Prevalence and clinical impact of severe anaemia in referral hospitals in southern Benin
Landry Assongba, Oumou Boukari, Jules Maroufou Alao, Natacha Nouwakpo, Jeanne Perpétue Vincent, Adrian J. F. Luty, Feiko O. ter Kuile, Achille Massougbodji, Jenny Hill, Valérie Briand, Manfred Accrombessi

TL;DR
This study examines the prevalence and impact of severe anemia in children in southern Benin, finding it to be a major health issue linked to severe malaria and malnutrition.
Contribution
The study provides updated data on severe anemia in southern Benin, highlighting its clinical impact and the need for integrated prevention strategies.
Findings
Severe malaria and clinical severe anemia were the most common diagnoses among hospitalized children.
Severe malnutrition significantly increased the risk of death in children with severe anemia.
An integrated strategy combining malaria chemoprevention and nutritional interventions is needed to reduce mortality.
Abstract
Severe anaemia is a critical public health issue worldwide, disproportionately affecting children in Africa, where approximately 40% of children aged 6 to 59 months are impacted. It leads to significant hospital and post-hospital complications. However, there is a notable lack of research on its burden and clinical impact, particularly in Benin, where existing data are outdated. This study aims to assess the prevalence and impact of severe anaemia in two areas of perennial transmission in southern Benin. We conducted a retrospective cross-sectional study at two referral hospitals in Benin, Lagune Mother and Child University Hospital Centre (CHU-MEL) and the Departmental Hospital Centre-Zou (CHD-Z). Sociodemographic, clinical and biological information were extracted from medical records of patients admitted to paediatric ward in 2023, using a standardised questionnaire. Clinical severe…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
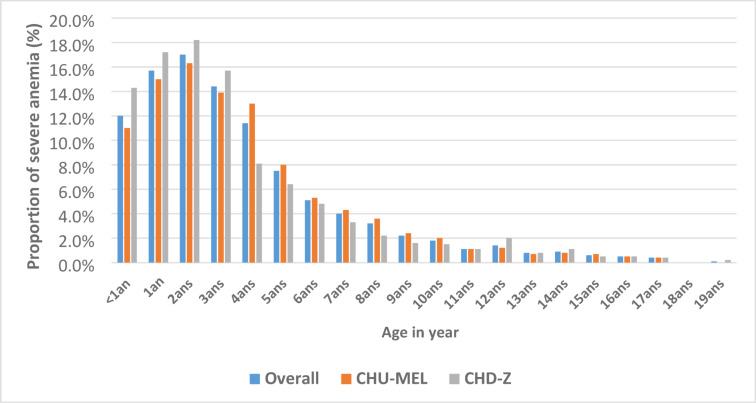 Figure 1
Figure 1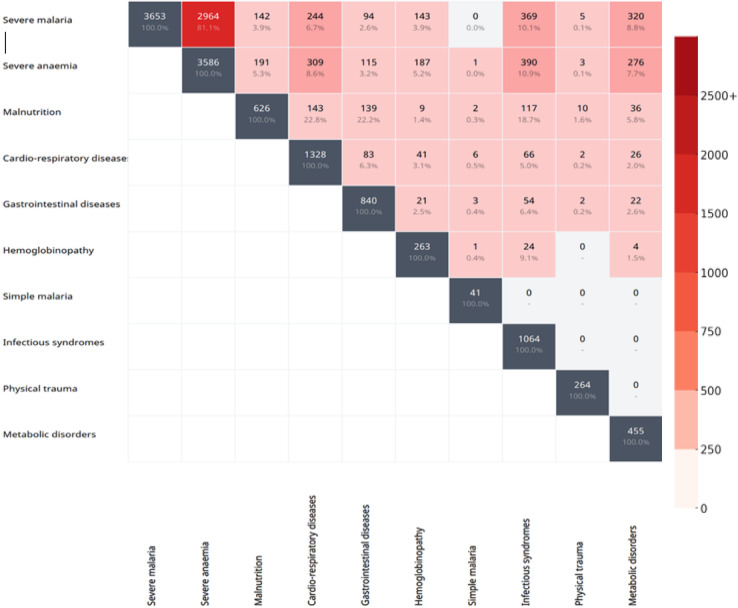 Figure 2
Figure 2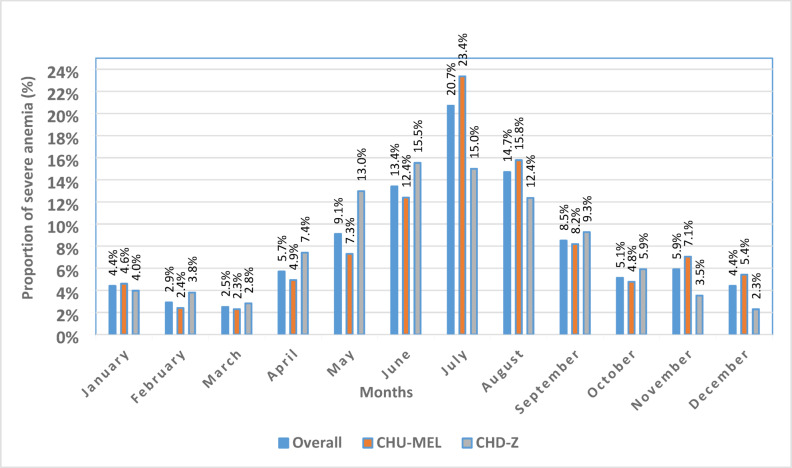 Figure 3
Figure 3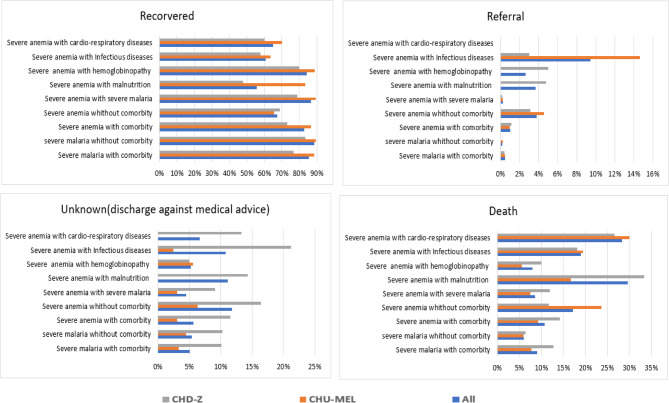 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIron Metabolism and Disorders · Child Nutrition and Water Access · Hemoglobinopathies and Related Disorders
Introduction
Severe anaemia remains a critical global public health concern, disproportionately affecting children in Africa. It is estimated that 40% of children aged 6 to 59 months worldwide suffer from anaemia, and this age group accounts for a substantial proportion of anaemia-related mortality. Africa and South-East Asia are the most affected regions, together contributing to approximately 40% of anaemia cases among children under five^1,2^. It is particularly prevalent in low- and middle-income countries, where children under five experience disproportionately high mortality rates^3^. In sub-Saharan Africa, severe anaemia is a leading cause of hospitalisation and death, largely driven by factors such as nutritional iron deficiency, soil-transmitted helminths, and malaria^2,4^. It is a multifactorial condition, often associated in African countries to specific diseases such as malaria, hookworm and HIV, or with individual factors like nutritional deficiencies in vitamin A or vitamin B12^5^. Despite its widespread prevalence and severe consequences, anaemia remains under-researched. Existing studies suggest that anaemia is associated with significant “hidden” morbidity and mortality, often manifesting months after diagnosis and treatment^3^.
In malaria-endemic regions, anaemia and malaria often coexist, with the prevalence of malaria infection strongly correlated with anaemia rates^6^. Among children under 15 years of age, anaemia prevalence generally increases with parasite density. However, this relationship can be bidirectional: a high parasite density can lead to anaemia, and conversely, anaemia can predispose to more serious parasite infections by impairing immune function^6^. Data on severe anaemia remain limited, and existing data generally come from disease-focused studies or sub-populations such as hospitalised patients^7–9^. In Benin, severe anaemia related to malaria is particularly prevalent in paediatric hospitals^10^. For instance, in northern Benin, 52.6% of severe malaria admissions had severe anaemia, hypoglycaemia, or both^11^. According to the last Demographic and Health Survey conducted in Benin in 2018, the prevalence of severe anaemia in children under five years of age was estimated at 3.3%^12^. Despite its importance, few studies have comprehensively assessed the broader scope of severe anaemia in Benin, including its underlying causes and its impact on both hospital outcomes and post-discharge recovery. While previous studies in Beninin 2015 and 2018 have examined severe anaemia specifically in malnourished children^13,14^, or in the context of transfusion practices in 2024^15^, our study provides a broader perspective by investigating severe anaemia in referral hospitals, and assessing its prevalence and clinical impact.
There is a critical need to assess the burden of severe anaemia in Benin, and its clinical impact on hospital outcomes. The present study aims to quantify the burden of severe anaemia, its associated co-morbidities, and its clinical impact on in-hospital mortality in two geographically distinct referral hospitals in southern Benin.
Methods
Study context
This study was part of the pre-intervention phase to collect baseline data for a cluster-randomised implementation trial designed to assess different strategies for optimising health system delivery of and adherence to post discharge malaria chemotherapy (PDMC) in Benin, an integral part of the EDCTP-funded “PDMC Saves Lives” project (ClinicalTrial.gov, NCT06601712: September 2024; PACTR202411682724094). PDMC is recommended by the World Health Organisation (WHO) for the post-discharge management of children with severe anaemia in settings with moderate to high perennial malaria transmission to reduce hospital readmissions and deaths after discharge.^16^.
Study design
We conducted a retrospective cross-sectional survey in two referral hospitals in Benin: one located in the Littoral region (Lagune Mother and Child University Hospital Centre, CHU-MEL) and the other in the Zou region (Departmental Hospital Centre-Zou (CHD-Z)). The CHU-MEL hospital is a national referral centre focused on mother and child health, situated in Cotonou, the economic capital of Benin. The CHD-Z is the regional referral hospital serving the Zou and Collines areas and is located in Abomey, approximately 150 km from Cotonou. These hospitals were selected as part of the PDMC-SL trial not only because of their status as referral hospitals with adequate technical facilities for severe anaemia management, but also because of their capacity to attract a high annual volume of children from various localities within their catchment areas.
Data collection occurred from March 25, 2024, to May 13, 2024 and encompassed all paediatric admissions to the general paediatric wards of both hospitals during the year 2023. General paediatrics serve children aged 1 month to 18 years. Data were extracted from the medical records of these children using a standardised data collection questionnaire. Neonatal admissions were excluded from the analysis.
Study procedures
Information collected included the child’s age, sex, suspected diagnosis at admission, and confirmed clinical diagnoses as documented by the health care providers. For children diagnosed with severe malaria and/or severe anaemia at admission or during hospitalisation, additional data were gathered. These included anthropometric measurements, vaccination status, HIV status, admission and discharge dates, mode of admission, and any history of severe anaemia within the past year. Details of treatments were also recorded, covering details on parenteral therapies administered during hospitalisation, oral antimalarial treatment prescribed at discharge, and clinical outcomes of disease.
Furthermore, we documented the geographical residence (department, commune, arrondissement, and village) of children admitted for severe anaemia. Finally, when available, we recorded the results of relevant biological tests, including Hb levels, thick blood smear, urine culture, C-reactive protein, blood culture results.
Definition of variables
- (i)Clinical severe anaemia: this refers to a clinical diagnosis of severe anaemia as documented in the medical records. Although the definition may vary slightly based on clinical judgment, it generally includes the presence of palmar pallor, coupled with signs of decompensation (cold extremities, altered consciousness, lower limb oedema, respiratory distress, chest indrawing, intercostal retractions, nasal flaring, increased jugular venous pressure, cardiac failure, or shock).
- (ii)Severe biological anaemia: defined as a haemoglobin level < 5 g/dl^17,18^.
- (iii)severe malarial anaemia: was defined as severe anaemia in the presence of any evidence of malaria infection detected by rapid diagnostic tests or microscopy^19^.
- (iv)Nutritional status: was assessed using weight-for-height (WHZ), height-for-age (HAZ), and weight-for-age (WAZ) z-scores. Severe malnutrition was defined as at least one z-score < − 3, moderate malnutrition as at least one z-score between − 3 and − 2, and no malnutrition as z-scores ≥ − 2^20^.
- (v)Comorbidity: defined as the presence of two or more concurrent diseases or medical conditions in the same patient. In addition to severe anaemia, medical records frequently documented other conditions, including severe malaria, malnutrition, hemoglobinopathies, gastrointestinal diseases, cardio-respiratory diseases and infectious syndromes.
- (vi)In-hospital mortality: defined as any death occurring during hospitalisation among children admitted to one of the two study hospitals in 2023.
- (vii)Clinical outcomes: defined as the final outcome of a patient’s hospitalisation, reflecting the patient’s state of health at the end of their hospital stay. In this study, clinical outcomes are categorised as follows: death during hospitalisation, clinically cured and discharged, discharged against medical advice or referred to another institution for follow-up or specialist care.
Data management and statistical analysis
Data were collected using a standardised questionnaire and entered using KoboCollect v2024.1.3 (developed by the Harvard Humanitarian Initiative), an application installed on tablets and smartphones. Data were transmitted daily to a secure, encrypted server. All data extractions were performed in CSV format, and subsequent analyses were conducted using Stata 15.0 (STATA Corporation, College Station, Texas). No information that would enable patients to be identified directly was collected, and a numeric code was assigned to ensure anonymity and confidentiality throughout the data collection and analysis process.
Data analysis was stratified by study site. The overall prevalence of clinical severe anaemia was calculated as the total number of severe anaemia cases divided by the total inpatient population, with 95% confidence intervals (CI) provided. It was used as a severe anemia variable for the study’s various descriptive and comparative analyses, since it also includes biological severe anaemia. Monthly prevalence rates were also computed to assess potential temporal variations. Descriptive analyses were performed to summarise patient characteristics, including age, gender, origin, HIV status, nutritional status and other comorbidities. Data were presented using means or medians for continuous variables and proportions for categorical variables. The Pearson Chi^2^ or Fisher exact tests were used for comparisons between groups for categorical variables. The Mann–Whitney test was used for comparison of age distributions by in-hospital death status. A bivariate analysis was performed to explore the association between in-hospital mortality related to severe anaemia and potential risk factors (age, sex, child nutritional status, child immunisation status, hospital visited and severe malarial anaemia). A backward stepwise procedure was used to select variables associated with deaths among children admitted to hospital with severe anaemia. A multivariate logistic regression model included variables associated with in-hospital mortality at a significance level of 0.2 in the bivariate analysis.
Ethical considerations
The study protocol was approved by the Ethics and Research Committee of the Institute of Applied Biomedical Sciences (CER-ISBA, N°191 of 18/12/2023). The study was conducted in compliance with the ethical principles from the revised Declaration of Helsinki, guaranteeing the protection of the rights, dignity and confidentiality of the participants.
In accordance with Article 23 of Law No. 2010-40 of 08 December 2010 on the Code of Ethics and Professional Conduct for Health Research in the Republic of Benin, informed consent was not required for this retrospective study based on hospital medical records. No information that could identify the participants was collected, and no contact with the participants was made during data collection. In addition, the study was conducted in referral hospitals with university affiliation, and site-specific research authorisations were obtained.
Results
The final sample consisted of 7152 records, with 4388 from CHU-MEL and 2764 from CHD-Z. The median age (IQR); Range was 32 months (13–61); 1–228 with a slight predominance of males (3853/7152 [53.9%]) (Table 1). Severe malaria and clinical severe anaemia were the leading causes of hospitalisation, accounting for (3653/7152 [51.1%]) and (3586/7152 [50.1%]) of admissions respectively. Less common diagnoses at admission included malnutrition, cardio-respiratory conditions, gastrointestinal diseases, and sickle cell anaemia (appendix).Table 1. Socio-demographic and clinical characteristics of the study population.CharacteristicsAllCHU-MELCHD-ZMedian age in months (IQR; Range)32 (13–61; 1–228)36 (14–60; 1–207)30 (12–72; 1–228)Mean age in months (standard deviation)47.1 (± 45.46)46.2 (± 43.18)48.5 (± 48.84)Proportion of male children (%; n/N)53.9; 3853/715253.1; 2330/438855.1; 1523/2764Proportion of children with severe malaria (%; n/N)51.1; 3653/715262.0; 2720/438833.8; 933/2764Severe malaria parenteral treatment (%; n/N)Artesunate injectable92.3; 3370/365397.6; 654/272076.7; 716/933Artemether injectable0.03; 1/365300.1; 1/933Children tested for malaria (%; n/N)47.7; 3409/715257.9; 2539/438831.5; 870/2764Malaria test result (%; n/N)Negative19.6; 668/340918.2; 463/253923.3; 205/870Positive80.4; 2741/340981.8; 2076/253976.4; 665/870Proportion of children with severe clinical anaemia (%; n/N)50.1; 3586/715256.0; 2453/438841.0; 1133/2464Children tested for Hb among clinical severe anaemia (%; n/N)92.1; 3302/358693.2; 2285/245389.8; 1017/1133Hb level (g/dL) (%; n/N) ≥ 110.7; 22/33020.5; 11/22851.1; 11/10175–10.950.0; 1652/330249.0; 1120/228552.3; 532/1017 < 549.3; 1628/330250.5; 1154/228546.6; 474/1017Severe malarial anaemia (%; n/N)79.0; 2834/358688.7; 2175/245358.2; 659/1133Proportion of children died while in hospital (%; n/N)10.5; 376/35869.1; 223/245313.5; 153/1133Children discharged among severe clinical anemias (%; n/N)80.5; 2886/358685.5; 2098/245369.5; 788/1133Children treated with an oral antimalarial at hospital discharge (%; n/N)85.9; 2479/288692.6; 1942/209868.2; 537/788Received antimalarial drug type (%; n/N)None14.1; 407/28867.4; 156/209831.9; 251/788Artemether-lumefantrine cp37.9; 1093/288626.7; 560/209867.6; 533/788Dihydroartemisinin-piperaquine cp47.8; 1380/288665.6; 1377/20980.4; 3/788Other (Quinine, ASAQ, SP)0.2; 6/28860.2; 5/20980.1; 1/788Proportion of children transfused (%; n/N)47.1; 3365/715253.5; 2347/438836.8; 1018/2764Proportion of severe anaemia transfused (%; n/N)88.2%; 3164/358688.7; 2175/245387.3; 989/1133Average haemoglobin levels in children transfused (standard deviation)4.98 (± 1.66)4.91 (± 1.54)5.15 (± 1.88)Median hospital stays in days (IQR)4 (2–6)3 (2–5)5 (3–7)Child’s vaccine status among severe clinical anemias (%; n/N)Up-to-date43.5; 1561/358649.5; 1214/245330.6; 347/1133Not up-to-date17.5; 628/358615.7; 384/245321.5; 244/1133Don’t know36.4; 1306/358633.4; 820/245342.9; 486/1133HIV test among severe clinical anemias (%; n/N)50.3; 1803/358634.9; 856/245383.6; 947/1133HIV-seropositive children (%; n/N)0.9; 44/18030.7; 26/8561.5; 18/947Mode of admission (%; n/N)Caregivers28.4; 1017/358626.1; 640/245326.1; 377/1133Referral from a hospital63.8; 2286/358666.6; 1633/245357.6; 653/1133The proportions of malaria test results are calculated only for children admitted with severe malaria who were tested.The proportions of haemoglobin levels are calculated only for children diagnosed with severe anaemia who had an Hb.Severe malaria anaemia is defined as the proportion of cases of severe anaemia who received parenteral antimalarial treatment in hospital during this episode.
Nearly all severe malaria cases were treated with injectable artesunate (3370/3653 [92.3%]). Malaria diagnostic confirmation, using either rapid diagnostic tests or thick blood smear, was positive in 80.4% of cases (2741/3409). The prevalence of clinical severe anaemia was 50.1% (3586/7152). Among these children, 49.3% (1628/3302) had haemoglobin levels < 5 g/dL (biological severe anaemia), with similar estimates across both hospitals (Table 1). Severe anemia prevalence was highest at the age of 2 years and remains above 10% for each groupe up to 4 years of age; and then decreases significantly after five years, it and drops below 5% (Fig. 1).Fig. 1. Distribution of severe anaemia in the two referral paediatrics hospitals according to age.
Severe malaria was identified as the primary cause of severe anaemia (79.0%). This proportion reached 88.7% (2175/2453) at CHU-MEL and 58.2% (659/1133) at CHD-Z. Most of the children recovered after treatment; however, 10.5% (376/3586) of those hospitalized with severe anaemia died, including 9.1% at CHU-MEL and 13.5% at CHD-Z. Among survivors, 92.6% (1942/2098) at CHU-MEL and 68.2% (537/788) at CHD-Z were prescribed antimalarial drugs upon hospital discharge. Dihydroartemisinin-piperaquine (DHA-PP) was the most commonly prescribed oral antimalarial at CHU-MEL (1377/2098 [65.6%]), whereas artemether-lumefantrine (AL) was the preferred regimen at CHD-Z (533/788 [67.6%]) (Table 1). Additionally, nearly half (3365/7152 [47.1%]), of the hospitalized children received a blood transfusion due to their clinical condition. The mean haemoglobin level among hospitalised children were 4.98 g/dl (± 1.66). (Table 1).
The median duration of hospitalisation was 4 days (Interquartile range [IQR]: 2–6) across both hospitals, with CHU-MEL showing a shorter median duration of 3 days (IQR: 2–5) compared to CHD-Z, where the median duration was 5 days (IQR: 3–7). Approximately 17.5% (638/3586) of children with clinical severe anaemia had incomplete vaccination records. HIV positivity was rare, with less than 1% of children testing positive. Additionally, 63.8% (2286/3586) of the children were referred from peripheral healthcare centres (Table 1). A significant number of hospitalised children (2964 out of 7152) had both severe anaemia and severe malaria. (Fig. 2).Fig. 2. Co-occurrence matrix for diagnoses of children admitted to paediatric hospitals in 2023.
Severe anaemia cases showed a seasonal pattern, with the highest cases occurring from May to September 2023. The peak incidence was observed in June-July, accounting for 20.7% of all severe anaemia cases at CHU-MEL. This trend was consistent across both sites (Fig. 3). Regarding spatial distribution, CHU-MEL received the highest number of severe anaemia cases from the communes of Abomey-Calavi (41.3%) and Cotonou (17.9%). In Abomey-Calavi, the Godomey (29.4%) and Hêvié (28.5%) arrondissements were the primary sources, while in Cotonou, the 12th arrondissement (17.9%) contributed the majority of cases. At CHD-Z, the commune of Bohicon was the most affected (27.8%), with the Bohicon I (33%) and Bohicon II (25.1%) arrondissements accounting for most severe anaemia admissions (appendix 2).Fig. 3. Temporal variation in severe clinical anaemia in paediatrics hospitals in 2023.
About one-in-ten children with severe anaemia (10.5%, 376/3586) died. Overall, mortality was particularly high when severe anaemia coexisted with malnutrition (29.3%) or cardiopulmonary diseases (28.3%). At CHU-MEL, mortality rates were higher when severe anaemia coexisted with comorbid conditions such as cardio-respiratory pathologies (30%), malnutrition (16.7%), or infectious syndromes (19.5%). Mortality was also notably high when severe anaemia occurred without any other associated morbidities (23.6%). At CHD-Z, mortality rate was also higher when severe anaemia coexisted with malnutrition (33.3%) or cardio-respiratory pathologies (26.7%). (Fig. 4).Fig. 4. Clinical outcome of children according to priority diagnoses.
In-hospital mortality related to severe anaemia was significantly associated with age, nutritional status, hospital visited and the presence of severe malarial anaemia. After adjusting for confounding factors, each additional year of age was associated with a 5% reduction in the risk of death (adjusted odds ratio [aOR] 0.95, 95% CI 0.92–0.99, p = 0.019). Children with severe malnutrition were 80% more likely to die (adjusted odds ratio [aOR] 1.80, 95% CI 1.34–2.43, p < 0.001). In addition, children without severe malaria-related anaemia were 4.70 times more likely to die than those with severe malaria-related anaemia (adjusted odds ratio [aOR] 4.70, 95% CI 3.74–5.89, p < 0.001) (Table 2).Table 2. Factors associated with death in children hospitalised for severe anaemia.Clinical characteristicsIn-hospital deathDescriptivesBi-variate analysisMultivariate analysisn/N%OR95%CIP-valueaOR95%CIP-valueAge (year)376/349510.80.930.89–0.96** < 0.0010.950.92–0.990.019Nutritional status < 0.001No malnutrition208/23328.91––1––Moderate malnutrition80/66612.01.391.06–1.830.0171.280.95–1.720.100Severe malnutrition88/49717.72.191.67–2.88 < 0.0011.801.33–2.43 < 0.001Severe malarial anaemia < 0.001**Yes200/283426.61––1––No176/6617.14.773.82–5.98 < 0.0014.703.74–5.89 < 0.001Referral hospitalCHU-MEL223/24189.21––CHD-Z153/107714.21.631.31–2.03 < 0.001Nutritional status: Assessed using WHZ, HAZ, and WAZ z-scores. Severe malnutrition: any z-score < − 3; moderate malnutrition: any z-score between − 3 and − 2; no malnutrition: all z-scores ≥ − 2. according to WHO standards.Significant values are in [bold].
Discussion
This study aimed to assess the prevalence and outcomes of severe anemia in children hospitalized in two referral hospitals in southern Benin. The burden of severe anemia was significant, with 4 out of 5 cases due to severe malaria. The hospital mortality rate was higher when severe anemia coexisted with malnutrition (29.3%). Additionally, age, the hospital visited, and malnutrition were strongly associated with an increased risk of hospital mortality.
Severe anemia was predominant among hospital admissions, accounting for half of the cases. This high hospital prevalence reflects the fact that hospitalized children often present more severe clinical conditions, such as severe malaria, malnutrition or bacterial infections, and are therefore different from the general paediatric population. Even so, this rate aligns with findings from other studies conducted in West and Central Africa^14,21^. In contrast, lower proportions of anemia have been reported in East Africa (e.g., Kenya and Tanzania) and North Africa (e.g., Sudan)^8,22,23^. Most of these studies, except for the one in Sudan, focused on children under 5 years old. The proportion of severe anemia peaked at two years of age, remained above 10% until four years, and then significantly declined after five years. In this study, 79% of severe anemia cases were diagnosed with severe malaria. In comparison, a keynian study conducted in 2007 reported a higher proportion, with 85% of severe anemia cases linked to severe malaria^8^. Beyond malaria, nutritional deficiencies, particularly iron deficiency, are significant contributors to severe anemia. Yessoufou et al*.* found that iron deficiency was responsible for 78.8% of severe anemia cases. Poor weaning practices and inadequate consumption of iron-rich foods further exacerbated the risk of nutritional anemia in this population^14^. However, the aetiology of severe anaemia in children is often multifactorial. In addition to nutritional deficiencies, other contributors include chronic inflammatory conditions, parasitic worm infestations (such as hookworm or schistosomiasis), and repeated infections, all of which can impair red blood cell production or increase destruction^24^. In severe malaria, high parasitemia combined with a strong inflammatory response can rapidly lead to severe haemolysis and bone marrow suppression, contributing to acute drops in haemoglobin levels^25^. Nearly half of the hospitalized children had been transfused (47.1%), reflecting the critical severity of anemia cases. This observation is slightly lower but consistent with previous studies conducted in Burkina Faso and Benin (CHU-MEL), which reported transfusion rates of 78% and 63%, respectively^26,27^.
The median hospital stay was four days, longer at CHD-Z compared to CHU-MEL. These prolonged stays are likely due to the need for comprehensive management, addressing both the immediate treatment of anemia and its underlying causes^22,28^. Mortality rates were higher when severe anemia was associated with comorbidities, such as cardio-respiratory diseases, malnutrition, or infectious syndromes. Notably, malnutrition was particularly associated with poor outcomes, as one-third of children with both severe anemia and malnutrition died at CHD-Z. Furthermore, hospital mortality related to severe anemia was strongly influenced by age, nutritional status and the presence of malaria-related anemia. Older children had a lower risk of death, while those suffering from malnutrition had a higher risk, particularly the most severely malnourished. Finally, children without malaria-related anemia had a significantly higher risk of death. This phenomenon may be explained by the fact that severe malaria-related anemia is generally identified quickly and treated according to well-established protocols, thereby reducing the risk of mortality. Conversely, when the underlying cause of anemia is not promptly identified or when hospital admission is delayed, the administration of appropriate care may be postponed, increasing the risk of death.
Severe malaria emerged as a co-principal cause of hospitalization, accounting for more than half of pediatric admissions, along with severe anemia. This finding aligns with studies conducted in Burkina Faso, where severe malaria represented 46% of pediatric admissions^26^, and in Kenya, where 83% of children under five were reported to have malaria parasitemia^8^. In Benin, severe malaria remains a major cause of hospitalization among children under five, as reported in similar studies^14,27^. The variability in malaria prevalence across regions can be attributed to several factors, including the implementation of malaria control measures, local vector resistance, differences in healthcare facilities, and geographical variations^29^.
Seasonal variations in severe anemia cases were observed, with peaks between May and September, particularly in June and July, corresponding to the rainy season. This period coincides with a well-documented increase in malaria cases in endemic regions^28^. In this context, the PDMC-SL study, based on the WHO’s new recommendation for post-hospitalization malaria chemoprevention in children treated for severe anemia, holds great potential, especially in malaria-endemic areas. This approach aims to prevent malaria recurrence and its associated complications in vulnerable populations. However, its efficacy and feasibility need to be thoroughly evaluated before broader adoption, including determining the optimal drug regimen and implementation strategies. The PDMC-SL implementation trial will be essential in addressing these gaps, generating context-specific data to inform its application in Benin^30^.
This study has certain limitations that may affect the interpretation of its results. Firstly, the lack of precise data on the delay between symptom onset and hospitalization limits the understanding of healthcare-seeking behaviors influencing severe anemia outcomes. The hospital-based study design may not accurately represent the prevalence of severe anemia among children who do not seek care or are treated in other healthcare facilities. Additionally, the focus on data from two referral hospitals, identified in the PDMC-SL study, limits its representativeness. Furthermore, retrospective data extracted from medical records may be affected by information quality, including incomplete documentation or transcription errors. Despite these constraints, the study provides crucial epidemiological insights into severe anemia in southern Benin, contributing to future control and optimization efforts within the PDMC-SL framework. It also highlights the need to adopt an integrated approach, including the treatment of underlying causes of anaemia, particularly in young children, and other key factors such as the promotion of good nutrition.
Conclusion
Severe anaemia remains a major cause of paediatric hospital admissions in southern Benin, with mortality influenced by younger age, malnutrition and the underlying cause of anaemia. Each additional year of age is associated with a reduced risk of death, highlighting the increased vulnerability of the youngest children. Malnutrition also plays a key role, with severely malnourished children running a significantly higher risk of death. In addition, children with severe non-malarial anaemia have an increased risk of death, probably due to delays in diagnosis and treatment, whereas well-established protocols for malaria-related anaemia may have a protective effect. These findings underscore the need for an integrated approach that combines prompt malaria diagnosis and treatment with robust nutritional support. Strengthening early detection of non-malarial causes of anaemia and improving overall care strategies by management of underlying causes of anemia, promotion good nutrition, worm control and multivitamin supplementation are essential to reduce mortality. Further research is needed to improve our understanding of the epidemiology of severe anaemia and to inform the development and optimisation of targeted public health strategies within frameworks such as the PDMC-SL to improve prevention and treatment outcomes for vulnerable paediatric populations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Organisation Mondiale de la Santé (OMS). Anémie [Internet]. 2023 [cité 7 oct 2024]. Disponible sur: https://www.who.int/fr/news-room/fact-sheets/detail/anaemia
- 2Global Health Metrics. Institute for Health Metrics and Evaluation. [cité 7 oct 2024]. Anémie—Déficience de niveau 1|Institut de mesure et d’évaluation de la santé. Disponible sur: https://www.healthdata.org/research-analysis/diseases-injuries-risks/factsheets/2021-anemia-level-1-impairment
- 3JEAI TILAPIA : Paludisme grave: formes cliniques ; étiologies des Anémies et des sepsis associés, en pédiatrie. | Site Web IRD. [cité 7 oct 2024]. Disponible sur: https://www.ird.fr/jeai-tilapia-paludisme-grave-formes-cliniques-etiologies-des-anemies-et-des-sepsis-associes-en
- 4Institut National de la Statistique et de l’Analyse Économique (INSAE) et ICF. Enquête Démographique et de Santé au Bénin, 2017–2018. Cotonou, Bénin et Rockville, Maryland, USA: INSAE et ICF. [cité 7 oct 2024]. Disponible sur: https://instad.bj/images/docs/insae-statistiques/enquetes-recensements/EDS/2017-2018/1.Benin_EDSBV_Rapport_final.pdf (2019).
- 5World Health Organisation Global Malaria Programme. WHO guidelines for malaria. Disponible sur: https://iris.who.int/handle/10665/354781 (2022).
- 6Severe Malaria Observatory. Knowledge sharing for severe malaria. Severe Malaria Criteria, Features & Definition. Disponible sur: https://www.severemalaria.org/severe-malaria/severe-malaria-criteria-features-definition
- 7World Health Organization (WHO). Guidelines for the treatment of malaria. Third edition|WHO |Regional Office for Africa. Disponible sur : https://www.afro.who.int/publications/guidelines-treatment-malaria-third-edition (2024).
- 8World Health Organization (WHO). Malnutrition. Disponible sur: https://www.who.int/news-room/fact-sheets/detail/malnutrition (2024).