Individual household-level dynamics and caries experience among young children in peru. a cross-sectional study
Luis Limo, Lupe Antonieta Vargas-Zafra, Ronald Espíritu Ayala-Mendívil

TL;DR
This study found that household factors like renting a home or living in a single-parent household are linked to higher rates of early childhood tooth decay in Peru.
Contribution
The study identifies specific household dynamics associated with early childhood caries and explores differences based on the severity of dental lesions.
Findings
Children in rented homes had a 29% higher prevalence of ECC.
Single-parent households were associated with a 75% higher ECC prevalence.
Non-cavitated lesions were more linked to family structure and size than cavitated lesions.
Abstract
We aimed to assess the association between household dynamic factors and early childhood caries (ECC) experience, and whether these associations differ based on the extent of dental tissue damage. We analyzed data from 210 children aged 3-5 years in Callao, Peru, using questionnaires and dental examinations. Household dynamics included house ownership, parental living arrangements, family structure, and family size. ECC experience was assessed by clinically examining decayed, filled, or missing primary teeth, including cavitated and non-cavitated lesions. Covariates included demographic, socio-economic, health behaviours, and access to dental care. Block-wise multivariable regression models with prevalence ratios and 95% CI were used, following STROBE guidelines. Fully adjusted estimates showed that the prevalence of ECC experience was higher among children living in rented…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
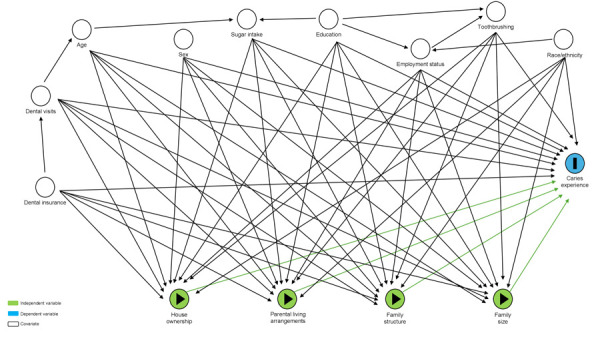 Figure 1
Figure 1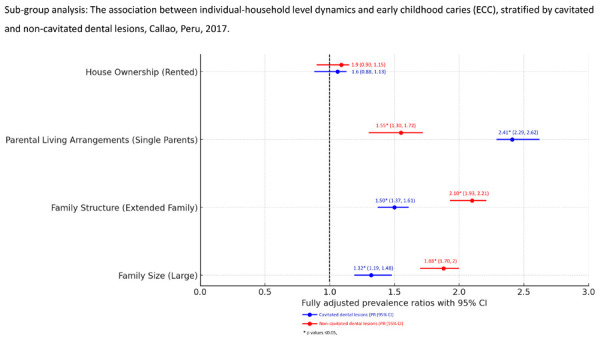 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Health and Care Utilization · Aging, Health, and Disability · Public Health and Environmental Issues
INTRODUCTION
Oral diseases are a major public health concern, as the recent WHO Global Oral Health Status estimated that they affect close to 3.5 billion people worldwide, with dental caries being the most prevalent chronic diseases in children, particularly affecting those coming from lower socio-economic positions 1. Importantly, the consequences of early childhood caries (ECC), defined as the presence of a primary tooth with one or more caries lesions (cavitated or non-cavitated), missing (due to caries), or filled surfaces in a child under the age of six years 2, include negative impacts on growth, development, nutritional problems, and oral health-related quality of life issues 3. Previous studies have suggested that children with dental caries tend to have poorer school performance and lower school attendance rates 4. Particularly, last available data from Peru, shows that high rates of ECC have been reported, revealing significant oral health inequalities, with a 59.1% of children with primary dentition diagnosed with dental caries 5.
Similar to other chronic conditions, dental caries is recognized as a multifactorial disease, influenced by an interplay of biological, health behaviours, and socio-environmental factors 6^,^7. Among these, household dynamics play a crucial role in shaping children's oral health outcomes, particularly in vulnerable populations 8. Household dynamics, including parental living arrangements, family structure, household ownership, and family size, are hypothesized to be determinants of a child's oral health 9^-^11. According to the 2017 Demographic and Familiar Health Survey (ENDES), in Peru, the family dynamic and household structure vary largely based on social classes and geographic regions. For instance, the nuclear family is the most common household unit and varies in size depending on the family’s geographic location. A significant proportion of children live with both parents, although there is a growing trend of single-parent households, particularly in urban areas 12. Lima households often consist of nuclear families, but there is a growing number of single-parent and extended family households, with an average family size of approximately 3.5 members. Around 30% of households have children under the age of 18, and single-parent households, primarily headed by women, make up about 20% of all households with children 12.
The Social Determinants of Health (SDH) framework, posits that health outcomes are influenced by the conditions in which people are born, grow, live, work, and age 13. According to this framework, socio-environmental factors including family interactions are pivotal in determining health outcomes, including oral health 14. Several frameworks addressing childhood health development have integrated family functioning as a crucial element theoretically impacting the development of children's oral health as well as the adoption of preventive oral health behaviours 15^,^16. The family’s role has predominantly been examined from behavioural, cognitive, and to a lesser extent, psychosocial perspectives, focusing on aspects such as parental oral health practices, knowledge, attitudes, and social status, rather than specific household dynamic interactions. Previous research suggest that close family interactions, characterized by supportive and cohesive relationships, may be associated with healthy behaviours, and subsequently, provide emotional and practical support for maintaining oral hygiene practices 17^,^18. However, little is known whether household dynamics, as the primary and fundamental socio-environmental factor in an individual’s life, could have an impact on the early onset of dental caries in young children. The aim of our study was to estimate the extent of the association between each of the individual-household level dynamics indicators and ECC experience among children aged 3-5 years old living in the province of Callao, Peru, and whether these factors are associated with the dental tissue structure’s damage. We hypothesize that there is a relationship between each of these factors and the caries experience among young children.
MATERIALS AND METHODS
The study followed ethical guidelines, including the 1964 Declaration of Helsinki and its updates. It was approved by the Graduate Studies Committee at San Fernando - Faculty of Medicine, Universidad Nacional Mayor de San Marcos (No. 018-UPG-FM-02018) and authorized by both the Regional Directorate of Education of Callao (DREC, Peru) and the school administration. Parents or legal guardians of eligible children provided written informed consent before participation. Data collection was anonymous, and parents completed questionnaires about their household and socio-demographic details. Our study follows STROBE reporting guidelines (see Supplementary Material).
Measurement of Variables
Household dynamics: We used 4 indicators including house ownership, parental living arrangements, family structure, and family size. House ownership was defined according to whether the family owns or rents the home in which the child resides. Parental living arrangements were dichotomized as whether the caregiver reports as a single parent (mother, or father), or whether the child lives with both of their parents. The variable for family structure distinguishes between nuclear families and extended families. A nuclear family consists of at least one parent and their children living together as a single household unit. In contrast, an extended family includes not only the nuclear family members but also other relatives such as grandparents, aunts, uncles, and cousins living in the same household and maintaining close daily interactions. Considering the latest census conducted in Peru, showing that the average family size in Lima is approximately of 3.5 members, we defined the variable family size as ‘small’ for households with up to 3 members, and as ‘large’ for those with 4 or more members.
Caries experience: This procedure was performed by a registered dentist, using portable equipment, dental explorers, biosafety measures, with support from a dental assistant as a note-taker, in a suitable room provided by the school, and it took approximately 10 minutes per child. We defined caries experience as the presence of at least one caries lesion (cavitated or non-cavitated), or filled surfaces, or missing teeth due to dental caries. Then, we dichotomized this variable into ‘high’ and ‘low’ using the 75^th^ percentile as a cut-off point, given the high prevalence (>10%). Specifically, we categorized children with a dmft score above the 75^th^ percentile as having high caries experience, and those with a dmft score below or equal to the 75^th^ percentile as low caries experience. For our sub-group analysis, dental lesions manifested as distinct, chalky white enamel, or with no clinically visible lesions, such as white spot lesions, were defined as non-cavitated. In contrast, cavitated lesions corresponded to those with evident loss of enamel structure 19. Our criteria did not differentiate between cavitated enamel and dentinal lesions.
Covariates: These included demographic factors such as child’s age, sex, and race/ethnicity. Parent’s socio-economic characteristics included their level of education, and employment status. Health behaviour factors included assisted toothbrushing, and frequency of sugar intake which was defined as high when 6 or more teaspoons of added sugar consumed daily, following the recommendation by the American Academy of Pediatrics (AAP) stating that children aged 2 years and older should consume less than 25 grams (approximately 6 teaspoons) of added sugar per day 20. Other covariates included factors related to access to dental services. These factors encompass the type of dental insurance, which is dichotomized as either public or private, and whether the child has ever visited a dentist for any reason. (Figure 1)
Figure 1. The directed acyclic graph (DAG) shows the potential association between several household dynamic indicators, such as house ownership, parental living arrangements, family structure, and family size, as independent variables, and caries experience as outcome of interest. Multiple covariates such as demographic, socio-economic, health behaviours, and factors of access to dental services may confound these associations.
Statistical analysis
We employed descriptive statistics reporting in absolute numbers and percentages for all variables. Next, multivariable block-wise regression models were constructed to estimate prevalence ratios (PR) with 95% confidence intervals (CI) of the association between household dynamics indicators and ECC experience, controlling for the aforementioned covariates. For the sub-group analysis, we summed the total number of decayed teeth, and stratified them by cavitated, and non-cavitated lesions as outcomes of interest, and adjusting for all covariates. All analyses were conducted using Stata v18.0 statistical software 21.
RESULTS
Characteristics of the study population
The sample comprised 210 children, each corresponding to one household, almost equally distributed by their age, with most being 3 years old (35.7%), followed by those aged 5 and 4 years. Most of the children were female (57.1%) and identified as mixed (78.6%). Predominantly, they were raised by single parents (77.1%), shared the household with at least 4 members (58.1%), and lived in rented accommodations (81.9%). Most of the households were defined as extended families (69.1%), including grandparents, aunts, uncles, and other relatives. Notably, 31.4% of the parents reported having incomplete high school education, and most (90.5%) were currently working. About 73.1% of the study sample was diagnosed with a decayed, missing, or filled tooth due to caries. Among those with decayed lesions, most had cavitated lesions (59.2%). While most of the parents reported not assisting their children during toothbrushing (89%) and never taking their child to the dentist (87.6%), 172 out of the 210 examined children fell into the category of low ECC caries experience (81.9%) compared to those with high ECC caries experience (18%). (Table 1).
Table 1. Descriptive statistics of characteristics of study participants (n = 210) stratified, Callao, Peru, 2017.Variables
All n (%) 210 (100)Age3y 75 (35.7)4y 67 (31.9)5y 68 (32.4)SexMales 90 (42.9)Females 120 (57.1)Race / EthnicityWhite 35 (16.7)Mixed 165 (78.6)Black 10 (4.7)DMFT indexDecayed Cavitated64 (30.4)Non-cavitated44 (20.9)Missing 36 (17.1)Filled 10 (4.7)No caries 56 (26.6)Early childhood caries experienceHigh (> 75th percentile) 38 (18)Low (≤ 75th percentile) 172 (81.9)Household dynamicsHouse ownershipOwn38 (18.1)Rented172 (81.9)Parental living arrangementsSingle parents (single mother, or single father)162 (77.1)Two-parent household48 (22.9)Family structureNuclear family65 (30.9)Extended family145 (69.1)Family sizeSmall (up to 3 members)88 (41.9)Large (4 or more members)122 (58.1)Health behavioursToothbrushingAssisted23 (11)Not assisted187 (89)Sugar intakeaHigh91 (43.3)Low119 (56.7)Parents’ socio-economic characteristicsEducation levelIncomplete high school66 (31.4)Complete high school or post-secondary education144 (68.6)Employment statusActive190 (90.5)Inactive20 (9.5)Access to dental servicesType of health insurancePublic (including army forces-funded)b190 (90.4)Private20 (9.6)Ever visited the dentistYes26 (12.4)No184 (87.6)aHigh sugar intake: ≥ 6 teaspoons of sugar daily; ^b^Government-funded including Essalud and the National Health Insurance (SIS by its acrnomym in Spanish)
Household dynamics indicators associate with high ECC experience
Each individual-household level dynamics indicator was significantly associated with young children’s caries experience. Parental living arrangement was the strongest indicator associated with a high ECC experience, followed by families in which the child, in addition to living with at least one parent, also lived with other relatives such as aunts, uncles, grandparents, cousins, etc. For example, the prevalence of having high ECC experience was almost twice as high in those children living with only one of their parents (PR 1.75, 95% CI 1.61, 1.91), after adjusting for other covariates. Specifically, this association was mostly explained by socio-economic factors such as the caregiver’s education level and employment status, contributing to 52% of the association. Other indicators, such as living in a rented house (PR 1.78, 95% CI 1.61, 1.87), living with other family members (PR 1.93, 95% CI 1.80, 2.12), and sharing the household with at least 4 other members (PR 1.39, 95% CI 1.26, 1.50) were significantly associated with high ECC experience. (Table 2).
Table 2. The association between household level dynamics indicators and high early childhood caries (ECC) experience, Callao, Peru, 2017. PR0 (95% CI)PR1 (95% CI)PR2 (95% CI)PR3 (95% CI)PR4 (95% CI)House Ownership (Rented)1.78* (1.61, 1.87 )1.75* (1.62, 1.89)1.63* (1.49, 1.79)1.32* (1.21, 1.47)1.29* (1.17, 1.41)Parental Living Arrangements (Single Parents)2.79* (2.59, 2.93)2.71* (2.54, 2.88)2.19* (2, 2.27)1.89* (1.71, 1.96)1.75* (1.61, 1.91)Family Structure (Extended Family)1.93* (1.80, 2.12)1.90* (1.79, 2.07)1.77* (1.61, 1.85)1.32* (1.23, 1.41)1.19* (1.08, 1.29)Family Size (Large)1.39* (1.26, 1.50)1.40* (1.26, 1.49)1.30* (1.22, 1.41)1.15* (1.07, 1.22)1.05 (0.94, 1.14)*p values ≤0.05, PR: prevalence ratio, CI: confidence intervalModel 0: Crude estimates (unadjusted)Model 1: Adjusting for age, sex, race/ethnicityModel 2: In addition, adjusted for parents’ education level, and employment statusModel 3: In addition, adjusted for assisted toothbrushing, and sugar intakeModel 4: In addition, adjusted for type of dental insurance, and ever visited the dentist
Sub-group analysis stratified by cavitated and non-cavitated dental lesions
Sub-group analysis revealed that several household dynamics indicators such as parental living arrangements, family structure, and family size were significantly associated with dental caries progression. The fully adjusted estimates controlling for demographic, socio-economic, health behaviours, and factors of access to dental services, suggest that the prevalence of having non-cavitated dental caries, such as white spot lesions, was higher among those children living in an extended family structure or sharing the household with at least 4 other members (PR 2.10, 95% CI 1.93, 2.21, and PR 1.88, 95% CI 1.70, 2, respectively), compared to their counterparts. Conversely, children living in single-parent families had a 2.4 times higher prevalence of having cavitated dental lesions compared to those with non-cavitated ones (PR 2.41, 95% CI 2.29, 2.62). No differences were noted when the associations were with house ownership. (Figure 2).
Figure 2. Forest plot graph shows the extent of the associations between each of the household dynamic indicators and cavitated (blue lines) and non-cavitated dental lesions (red lines), reported in prevalence ratios (PR) using 95% confidence intervals (CI). In our study sample, we found significant associations for each of the household dynamic indicators, except for house ownership, indicating that living in rental accommodations is not associated with the prevalence of either cavitated or non-cavitated dental lesions.
DISCUSSION
By cross-sectionally analyzing data from 210 children representing their households, we found that house ownership, parental living arrangements, family structure, and family size were significantly associated with a higher prevalence of ECC experience. Estimates from further analysis revealed that the prevalence of cavitated dental lesions was higher among young children from single-parent families, living with more members beyond their nuclear family, and sharing the household with at least four members. Children from larger families tended to have a higher prevalence of caries experience, in part due to resource dilution, where the attention and resources available per child decrease as the number of children increases. The rationale behind the association between the number of family members and caries experience may be explained through several mechanisms. Larger households may face greater financial constraints, leading to limited access to dental services and oral hygiene products. Additionally, in larger families, parents might have less time to dedicate to each child's oral hygiene, resulting in inadequate toothbrushing and oral hygiene routines 22. Moreover, siblings may share eating habits and sugary snacks, contributing to a higher risk of dental caries 23^,^24. Furthermore, a study conducted in families with 3- and 4-year-old children found that parents' marital status, including single-parent households, correlates with increased caries incidence, likely due to reduced supervision and inconsistent oral hygiene practices 9. Our estimates indicate that children raised by single parents showed a higher prevalence of caries experience compared to those raised by both parents. Single-parent households, due to economic struggles, increased stress, and limited time for childcare, may face challenges in maintaining regular dental visits and consistent oral hygiene routines for their children, potentially impacting overall health behaviours 23^,^25. Estimates from our sub-group analysis on the extent of dental tissue damage may be partly explained by the notion that these households may have fewer resources for preventive measures, such as regular dental visits. Consequently, the lack of timely intervention and ongoing dental care can lead to the progression of non-cavitated lesions, such as white spot lesions, into cavitated lesions, indicating more advanced tissue destruction 26^,^27.
Our findings strengthen our hypothesis that children living with their nuclear families may be generally less likely to develop dental caries compared to those sharing households with extended relatives. This difference may stem from more consistent caregiving routines in nuclear families, where parents can closely monitor and enforce oral hygiene practices. Extended family members might introduce varied dietary habits and potentially less rigorous oral hygiene standards, increasing caries risk among children 28.
Our sub-group analysis indicates that children living with extended family and in households with at least four members have a higher prevalence of early dental caries, such as non-cavitated lesions. This may be due to shared resources and differences in dietary and hygiene practices. Extended families often expose children to more sugary foods and beverages, while larger families might experience resource dilution, reducing attention and financial support for each child's dental care 6^,^29. However, we recognize that other variables related to breastfeeding, oral health habits during pregnancy, and use and frequency of bottle-feeding could potentially influence ECC experience 30^,^31.
One of the strengths of this study was the use of four comprehensive indicators of household dynamics (house ownership, parental living arrangements, family structure, and family size), providing a thorough understanding of the family environment. Second, the use of reliable and valid instruments to measure both family dynamics factors and caries experience, including the validation of the questionnaire using the Cronbach alpha test, adds to the study's robustness. Third, the use of clinical examinations for ECC provides an accurate assessment of children’s oral health. The clinical assessment conducted by a registered dentist ensures reliability and accuracy in diagnosing caries. Finally, the identification of multiple covariates acting as potential confounders and controlling them by the use of multivariable block-wise regression models for statistical analysis provides more precise estimates of the associations between household dynamics and ECC experience.
We acknowledge several limitations. First, the cross-sectional design limits the ability to draw causal inferences, as it captures data at a single point in time without considering changes over time. Second, the sample size, while sufficient for detecting associations, may not be large enough to generalize the findings to broader communities in Peru or other similar settings. Third, the reliance on questionnaires for data collection may introduce the risk of reporting bias, as responses may be influenced by social desirability or recall bias. Fourth, the clinical assessment, although thorough, did not differentiate cavitated enamel lesions from those involving dentin, potentially limiting the granularity of the caries experience data. However, while the dmft index does not allow us to assess the severity of the dental caries lesion, our clinical assessment allowed us to record the type of lesion by differentiating between cavitated and non-cavitated lesions, indicating the degree of progression of dental caries, particularly relevant in primary dentition. Fifth, our methods of dichotomizing certain variables, such as family size and caries experience, may oversimplify the complexity of these factors and reduce the variability in the data. Furthermore, the potential for unmeasured confounding variables, despite the inclusion of numerous covariates, remains a concern, as other factors influencing caries experience may not have been accounted for. Finally, the study's findings, while aligning with previous research, may still be subject to contextual biases specific to the studied population and setting, necessitating caution when generalizing to broader populations.
Our study has several policy implications, including the development of targeted interventions that address the specific needs of high-risk groups, such as single-parent households and larger families, by providing additional resources and support to mitigate the economic and social challenges these families face. Particularly in Peru, enhancing access to dental services and promoting educational campaigns by integrating oral health education into broader family support programs could be beneficial. Future research should focus on longitudinal studies to establish causal relationships and better understand the long-term effects of household dynamics on children’s oral health. Additionally, exploring the impact of other variables, such as breastfeeding practices, use of bottle-feeding, and maternal oral health habits during pregnancy, could provide a more comprehensive understanding of the factors influencing ECC. Ultimately, expanding the study to include diverse populations and settings will also help to generalize the findings and inform more effective public health strategies globally.
CONCLUSION
Individual household-level dynamics factors, including house ownership, parental living arrangements, family structure, and family size, are associated with the early onset of dental caries among young children in Peru. While parental education level and employment status explain most of these associations, further analysis is required to fully understand the underlying mechanisms and other contributing factors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO The Global Status Report on Oral Health 2022 [Internet]2022 https://www.who.int/team/noncommunicable-diseases/global-status-report-on-oral-health-2022
- 2IAPD Early Childhood Caries: IAPD Bangkok Declaration Int J Paediatr Dent 20192938438610.1111/ipd.1249031099129 · doi ↗ · pubmed ↗
- 3American Academy of Pediatric Dentistry.American Academy of Pediatrics.American Academy of Pediatric Dentistry Council on Clinical Affairs Policy on early childhood caries (ECC) classifications, consequences, and preventive strategies Pediatr Dent 200527313316541878 · pubmed ↗
- 4Rebelo MAB Rebelo Vieira JM Pereira JV Quadros LN Vettore MV Does oral health influence school performance and school attendance? A systematic review and meta-analysis Int J Paediatr Dent 20192913814810.1111/ipd.1244130367538 · doi ↗ · pubmed ↗
- 5CDC, MINSA Perú Reporte Estudio 2012-2014 - Centro Nacional de Epidemiología, Prevención y Control de Enfermedades 2014 https://www.dge.gob.pe/portalnuevo/
- 6Harris R Nicoll AD Adair PM Pine CM Risk factors for dental caries in young children a systematic review of the literature Community Dent Health 200421718515072476 · pubmed ↗
- 7Meyer F Enax J Early Childhood Caries: Epidemiology, Aetiology, and Prevention Int J Dent 201820181415873141587310.1155/2018/141587329951094 PMC 5987323 · doi ↗ · pubmed ↗
- 8Kirthiga M Murugan M Saikia A Kirubakaran R Risk Factors for Early Childhood Caries A Systematic Review and Meta-Analysis of Case Control and Cohort Studies Pediatr Dent 2019419511230992106 PMC 7100045 · pubmed ↗