The effect of Photobiomodulation therapy on implant stability in patients receiving dental implants- a systematic review and meta-analysis
Ashika Singhania, Anjali Borle, Surekha Godbole, Seema Sathe

TL;DR
This study reviews and analyzes the impact of photobiomodulation therapy on dental implant stability in patients, finding mixed results that suggest more research is needed.
Contribution
The paper provides a systematic review and meta-analysis of PBM therapy's effect on implant stability, revealing inconsistent outcomes across time intervals.
Findings
At 2, 4, and 8 weeks, the control group showed better implant stability than the PBM group.
At 3 weeks, the PBM group showed better implant stability than the control group.
No significant difference was observed between groups at 6 and 12 weeks.
Abstract
The use of photobiomodulation (PBM) therapy in implant dentistry for enhancing the osseointegration is proven in many studies. However, the cumulative data of its effect around dental implants in patients is limited. The purpose of the present study was to evaluate the effect of the PBM therapy on primary and secondary implant stability. The studies included in the review and meta-analysis were selected according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the PICOS criteria. The RoB 2 tool was used for assessing the risk of bias and the RevMan software, v. 5.4, was used for meta-analysis. Quantitative analysis was done using two tools considering the implant stability measurement using Ostellmeter and radiographs as the outcome. The mean and standard deviation (M ± SD) values for implant stability as well as the sample size were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
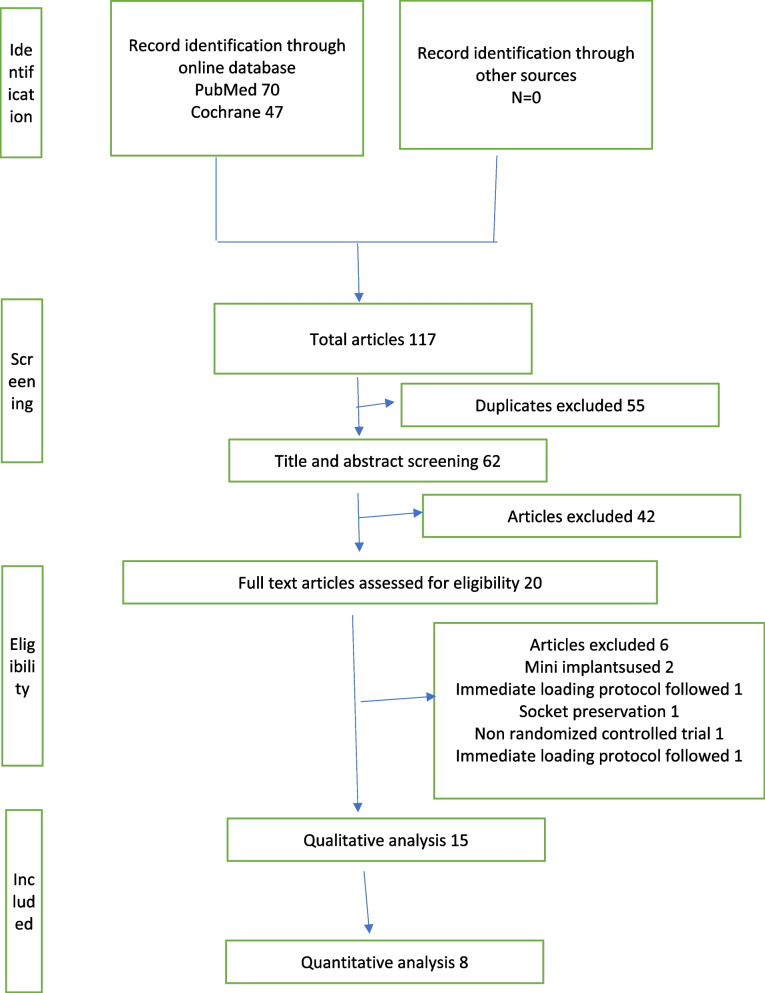 Figure 1
Figure 1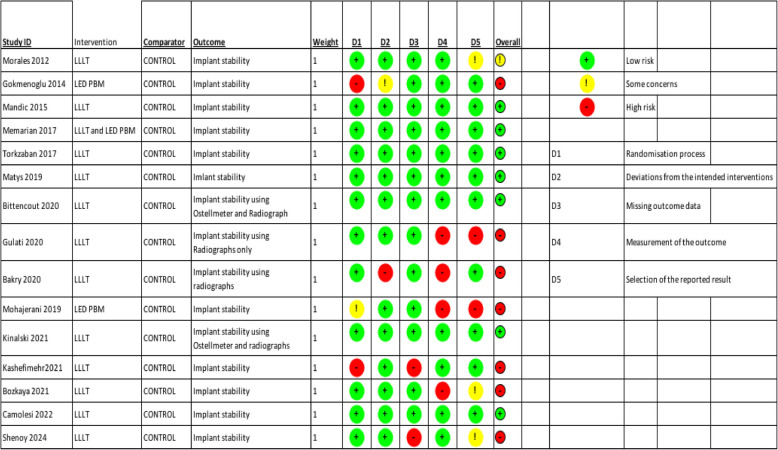 Figure 2
Figure 2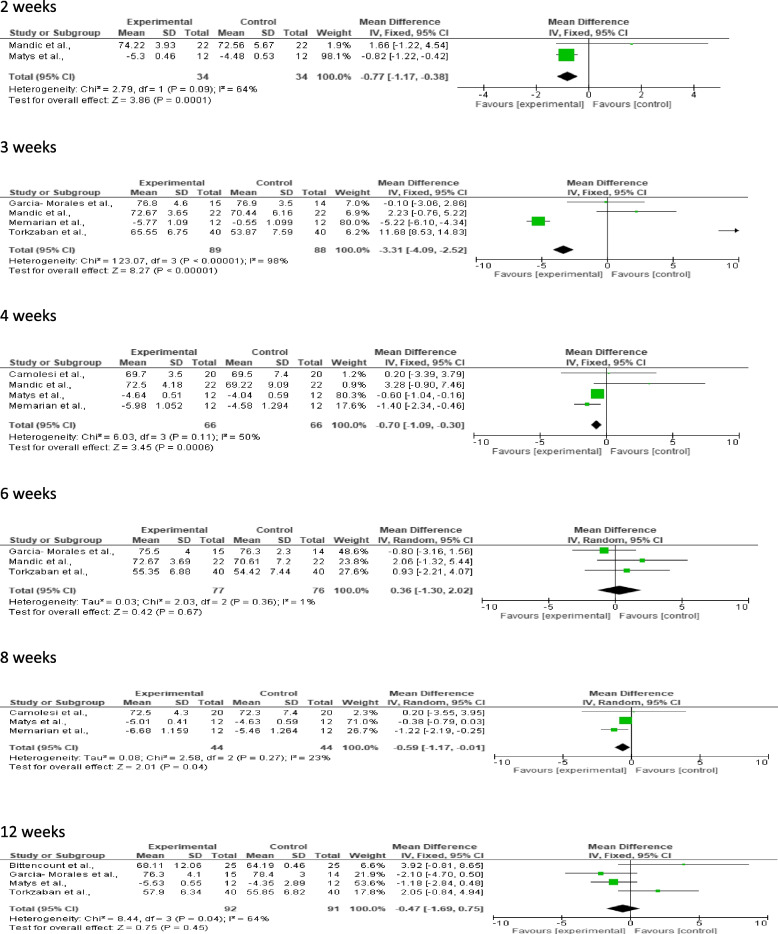 Figure 3
Figure 3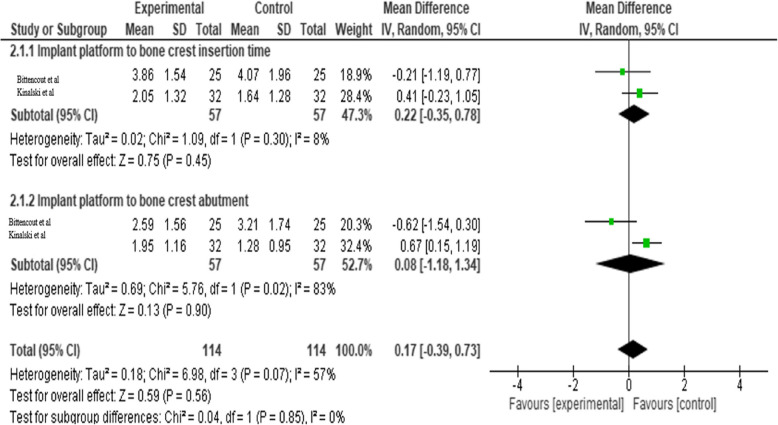 Figure 4
Figure 4- —Datta Meghe Institute of Higher Education and Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLaser Applications in Dentistry and Medicine · Dental Implant Techniques and Outcomes · Dental materials and restorations
Introduction
Humans have always had to deal with tooth loss, and in the modern world, as life expectancy has increased, so has the impact of age on tooth loss. For people of all ages, attempts to replace lost teeth have proven essential, and Branemark has accomplished this by developing endosseous dental implants. He identified the phenomenon known as osseointegration—the tight bond between titanium implants and bone that is strong enough to transfer force [1]. According to biological theory, osseointegration is an immune-driven process that produces new bone and for protecting the implant from the surrounding tissues, the immune system first perceives the implant as a foreign body and then builds bone around it [2]. Preliminary guidelines indicate that 3–4 months will pass after implant insertion for healing. Because there is more cancellous bone in the maxilla and posterior mandible, this process takes longer and could take up to six months. The key requirement for implant loading is that the implant must have sufficient primary stability at the moment of implantation. Dental implants'primary stability is influenced by a number of parameters, including as surface topography, implant morphology, bone quantity and quality, and surgical technique [3]. Both the surgical approach and the characteristics of the dental implant affect secondary stability. However, secondary stability is also directly impacted by primary stability. Determining the optimal loading time thus requires evaluating implant stability at various time periods [4].
Implants frequently lack the ideal circumstances for both the amount and quality of bone. Photobiomodulation, or low-energy photon irradiation by light in the far-red to near-infrared (NIR) spectrum (630–1000 nm) utilizing low-energy lasers or light-emitting diodes (LED), is one of the potential techniques to promote osseointegration. When cytochrome c oxidase, a photoacceptor molecule in the mitochondria, absorbs light, it changes the cellular process and increases the generation of adenosine triphosphate (ATP), which promotes wound healing in injured and ischemic tissues [5]. This light source is necessary for the activation of the light sensitive substance (PS) by exposing a low power light at visible wavelengths and activating it. Additionally, it promotes osteoblast development and proliferation, which biostimulates bone tissue. PBM has been investigated for its possible use in implant dentistry to enhance implant stability and the general healing of the hard and soft tissues surrounding dental implants. LLLT has been shown to have a beneficial effect around the implant in a number of in vitro and animal investigations [6]. This systematic review and meta-analysis were conducted on the basis of clinical studies to evaluate the qualitative and quantitative effect of PBM on implant stability.
Methods
This systematic review and meta-analysis were performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [7]. The review protocol was registered under PROSPERO International Prospective Register of Systematic Reviews (CRD42024427943).
Study design
Randomised controlled trials(RCT’s) on humans.
Search strategy
The search strategy was based on the PICO criteria due to the comparative nature of the study: Population(P): male or female patients requiring the replacement of one or more missing teeth with dental implants, Intervention(I): the PBM therapy around dental implants, Comparison(C): patients who did not receive PBM or any other adjunctive therapy around dental implants, Outcome(O): the effect of the PBM therapy on primary and secondary implant stability. An advanced search of electronic databases was carried out by 2 investigators individually without consulting one another. The following terms were searched in all data bases, in Pubmed and Cochrane the search strategy followed was as follows. For population following search terms were used"low intensity laser therapy"[Title/Abstract] OR"low intensity laser therapy"[Title/Abstract] OR"low level laser therapy"[Title/Abstract] OR"low level laser therapy"[Title/Abstract] OR"photobiomodulation*"[Title/Abstract] OR"Photobiomodulation therapy"[Title/Abstract] OR"low level light therapy"[Title/Abstract] OR"low level light therapy"[Title/Abstract] OR"low level light therapy"[MeSH Terms]. For intervention following search terms were used"dental implant*"[Title/Abstract] OR"implant*"[Title/Abstract] OR"dental implantation"[MeSH Terms]. In The electronic databases were searched for articles published till January 2024. To avoid missing any eligible studies, the references of all eligible articles were also searched. The grey literature was also searched using Proquest and Google scholar and no relevant data was found. The data of 117 articles was uploaded on Rayyan where two blinded investigators screened the abstracts, removed 55 duplicates, title and abstract screening was done for 62 articles. Later eligible articles fulfilling the inclusion criteria were further assessed by accessing their full text from relevant sources by 2 investigators individually. Any discrepancy between 2 investigators was resolved by a third investigator. The qualitative analysis was done for 15 articles and quantitative analysis was done for 8 articles.
Inclusion and exclusion criteria
This review focussed on randomised controlled trials (RCT) or quasi RCT on humans reporting the effects of Photobiomodulation on primary and secondary implant stability assessed using Ostellmeter in ISQ scale and Radiographs. RCT that used LED as photobiomodulation therapy was excluded, also case reports, review papers, clinical trials, letters to editors, monographs, in vitro studies, animal studies.
Data collection and analysis
The following information was extracted from the studies included in this review by 2 independent reviewers: first author(year),country, sample size, study design, mean age of patient, implant site, type of implant, outcome, evaluation time, study conclusion. Another data extraction was done for the laser parameters which included: Study, type of LLLT, wavelength, mode, output/energy density, irradiation time and energy per point and number of points, total energy per session, frequency of laser treatment.
Statistical analysis was conducted using RevMan version 5.4 provided by Cochrane collaboration [7]. The meta‑analysis was conducted using the fixed‑ or random‑effects methods. Fixed‑effects meta‑analysis was used when the heterogeneity was small (I2 < 50%, P < 0.05). When the heterogeneity was large (I2 > 50%, P > 0.05), a random‑effects model analysis was undertaken considering 95% confidence interval. If a meta-analysis could not be performed, data was summarized qualitatively.
Risk of bias assessment
The risk of bias of all the studies included in the review was assessed by two investigators who were blinded, using the Cochrane risk of bias assessment tool [8]. The agreement between reviewers was assessed based on Cohen’s kappa statistics, assuming k = 0.6 to be an eligible score [9]. According to ROB 2 tool, 5 domains were taken into consideration to evaluate each article in terms of risk of bias, namely randomisation process, deviation from intended interventions, missing outcome data, measurement of outcome, selection of the reported results. Accordingly the risk of bias of particular studies was calculated as high, low or unclear [10].
Results
During the search process, a total of 117 articles were identified (Fig. 1) from electronic databases, out of which 62 articles remained after removal of 55 duplicates. 42 articles were excluded based on exclusion criteria and at the end of study selection, 15 articles were selected for qualitative analysis [1, 3, 5, 13–24] and 8 articles for quantitative analysis [2, 11–15, 19, 21].The inter-investigator reliability in the selection of articles was statistically evaluated using Cohen’s kappa analysis and a score of 0.97 was obtained.Fig. 1. Flowchart depicting the study selection process
The risk of bias in the study included in the review was assessed according to the ROB2 tool (Table 1). Out of 15 studies, 6 studies showed high risk of bias [1, 4, 16–18, 20, 22], 1 study showed some concerns [11]and 7 studies were low risk of bias [2, 12–15, 19, 21].In the high risk studies, 2 studies had missing outcome data (D3) [1, 4, 22], studies had different outcome measurement(D4) 16–18, 20] and 2 studies did not adhere with randomisation process (D1) [1, 4].
Table 1. Risk of bias assessment of the included studies with the use of the RoB 2 tool
Characteristics of systematic review
All the articles included in the systematic review were randomised controlled trials, and were published between 2012 and 2024. Six studies had a split mouth design [1, 11–13, 20, 22 ] whereas 9 studies had a case control design [2, 4, 14–19, 21]. The studies were conducted in Brazil, Turkey, Serbia, Iran, Poland, India, Egypt, Spain. In 5 studies implant placement was done in mandible [11, 13, 14, 16, 18] in 3 studies implant was placed in maxilla [2, 12, 17] and in 3 studies bilateral mandibular or maxillary implants [1, 20, 22] was placed and implant site was not mentioned in 4 studies. The primary outcome, implant stability was assessed in ISQ scale in 11 studies, in 2 studies PTV value was assessed. The implant stability was assessed using Ostellmeter in majority of studies. In 2 studies implant stability was assessed radiographically, Gulati et al. assessed using IOPA and CBCT and Bakry et al. assessed using RVG. In study by Mandic et al., Alkaline phosphatase level was also assessed, Memarian et al. assessed GCF fluid for levels of IL‐1β and PGE2 markers, Bakry et al. assessed the probing depth, Bozkaya et al. assessed the microbiological changes, Camolesi et al. assessed the post-surgical healing and inflammation. In the CBCT analysis by Matys et al., the bone density level(grayscale value) was measured at three levels cervical, middle and apical and in the CBCT analysis by Gulati et al., average crestal bone level value was made on four anatomical sites mesial, distal, buccal and lingual. In IOPA analysis by Bittencout et al., Bakry et al. and Kinalski et al. implant platform to bone crest measurement at insertion time and abutment stage was recorded whereas Gulati et al. did IOPA assessment in mesial and distal site. The evaluation period was different for all the studies and varied from baseline to 1 year (Table 2).
Table 2. Characteristics of included studiesAuthor(Year)CountrySample sizeStudy designMean ageImplant siteType of implantBone typeOutcomeEvaluation timeStudy conclusionMorales et al. 2012BrazilLG 15CG 14Split mouth36Posterior mandibleDentsply, Germany with diameter of 3.8 mm and a length of 11 mmImplant stability in ISQ scalebaseline, 10 days, 3, 6, 9, and 12 weeksno effectGokemenoglu 2014TurkeyLG 10CG 12Case control48Dentsply, Manheim, GermanyType 2 or 3Implant stability in ISQ scaleimmediately, 2, 4, 8 and 12 weeks postoperativelypositive effectMandic 2015 [12]SerbiaLG 20CG 20Split mouth61posterior maxillaBredent, Senden, GermanyImplant stability in ISQ scale, Alkaline phosphatase level and early implant success rateImplant stability: immediately and 1, 2, 3, 4, 5, 6 weeks postoperativelyPICF: postoperative, 7, 14, 21, 28 daysEarly implant success rate: 6 weeks postoperativelyno effectMemarian 2018 [13]IranLG 12LG 12CG 12Split mouthanterior mandibleDio, Busan, South KoreaType 2 or 3implant stability (PTV) and GCF fluid for levels of IL‐1β and PGE2 markersimplant stability: day of surgery, 3, 4, and 8 weeks after surgeryInflammatory markers: 4 and 8 weeks postoperativelypositive effectTorkzaban 2018IranLG 40CG 40Case control42maxillaDio, Busan, South KoreaD3, D4Implant stability in ISQ scaleimmediately, 10 days, 3, 6 and 12 weeks postoperativelyno effectMatys 2019 [14]PolandLG 18CG 22Case control47posterior mandibleDentium, cypress, USAD2implant stability(PTV) and CBCTPTV: after surgery, 2 weeks, 4 weeks, 2 months and 3 months after surgeryCBCT: after surgery, 4 weeks and 3 months after surgerypositive effectBittencount 2019BrazilLG 23CG 23Case control51Straumann, Basel, SwitzerlandImplant stability in ISQ scale and IOPAduring implant placement and at abutment selection phaseno effectGulati 2020 [16]IndiaLG 10CG 10Case control35posterior mandibleAdin Dental, Polandtype 2 or 3implant stability using IOPA and CBCTIOPA: immediately, 6 weeks, 6 months and 1 year following prosthesis loadingCBCT: immediately and at 1 yearpositive effectBakry 2020 [17]EgyptLG 6CG 6Case control40posterior maxillaZimmer Dental, Carlsbad, USAcrestal bone level using RVG, clinical parameters probing depthbaseline, 2 weeks, 3 months, and 6 monthsno effectMohajerani 2020IranLG 28CG 28Case control38posterior mandibleZimmer Dental, Carlsbad, USAImplant stability in ISQ scaleimmeditaley, 10, 21, 42 and 63 days postoperativelypositive effectKinalski 2021 [19]BrazilLG 32CG 32Case control49.94Alvim CM, Neodent Straumann, Curitiba, BrazilImplant stability in ISQ scale and Digital radiographsbaseline, at sbutment selection phase(4–6 months)no effectKashefimehr 2021 [1]IranLG 12CG 12split mouth44.75bilateral mandibular or maxillary implantsDio, Busan, South KoreaType 3 or 4Implant stability in ISQ scaleimmediately, one month and 3 monthspositive effectBozkaya 2021 [20]TurkeyLG 47CG 46split mouth55bilateral mandibular or maxillary implantsStraumann Stan- dard Plus Implant; Institute Straumann AG, Waldenburg, Switzerland)Implant stability in ISQ scale and microbiological changesbaseline, 30, 60 and 90 daysno effectCamolesi 2022SpainLG 20CG 20Case controlModel IPX, Nueva GalimplantType 1, 2, 3, 4Implant stability in ISQ scalePost-surgical healing and inflammationimmediately, 7 days, 4 weeks, 8 weeksno effectShenoy 2024 [22]IndiaLG 20CG 20split mouth18–65bilateral mandibular or maxillary implantsOsstem implant TS III SA, Osstem Implant Co., Seoul, KoreaImplant stability in ISQ scale1, 2, 4 and 12 weeks postoperativelypositive effect
The type of laser and protocol used for PBM is presented (Table 3). Diode lasers used in all the studies varied from 626-980nm. The time of laser application varied in all the studies ranging from before placement to 24 days after implant placement. Table 3. Laser specificationsStudyType of LLLTWavelengthModeOutput/Energy densityirradiation time and energy per point and number of pointstotal energy per sessionfrequency of laser treatmentMorales 2012GaAIAs laser830 nmcontact continuous86 ± 2 mW, 92.1 J/cm2irradiation time per point: 3 stotal points: 20 (9 at the vestibular, 9 at the lingual, 1 at mesial and 1 at distal)energy per point: 0.25 J per point, 5 J per implant8 Jimmediately, 2, 4, 8,10, 12 and 14 daysGokemenoglu 2014LED(Osseopulse Ar 300)626 nmNR100 mW, 28.37 J/cm2irradiation time per point: 20 mintotal points: 2 (buccal and lingual)energy per point: 20 J/cm2222 J3 times per week for 3 weeksMandic 2015 [12]GaAIAs laser637 nmcontact continuous40 mW, 6.26 J/cm2immediately after surgery, 1, 2, 3, 4, 5, 6, 7 days laterMemarian 2018 [13]Diode laserLaser: 810 nmLED: 626 nmcontact continuousLaser: 50 mWLED: 185 mWirradiation time per point: Laser 400 s, LED 20 mintotal points: 2 (buccal and lingual)energy per point: 20 J/cm2,222 Jday of surgery, 3, 7, 10 and 14 daysTorkzaban 2018Biolase diode laser940 nmcontact continuous100 mW, 354.6 J/cm2irradiation time per point: 40 stotal points: 2 (buccal and lingual)energy per point: 4 J56 Jimmediately, 2, 4, 6, 8, 10 and 12 days after insertionMatys 2019 [14]red diode laser635 nmcontact continuous100 mW, 99.04 J/cm2irradiation time per point: 40 stotal points: 2 (buccal and lingual)energy per point: 4 J56 J1 day before surgery, immediately after surgery, 2, 4, 7 and 14 days laterBittencount 2019GaAIAs laser808 nmcontact continuous50 mWirradiation time per point: 1.23 mintotal points: 6 (2 buccal, 2 lingual and 2 occlusal)energy per point: 11 J66 Jbefore implant placement after suturingGulati 2020 [16]GaAIAs laser980 nmcontact continuous0.1 Wirradiation time per point: 1.23 mintotal points: 6 (mesiobuccal, distobuccal, midbuccal, mislingua, mesial, distal)energy per point: 1 J6 Jafter implant placement, 3, 7 and 14 dayBakry 2020 [17]smart M lasotronix Pro diode laser980 nmcontact continuous2 Wirradiation time per point: 5 mintotal points: buccal, lingual as well crestal surfacestwo weeks before implant placement, 2, 4, 6, 8, 10, 12, 14, 16, 18, 20, 22, 24 days postoperativelyMohajerani 2020LLLT and LED device830 nm laser with 632 nm LEDcontact continuousLaser 15 mW/cmsq LED 10 mW/cmsqirradiation time per point: 20 mintotal points:four points around the implantsEveryday for 10 daysKinalski 2021 [19]GaAIAs laser808 nmcontact continuous50 mWirradiation time per point: 80 secstotal points: 6 points in the labial region where the implant would be placed (apical and cervical): two points in the lingual region (apical and cervical) and two points in the occlusal directionenergy per point: 1 J66 JBefore implant placement after suturingKashefimehr 2021 [1]LED(Osseopulse Ar 300)626 nmirradiation time per point: 20 min1 days before surgery, 10 days consecutive sessions including day of surgeryBozkaya 2021 [20]GaAIAs laser830 nmnon contact continuous with application distance 0.5 to 1 cm300 mWirradiation time per point: 3 stotal points: 20 points in the eight points at the vestibular, eight points at the lingual, two at the distal, and two at the mesial region of the implantenergy per point: 0.3 J6 Jimmediately and 3 times a week for 15 daysCamolesi 2022GaAIAs laser630 nm and 808 nmcontact continuous100 mWirradiation time per point: 100 stotal points: Three points were irradiated: the buccal side (4 J) and the palatal or lingual side (4 J) using the infrared light mode (808 nm) and the occlusal side (2 J) using the red- light mode (630 nm)energy per point: 0.1 J10 Jimmediately and after 7 daysShenoy 2024 [22]GaAIAs laser940 nmcontact continuous100 mWirradiation time per point: 40 stotal points: 2 (buccal and lingual)energy per point: 14.18 J/cmsq8 Jimmediately, 2, 4, 6, 8, 10 and 12 days after insertion
Meta-analysis
A meta-analysis was performed to evaluate the effect of PBM therapy on implant stability measured in ISQ or RFA scale and using Radiographs. The analysis was divided into two outcomes and each outcome was divided into subgroups based on evaluation time of the implant stability. At 2 weeks, 4 weeks and 8 weeks, the control group demonstrated significantly higher implant stability compared to the experimental group and statistically significant result (p = 0.0001, p = 0.0006, p = 0.04). There was low to moderate heterogeneity seen with I^2^ = 23% at 8 weeks, I^2^ = 50% at 4 weeks and I^2^ = 64% at 2 weeks. At 3 weeks, the implant stability significantly favoured the experimental group with p < 0.00001 but the heterogeneity being high I^2^ = 98%. At 6 weeks and 12 weeks, there was no statistical significant difference seen between the groups (p = 0.67, p = 0.45) and heterogeneity being I^2^ = 1% at 6 weeks and I^2^ = 64% at 12 weeks (Table 4). Table 4. Forest plots of dental stability for experimental (laser) and control groups at 2 weeks, 3 weeks, 4 weeks, 6 weeks, 8 weeks, and 12 weeks
In the second outcome, where the implant stability was assessed using radiographs. The overall result and heterogeneity of implant platform to bone crest at insertion time was statistically not significant (p = 0.45, p = 0.30 I^2^ = 8%). The overall result was statistically non-significant and heterogeneity of implant platform to bone crest at abutment stage was statistically significant (p = 0.90, p = 0.02 I^2^ = 57%). The overall pooled mean difference between the groups was 0.17 with 95% CI (−0.39, 0.73) which was found to be not significant statistically (p = 0.86) (Table 5). Table 5. Forest plots of dental stability using IOPA for experimental (laser) and control groups at insertion time and at abutment time
Discussion
There are not many systematic reviews and meta-analyses conducted evaluating the effect of PBM therapy on implant stability and also the implant stability assessed using radiographs is not assessed in these meta-analyses. This review was conducted to evaluate the effect of PBM therapy on implant stability. Out of various techniques to assess the implant stability, the RFA technique is routinely used in clinical practice because it is easy to perform and also there is strong correlation between RFA and histomorphometric measures. Other than this insertion torque values, reverse torque test, percussion test, CBCT, radiography, and histomorphometric analysis are some of the techniques utilized to evaluate the stability of the implant. Among these the most reliable are ISQ, PTV and meta-analysis is conducted for same but digital assessment through CBCT and radiographs are also included in these meta-analyses. Out of all the studies assessed for meta-analyses, positive effect was seen in 2 studies [13, 14] and other studies showed no significant difference or effect. Another meta-analysis conducted by Remisio et al. which included all preclinical studies where assessment of osseointegration was done. There was no statistical difference between studies at the 2 month follow-up (p = 0.672) but this difference was significant at 1 and 3 months (p < 0.001) [25]. Similarly in the present meta-analysis, the studies included for qualitative analyses and not for quantitative analysis, 5 studies showed positive effect [1, 4, 16, 18, 22].
The studies by Gokmenoglu et al., Mohajerani et al. [4, 18] used LED for their intervention group, although it gave a positive effect but other studies gave intervention only through PBM therapy. Using the same wavelength of 980 nm, Gulati et al. and Bakry et al. [16, 17] found different results. This could be because histological observations and gene expression analyses showed that 980 nm diode laser irradiations reduced the number of inflammatory cells and accelerated bone regeneration by increasing the number of fibroblasts and osteoblasts [26]. By evaluating the PTV value and CBCT, Matys et al. [14] shown a favorable effect between the laser and control group in their study. The data show that the stability of the bone healing process typically decreases, rises, or plateaus in the weeks that follow. After three months, the secondary stability measured in the laser group was higher than at the baseline, whereas it was lower in the control group. Torkzaban et al. and Shenoy et al. [2, 22] used the same wavelength of 940nm in their study and the irradiations given were also of the same days but Shenoy et al. showed positive effect which may be due to LLLT may vary due to individual patient factors and individual variables. Crestal bone loss was assessed by Matys et al., Bittencount et al., Gulati et al., Bakry et al. and Kinalski et al. but there was variability of assessment where only Matys et al. and Gulati et al. did the CBCT assessment and showed positive effect and IOPA analysis was done by others.
As shown in the meta-analysis statistically significant results were not observed when the overall result between the studies was assessed. This could be the result of non-homogeneity in the laser parameters—wavelength, mode, output, energy density, exposure duration, and treatment frequency—that were employed in the various experiments. Moreover, a split mouth design was used in many trials, which dispersed laser energy and could have an impact on the outcomes [1, 11–13, 20, 22]. Hence a standardised protocol for PBM therapy should be implemented.
Limitations of study
This systematic review included 15 articles eligible for qualitative analysis, but only 8 articles met the criteria for quantitative analysis, which may limit the robustness of the findings. Notably, the baseline parameters across studies exhibited significant variability, particularly regarding evaluation time, study design, and bone type. These discrepancies resulted in inconsistent baseline parameters, which may have influenced the collected data and analysis of results, especially with regards to implant stability. Given these limitations, further research in this field is warranted, and a future review incorporating a larger, more homogeneous dataset would be valuable to provide more definitive conclusions.
Directions for future research
There should be more high-quality RCT done in light of the aforementioned limitations. Patients'bone health and the PBMT criteria ought to be covered in full. The study's findings should be appropriately reported, and any missing data should allow for the substantial conducting of meta-analyses.
Conclusion
Studies currently conducted do not provide a standardized procedure for PBM to improve implant stability or success rates in people. It would be very beneficial to further investigate this technology using other implant systems and characteristics, as well as varied bone states, LLLT parameters, and follow-up period durations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sterne JA, Savović J, Page MJ, et al. Ro B 2: A revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l 4898. 10.1136/bmj.l 489810.1136/bmj.l 489831462531 · doi ↗ · pubmed ↗
- 2Shenoy A, Ganapathy D, Subhabrata Maiti. Effectiveness of Photobiomodulation With Low-Level Laser Therapy on the Implant Stability Quotient at Different Time Intervals: A Randomized Clinical Trial. Curēus. 202410.7759/cureus.52160 PMC 1085906138344646 · doi ↗ · pubmed ↗