress (score of 8–10) at baseline, for the 239 participants, were fatigue, exhaustion or extreme tiredness (135 (56%) participants), sleep problems and/or nightmares (134 (56%) participants), worry, fear or anxiety (113 (47%) participants), hot flushes (96 (40%) participants), pain (84 (35%) participants), memory loss or concentration (83 (39%) participants), and sadness or depression (83 (35%) participants); these concerns remained constant over time (Table 5).
Table 5. The most common reasons for causing high levels of distress in all patients over timeMost common reasons for high level distress (8–10)BaselineN(%)4 yearsN(%)5 yearsN(%)6 yearsN(%)7 yearsN(%)8 yearsN(%)9 yearsN(%)10 yearsN(%) N 23921319516318021715387 Fatigue & exhaustion 135 (56.5)128 (60.1)103 (52.8)95 (58.3)91 (50.6)112 (51.6)80 (52.3)45 (51.7) Sleep problems and/or nightmares 134 (56.1)117 (54.9)89 (45.6)72 (44.2)75 (41.7)106 (48.8)69 (45.1)42 (48.3)Worry,** fear or anxiety**113 (47.3)122 (57.3)107 (54.9)95 (58.3)101 (56.1)124 (57.1)80 (52.3)47 (54.0) Hot flushes 96 (40.2)85 (39.9)63 (32.3)42 (25.8)43 (23.9)49 (22.6)31 (20.3)12 (13.8) Pain 84 (35.1)70 (32.9)58 (29.7)70 (42.9)61 (33.9)71 (32.7)47 (30.7)25 (28.7) Memory or concentration 83 (34.7)80 (37.6)72 (36.9)63 (38.7)72 (40.0)81 (37.3)55 (35.9)23 (26.4) Sadness or depression 83 (34.7)87 (40.8)92 (47.2)70 (42.9)76 (42.2)91 (41.9)68 (44.4)32 (36.8)
Thematic content analysis
A total of 5125 free text fields were completed from 2581 participants (1304 participants on the annual arm; 1277 participants on the less frequent arm), with some participants contributing at several time points. The thematic content analysis of the free text responses from the questionnaire identified the main themes for participants on both arms of the study as co-morbidities and ageing, side effects of treatment, family issues, fear of recurrence and mental health issues (Fig. 5).
Fig. 5. Frequency of overarching themes identified within the free text fields for the patient reported experiences
Many of the respondents described how they were living with co-morbidities which caused them more problems than their sometimes long-forgotten breast cancer diagnosis, e.g. cardiac issues (Table 6). Arthritis and osteoarthritis were cited by many respondents.
Table 6. Selected quotes relating to the patient reported experiences from the free text field on the quality of life bookletsCo-morbidities and ageing (22% of text fields)• As I am 72 it may be difficult to separate symptoms,* like fatigue and lack of strength (physical & mental), from possible post cancer symptoms. [Annual Arm 3 year]• I have lost about a stone in 6 months. My IBS is causing me some distress, but not the breast cancer. [ Annual Arm 4 year]• My main problem now is I have an inoperable leaking heart valve….this stops me doing a lot of the things I did. [Annual Arm 10 year]• I am a 70 year old lady living on her own. Any difficulties I have are more related to my age rather than having had breast cancer [Less frequent arm year 5].• I enjoy life rarely think about my former illness I get a bit of pain and stiffness but mostly related to age as I am 76 and lack a bit of energy for the same reason. [Less frequent arm year 8]. Side effects of treatment (18% of text fields) • In the area of my operation after 3 years I still experience ‘pulling’ around the breast and pain in my ribs, this bothers me sometimes. [ Annual Arm 3 year]• Would accept it [hormone therapy] again as a precaution but feel that the treatment has been worse than the problem. [ Annual Arm 5 year]• Apart from the pain in the reconstruction area, I rarely think about breast cancer now. I wish I hadn’t had the reconstruction*,* as it feels false & is still uncomfortable*,* but it does not affect my life. [Less frequent arm year 5].• I stopped taking Letrozole after 3.5 years. it made sleeping difficult - (hot flushes), I also got trigger fingers which made gardening*,* especially pruning*,* painful and awkward [Less frequent arm year 4].* Family Issues (16% of text fields) • My husband died……during the night after many years of continuing weakness following strokes,* we were married 62 years. I think maybe my answers to the questionnaire may be coloured by my response to this*,* rather than actual cancer worries [ Annual Arm 10 year]• …many of my feelings about emotional wellbeing relate to loss and bereavement… At the time this completely erased all my feelings about my own illness. I am still learning to cope with loss. [ Annual Arm 4 year]• My husband… passed away. This has obviously affected my well being. [Less frequent arm year 10].• My only problems are all related to having a daughter who had to move in with me. Her problems just keep on growing - and it is all draining me - physically, mentally and financially!!!* [Less frequent arm year 3] Fear of recurrence (9% of text fields) • With hindsight I would have preferred not to be in the trial as each year I have had a mammogram and had an all-clear letter I felt confident I was doing okay. This year of course I did not have that satisfaction. [Less frequent Arm 4 year]• I often think about a recurrence and reflect back on the treatment I received which saved my life and hope I don’t have to go through it again. [Annual Arm 3 year]• I have never felt that after removal of the cancer,* it was an illness. I prefer to be positive and enjoy life. [Annual Arm 10 year]• I am anxious that I may get cancer again [Less frequent arm year 4] Mental Health Issues (7% of text fields) • The mental wellbeing of cancer patients is not being considered at all both during and after treatment. Life does change, cannot work out what is normal and what is down to side and after effects of cancer [Annual Arm 4 year]• The one thing that has affected me since my diagnosis is my lack of s self-confidence - this has really had a major impact on my life and the way I feel mentally……. as soon as all the treatment was over I felt very down and this has led to depression (whether this is due to the side effects of some of the medication I take I am unsure) but it is a constant battle to motivate myself to do anything or to socialise…. [ Annual Arm 3 year]• Most of my health concerns are not related to cancer. Arthritis and mental health play a large part [Less frequent arm year 4].• My temper seems to be at a higher level these days. It worries me because relationships at home are suffering, and I nearly lost a close friend because of my volatile temper. [Less frequent Arm 8 year]*
676 (18%) of the free text fields cited issues with side-effects of their cancer treatment (318 on the annual arm and 358 on the less frequent arm) (Fig. 5). The side effects most frequently described were arthritis, pain/tenderness, lymphoedema, fatigue and disfiguration/implant issues (Fig. 6; Table 6).
Fig. 6. Frequency of side effects of treatment identified within the free text fields for the patient reported experiences
Family issues were cited in 632 (16%) free text fields (331 annual arm and 358 less frequent arm), (Fig. 5). Many of the reported family issues were inevitable consequence of living into older age, e.g. the death of a partner (Table 6).
355 (9%) free text fields described a fear of recurrence (175 annual arm and 180 less frequent) (Fig. 5). Participants in both arms of the study describe fear of recurrence and this fear is expressed at all timepoints of the study. Other participants stated that they really didn’t think about their breast cancer anymore.
Whilst 278 (7%) of the text fields cited issues with mental health (132 annual arm and 142 less frequent) (Fig. 5), reasons were often not directly related to the cancer diagnosis, but included family issues, bereavements and co-morbidities. Some of the participants report changes in their mood, often describing how difficult this can be to control. Finally, self-confidence is an issue for lots of participants (Table 6).
Discussion
The Mammo-50 QoL sub-study explored QoL, fear of recurrence, distress levels as well as worries and concerns within a large randomised multicentre trial of annual versus less frequent mammographic surveillance. For this population of women aged 50 years or older at diagnosis of breast cancer and recurrence free at 3 years post diagnosis, there was no difference between trial arms for any of the QoL scales used in the study, suggesting that less frequent mammographic surveillance did not adversely impact QoL. The choice of validated QoL scales were informed in collaboration with the patient and public involvement group to reflect the issues such as fear of recurrence, mental health and well-being as well as functional assessment that were of importance to women with breast cancer in follow-up. In addition, the NCCN Distress Thermometer was used for patients to self-evaluate their levels of distress and its underlying causes [17, 18]. Within Mammo-50 the Distress Thermometer was a useful tool to identify participants with persistent unmet needs resulting from their diagnosis or their treatment for early breast cancer. Within our study, there was a small percentage of women who had high levels of distress (scores of 8–10) at baseline (6.2%), which was persistent over time (7.7% at 10 years), and the reasons associated with this distress was reported back to the clinical teams at site. In any de-escalation trial there needs to be some way of managing this small percentage of women longer term.
The differences found across time with increases in the distress scores, survivor concerns and cancer worry could be attributable to the very large numbers assessed in this study (i.e. the ability to detect very small differences) or it could reflect the patients’ worry increasing over time. It was reassuring that the median WEMWBS score of 54 in each trial arm was similar to the median score of 51 in the general population implying that for the majority of women they did not have impaired mental health or wellbeing. Existing research confirms that women with breast cancer experience higher levels distress, side effects and fear of recurrence, throughout their treatment and follow up [19]. Those with high levels of distress experience a poorer quality of life and survival rates [20]. Worry was the most frequently selected reason for the distress in our study. Fatigue and sleep issues were another physical problem experienced by women with breast cancer, causing increased distress [20, 21]. Osteoporosis is one of the most common side effects of cancer treatment which can greatly impact a patients QoL [22], along with long term physical changes such as chronic pain and anatomic changes [23].
This study is unique as it includes one of the largest collections of PROMs data [4, 5] and direct speech, reported in the free text, shared by breast cancer survivors, predominantly after conservation surgery and gathered over seven years, after the peak of clinical events. The voices in this report come mostly from participants benefiting from conservation surgery, with few making reference to the emotional morbidity of disfigurement. Both the Qol and the free text data support that women on both arms of the trial experienced similar levels of distress and worries. Participants irrespective of the frequency of mammographic surveillance indicated within the free text field that they were worried more about family issues and co-morbidities than their breast cancer. Fewer participants said they were worried about fear of recurrence than about other issues, regardless of which arm of the study they were on. Our study has highlighted that mental health is a constant struggle for many of these women as they cope with their personal history of breast cancer whilst supporting their loved ones as they move into older age.
Many of the side effects from the treatment this group of patients receive, especially taxanes and hormone treatment, can manifest in the same way as general effects of ageing and menopause: including fatigue, muscle aches and pains, increased body fat, hot flushes, sleepless nights [24]. Many of the women in the trial received aromatase inhibitors, prescribed to lower the natural levels of oestrogen after the menopause, but these are often responsible for arthritic side effects [24]. However, as this cohort of women could also be going through the menopause and naturally ageing, it is difficult to ascertain whether reported co-morbidities and side effects can be directly attributed to their hormone therapy or due to the ageing process.
To discontinue the hormone treatment means increasing the risk of recurrence and so women often prefer to continue and simply accept the side effects [25, 26]. The worry of stopping hormone therapy early may be reflected in the Mammo-50 participants reporting 10% higher levels of distress for those stopping treatment early compared to those who have never been on hormone therapy or those whose hormone therapy is on-going, albeit this group was quite small. Aging and menopause bring a whole range of inevitable symptoms, but it is unwise to dismiss them as not distressing [27]. Aging has a particular significance to cancer patients, it heralds a physiological decline in host immunity and immunosurveillance of occult disease [28]. A patient in self-care many years post diagnosis might best be prompted to take steps to prolong life by adhering to oestrogen deprivation measures and improving immunity by exercise, diet and avoiding smoking or alcohol [5, 29].
The Mammo-50 QoL sub-study provided a wealth of QoL data and patient reported experiences on the long-term survivorship of a large population of women with breast cancer. However, the trial was limited to those aged 50 years or older at diagnosis and at lower risk due to having to be recurrent free at three years post diagnosis and despite the trial being pragmatic majority of the participants recruited were from a white ethnic background and had small, lower grade ER positive tumours [11]. Thus as the results of this QoL substudy may not be generalisble to younger women diagnosed under 50, those at a higher risk, i.e. triple negative cancer, or those from other ethnic backgrounds that were not well represented within the Mammo-50 trial populations, further research is required.
Conclusions
For women aged 50 years or older and 3-years post breast cancer diagnosis, less frequent mammograms (2-yearly after conservation surgery; 3-yearly after a mastectomy) compared to annual mammograms did not impact on their QoL or their reported experiences. For this group of ageing women, the Distress Thermometer provided a useful triaging tool that identified a small percentage of women with raised levels of distress even ten years after their diagnosis of breast cancer. These women may benefit from additional intervention whether this be psychosocial or management of ongoing hormone therapy side-effects or management of new co-morbidities. The results of this study add to the available evidence and help to inform clinical practice regarding the use of less frequent mammographic surveillance for this population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1: Facts and Figures, Cancer B, May UK. 2024 [Available from: https://www.breastcanceruk.org.uk/about-breast-cancer/facts-figures-and-qas/facts-and-figures/
- 2Marzban S, Shokravi S, Abaei S, Fattahi P, Karami M, Tajari F. Patient-Reported outcome measures of breast Cancer surgery: evidence review and tool adaptation. Cureus 14(8):e 27800.10.7759/cureus.27800 PMC 948122536134055 · doi ↗ · pubmed ↗
- 3Maheu C, Singh M, Tock WL, Eyrenci A, Galica J, Hébert M et al. Fear of Cancer recurrence, health anxiety, worry, and uncertainty: A scoping review about their conceptualization and measurement within breast Cancer survivorship research. Front Psychol. 2021;12.10.3389/fpsyg.2021.644932 PMC 807211533912113 · doi ↗ · pubmed ↗
- 4NCCN. Distress Management (Version 1.2008) 2007 [Available from: http://www.nccn.org
- 5Nardin S, Mora E, Varughese FM, D’Avanzo F, Vachanaram AR, Rossi V et al. Breast Cancer survivorship, quality of life, and late toxicities. Front Oncol. 2020;10.10.3389/fonc.2020.00864 PMC 730850032612947 · doi ↗ · pubmed ↗