Enamel matrix derivative and root coverage: A literature review
Edgar Daniel Vargas Quiroga, Brenda Carolina Pattigno Forero, Gloria Estefanía Amaya Chica, Lesbia Rosa Tirado Amador, Marilia Bianchini Lemos Reis

TL;DR
This paper reviews how enamel matrix derivative (EMD) improves periodontal treatments and root coverage surgeries, based on recent clinical studies.
Contribution
A systematic review of recent randomized clinical trials on EMD's effectiveness in periodontal regeneration and root coverage.
Findings
EMD significantly contributes to periodontal regeneration and root coverage outcomes.
Results across studies show variability in clinical outcomes like root coverage and clinical attachment gain.
More randomized controlled trials are needed to confirm EMD's efficacy in diverse clinical settings.
Abstract
: The use of enamel matrix derivative proteins, also known as Emdogain®, has revolutionized clinical practice in dentistry since the 90s. This biomaterial has demonstrated to promote periodontal tissues regeneration lost due to periodontal disease which persists as a public health problem, emerging as an effective alternative in treatments such as non-surgical periodontal therapy, treatment of furcation lesions, intraosseous defects, and more recently, its use has become especially popular in root coverage surgeries. : Evaluate studies in reference to the use of enamel-derived matrix proteins in periodontal treatments, to offer a comprehensive and up-to-date vision of its impact and effectiveness. : Systematic review was conducted about randomized clinical trials (RCTs) published between 2019 and 2024, using databases PubMed and Scopus, considering Clinical measurements performed in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
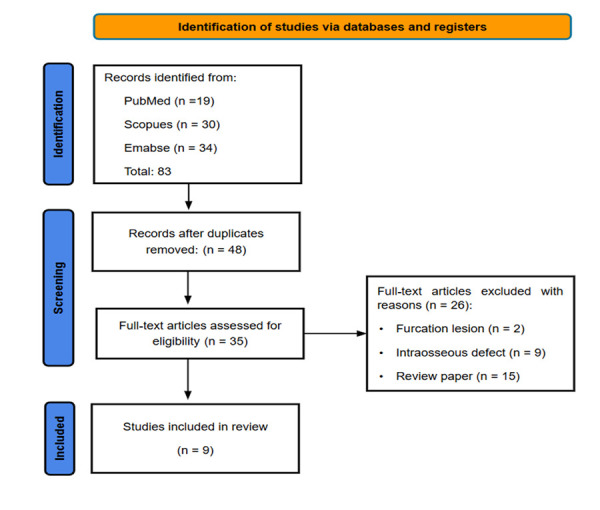 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeriodontal Regeneration and Treatments · Dental Implant Techniques and Outcomes · Electrospun Nanofibers in Biomedical Applications
INTRODUCTION
One of the current concerns among patients regarding aesthetics and dental sensitivity is gingival recession, which is an apical displacement of the gingival margin relative to the cemento-enamel junction (CEJ), exposing the root surface to the oral environment 1^,^2. Its etiology includes traumatic factors such as aggressive tooth brushing, excessive occlusal forces, and trauma, in combination with the patient's anatomical and biological predisposing factors, such as a thin gingival phenotype, dental malpositions, thin alveolar bone, and dental malformations 3^,^4. Periodontal mucogingival surgery aims to restore lost anatomy through surgical techniques designed to reposition the gingival margin either coronally or at the level of the cemento-enamel junction (CEJ) 5. The use of subepithelial connective tissue grafts (SCTG) has been shown to be effective in achieving increases in tissue volume and quality; however, it often results in the formation of a long junctional epithelium 6^,^7.
In 1997, Lars Hammarström introduced enamel matrix derivatives (EMD), which are porcine-derived proteins, with amelogenins as the main component 8. This biomaterial, commercially known as Emdogain®, has become a valuable tool in procedures such as non-surgical periodontal therapy, furcation defect treatment, and intrabony defect regeneration. Its use has gained popularity in root coverage surgeries 9^-^11. These proteins mimic the biological processes that occur during tooth development, promoting the formation of new acellular extrinsic fiber cementum, periodontal ligament, and alveolar bone 12. EMD stimulates cell proliferation and differentiation, particularly of fibroblasts and cementoblasts, which are responsible for extracellular matrix release. Additionally, it contributes to an increase in vascular endothelial growth factor (VEGF), enhancing tissue oxygenation and inducing angiogenesis. Moreover, it promotes transforming growth factor-beta (TGF-β), facilitating tissue repair and supporting the expression of gingival fibroblasts and periodontal ligament cells 12^,^13. The regenerative effect of EMD on bone is limited 14. While it has the potential to induce bone formation, it appears to be insufficient on its own and should be supplemented with a bone graft for optimal results 14^,^15.
Its association with periodontal root coverage surgery has shown improvements in connective tissue attachment, primarily because it promotes the formation of cementum and periodontal ligament. However, its effect on bone formation is limited. Nevertheless, it enhances the insertion of connective tissue fibers into the root surface 15. The objective of this narrative review is to thoroughly analyze contemporary studies from the last five years on randomized clinical trials investigating the use of enamel matrix derivative (EMD) in root coverage procedures, providing a comprehensive and updated perspective on its impact and efficacy.
MATERIAL AND METHODS
The search and analysis of information followed a systematic approach to identify, select, and analyze relevant studies published in the last five years.
Search Strategy
A search was conducted in two databases: PubMed and Scopus, with the aim of identifying research published between 2019 and 2024. The search method used a combination of keywords and Boolean operators to ensure a comprehensive selection of articles:
PubMed:
(("enamel matrix derivative"[All Fields] OR "EMD"[All Fields]) AND ("root coverage"[All Fields] OR "gingival recession"[All Fields]) AND ("surgery"[All Fields] OR "surgical procedure"[All Fields]) AND ("randomized controlled trial"[All Fields] OR "RCT"[All Fields])) AND (y_5[Filter])
Scopus:
TITLE-ABS-KEY ((“enamel matrix derivative" OR emd ) AND ( "root coverage" OR "gingival recession" ) AND (“surgery" OR "surgical procedure" ) AND ( "randomized controlled trial" OR rct ) ) AND PUBYEAR > 2018 AND PUBYEAR < 2025
Embase:
#1 ('enamel matrix derivative'/exp OR 'enamel matrix derivative' OR 'emd'/exp OR 'emd') AND ('root coverage'/exp OR 'root coverage' OR 'gingival recession'/exp OR 'gingival recession') AND ('surgery'/exp OR 'surgery' OR 'surgical procedure'/exp OR 'surgical procedure') AND ('randomized controlled trial'/exp OR 'randomized controlled trial' OR 'rct')
#2 (2019:py OR 2020:py OR 2021:py OR 2022:py OR 2023:py OR 2024:py)
1# AND 2#
The search was limited to randomized clinical trials (RCTs) with a follow-up period of more than 6 months, published in English within the last five years.
Inclusion and Exclusion Criteria
The following were excluded:
-
- Articles that were not RCTs (e.g., case reports, observational studies, systematic reviews, or scoping reviews).
-
- Articles that did not focus on root coverage surgery or EMD (e.g., surgeries for intraosseous defects).
-
- Articles not published in English.
-
- Articles published outside the specified five-year period.
Study Selection Process
The study selection process was carried out in three stages:
-
- Screening: Titles and abstracts of all retrieved studies were reviewed to exclude irrelevant articles.
-
- Review: The remaining articles were evaluated in full to determine their eligibility based on the inclusion and exclusion criteria.
-
- Selection: Studies that met all the criteria were included in the review. Additionally, the Jadad scale was used to assess the methodological quality of the clinical trials.
The Rayyan tool was used to detect and eliminate duplicate articles. Two independent reviewers, B.C.P.F. and E.D.V.Q., conducted the selection process. Disagreements between reviewers were resolved by a third reviewer, G.E.A.C., who determined whether the article would be included or excluded. The search was limited to studies published between 2019 and 2024.
Data Extraction
The following data were extracted from the selected studies: Author/Year, Country, Sample Size, Surgical Technique, Emdogain Group, Control Group, Outcomes (Root Coverage Percentage and Clinical Attachment Gain), Key Findings, and Conclusions. The Jadad Scale 16^,^17 was used to evaluate the methodology and assign a score to each selected clinical trial. The details of the selection process are presented in Table 1. The data were organized in an Excel table to facilitate collection, organization, and analysis of the information.
Table 1. Criteria used to assess the methodological quality of the included studiesCriterionDescriptionAuthorNameYearYear of publication of the study.Impact FactorWeb of Science (WoS) Journal InfoQuartile (Q1-Q4)Journal ranking within the Web of Science (WoS) Journal Info, ranging from Q1 (highest) to Q4 (lowest).RandomizationIndicates whether the study was randomized (Yes/No).Randomization MethodAssesses whether the randomization was adequate, inadequate, or not described.Double-BlindIndicates whether the study used the double-blind technique (Yes/No).Blinding MethodAssesses whether blinding was adequate, inadequate, or not described.Reported Dropouts/WithdrawalsIndicates whether the study reported participant losses and withdrawals during follow-up (Yes/No).Jadad Score (0-5)Jadad score for assessing the methodological quality of randomized clinical trials, considering randomization, blinding, and reporting of losses and exclusions.
RESULTS
A total of 83 studies were identified in the PubMed, Scopus, and Embase databases. After removing duplicates and applying the selection criteria filters, 9 studies were included in this review Figure 1 and Table 2.
Figure 1. Flow-chart of the screening of the relevant publications
Table 2. Selected articles and methodological quality assessment based on the Jadad scaleArticleYearImpact FactorQuartile (Q1-Q4)Randomized? (Yes/No)Randomization Method (Adequate/Inadequate/Not described)Double-Blind? (Yes/No)Blinding Method (Adequate/ Inadequate/Not described)Reported Dropouts/ Withdrawals? (Yes/No)Escore Jadad (0-5)Górski et al. (^18^)20203.1Q1YesAdequateYesAdequateYes5França-Grohmann et al. (^19^)20193.1Q1YesAdequateYesAdequateYes5Mercado et al. (^20^)20194.2Q1YesAdequateYesAdequateYes5Stähli et al. (^21^)20203.1Q1YesNot describedNoAdequateYes3Zuhr et al. (^22^)20205.8Q1YesNot describedNoAdequateYes3Dias et al. (^23^)20223.1Q1YesNot describedNoAdequateYes3Stähli et al. (^24^)20233.1Q1YesAdequateNoAdequateYes4Rieder et al. (^25^)20243.1Q2YesAdequateNoNot describedYes3Aydinyurt et al. (^26^)20191.5Q3YesInadequateYesAdequateYes3
Table 3. Summary of the included articles. Abbreviation: RCT- randomised controlled trial. MCAT - Modified Coronally Advanced Tunnel. SCPF - Semilunar Coronally Positioned Flap. CAF - Coronally Advanced Flap. TUN - Tunnel Technique. SCTG - Subepithelial Connective Tissue Graft. CTG - Connective Tissue Graft. XDM - Xenogeneic Dermal Matrix. CRC - Complete root coverage.Author/yearStudy DesignSample Size (patients)Gingival recessionSurgical TechniqueEmdogain GroupGroup ControlKey FindingsGórski et al. 2020 (^18^)RCT20RT 1 and RT 2 CairoMCATMCAT + SCTG + EMDMCAT + STCGNo significant difference in root coverage between the two groups (87.4% for test vs. 90.9% for control). Complete root coverage (CRC) was similar in both groups (86.7% for test vs. 85.3% for control).França-Grohmann et al. 2019 (^19^)RCT30Miller Class I (RT 1 Cairo)SCPFSCPF + EMDSCPF aloneNo significant difference in root coverage between the two groups (90.86% for test vs. 79.76% for control). CRC was higher in the test group (66.67% vs. 33.33% in control).Mercado et al. 2019 (^20^)RCT41Multiple Miller Class III and IV (RT 2 and 3 Cairo)CAFCTG + EMDCTG aloneIn the test group, recession depth decreased from 5.71 ± 0.58 mm to 1.57 ± 0.85 mm at 36 months, while in the control group, it decreased from 5.94 ± 0.46 mm to 2.51 ± 0.62 mm. The difference was statistically significant ( P<0.001). In the test group, KT increased from 1.51 ± 0.26 mm to 4.18 ± 0.34 mm, while in the control group, it increased from 1.65 ± 0.21 mm to 2.90 ± 0.20 mm. The difference was statistically significant (P<0.001).Stähli et al. 2020 (^21^)RCT40Miller Class I, II or III single or multiple (RT 1 and 2 Cairo)MCATMCAT + EMD + SCTGMCAT + STCGAt 6 months, recession depth was reduced from 4.0 ± 1.2 mm to 0.9 ± 1.3 mm in the test group and from 4.5 ± 2.0 mm to 1.0 ± 1.0 mm in the control group. Mean root coverage was 78 ± 26% in the test group and 77 ± 18% in the control group, with no significant differences between the groups.Zuhr et al. 2020 (^22^)RCT23Miller Class I or II, RT 1 CairoTunnel and CAFTunnel + CTGCAF + EMDAt 24 months, digitally evaluated CRC was present in 60.0% of the TUN + CTG group and 0.0% of the CAF + EMD group. RC amounted to 94.0% in the TUN + CTG group and 57.3% in the CAF + EMD group. REC reduction (RECred) was significantly higher for TUN + CTG (1.81 ± 0.56 mm) than for CAF + EMD (0.90 ± 0.45 mm).Dias et al. 2022 (^23^)RCT16RT 1 CairoCAFCAF + SCTG + EMDCAF + SCTGThe test group showed significantly higher root coverage (86%) compared to the control group (66%) after 6 months. Recession height (RH) and recession width (RW) were significantly reduced in both groups, with better results in the test group. No significant differences were observed in KTH and GT between the groups.Stähli et al. 2023 (^24^)RCT24RT 1 and RT 2 CairoMCATMCAT + CTG + EMDMCAT + CTGAt 5 years, 57.14% of the test group and 60% of the control group showed complete root coverage. Mean root coverage (MRC) was 73.87% in the test group and 75.04% in the control group. Keratinised tissue (KT) increased significantly in both groups, from 1.14 mm to 3.07 mm in the test group and from 1.24 mm to 3.02 mm in the control group. No statistically significant differences were found between the groups in terms of CRC, MRC, KT, or RES.Rieder et al. 2024 (^25^)RCT15Miller class I or II, RT 1 CairoCAFCAF + XDM + EMDCAF + XDMNo statistically significant difference in root coverage between the control group (69 ± 28%) and the test group (36 ± 32%) (p = 0.094). Both groups showed significant improvement in KTW over time (p < 0.001), with no significant difference between groups (p = 0.690). The control group showed superior results in keratinized tissue thickness (KTT) compared to the test group (p = 0.044).Aydinyurt et al. 2019 (^26^)RCT19Miller class I or II, RT 1 CairoCAFCAF + SCTG + EmdogainCAF + SCTGBoth techniques showed a significant reduction in gingival recession. The EMD group showed better results in soft tissue texture and mucogingival junction alignment (p < 0.05). The complete root coverage rate was 68% in the EMD group and 52% in the control group.
The analyzed studies compared different surgical techniques for the treatment of gingival recessions, focusing on the percentage of root coverage (RC), clinical attachment gain (CAL), increase in gingival thickness (KTW), long-term stability, and postoperative pain (VAS). Clinical measurements performed in the studies were included to allow comparison of results. The analysis of the articles also showed that the Coronally Advanced Flap (CAF) technique is the most commonly used (five studies), often associated with subepithelial connective tissue graft (SCTG), connective tissue graft (CTG), and xenogeneic dermal matrix (XDM). The main results were summarized in Table 3. A total of 228 patients were evaluated in the studies, and a total of 549 were part of the study. The use of Enamel Matrix Derivative (EMD) is associated with these techniques, and its combination with other techniques showed better results in terms of postoperative outcomes and aesthetic perception. The criteria by which these results were achieved include the evaluation of the percentage of root coverage, clinical attachment gain, increase in gingival thickness, long-term stability, and postoperative pain.
DISCUSSION
This literature review analyzed randomized clinical trials (RCTs) published in the last five years that investigated the use of enamel matrix derivative (EMD) in root coverage procedures for the treatment of gingival recessions. The results of the included studies show a variety of findings regarding the efficacy of EMD in root coverage, clinical attachment gain, reduction of sensitivity, and aesthetic perception.
EMD and root coverage
The use of EMD has been associated with positive outcomes in terms of root coverage, especially in more complex gingival recessions such as those classified as Cairo RT2 or Miller Class III and IV. Mercado et al. 20 evaluated the use of EMD in combination with Connective Tissue Graft (CTG) in Miller Class III and IV recessions (Cairo RT2 and RT3) over 36 months. The results showed a significant reduction in recession depth (from 5.71 mm to 1.57 mm in the EMD + CTG group) and stable root coverage over time 20. It also resulted in a significant increase in the width of keratinized tissue (from 1.51 mm to 4.18 mm), demonstrating that the use of EMD can improve not only root coverage but also the quality of gingival tissue 20. Stähli et al. (^24^) followed patients for 5 years after the treatment of Cairo RT1 and RT2 recessions with EMD + CTG 24. Complete root coverage (CRC) was achieved in 57.14% of cases in the EMD + CTG group, with an average root coverage (MRC) of 73.87% 24. The stability of results over 5 years reinforces the efficacy of EMD 24. However, no statistical difference was shown with the control group.
Stähli et al.21^)^ did not find significant differences between MCAT + SCTG + EMD and the control group (78% vs. 77% of RC), suggesting that EMD may not be decisive in all techniques 21. Górski et al. 18^)^ showed no significant differences in root coverage between MCAT + SCTG + EMD and the control group (87.4% vs. 90.9%), reinforcing that EMD may not be decisive in all techniques 18. Rieder et al. 25 also observed no advantages of CAF + XDM + EMD (test 36% vs. 69% in the control), indicating that factors such as the xenogenic matrix (XDM) may limit its efficacy 25. Aydinyurt et al.26 reported a higher rate of CRC in the EMD group (68% vs. 52%), highlighting its positive impact on Miller Class I/II or Cairo RT 1 recessions 26. Dias et al. 23 reinforced this finding, showing that CAF + SCTG + EMD achieved 86% complete root coverage, compared to 66% in the control group 23.
EMD and tissue thickness
The use of EMD has shown a positive impact on the thickness of the keratinized tissue (KT) and the quality of the gingival tissue. Mercado et al. 20 indicates that the group treated with EMD showed a significant increase in the width of the keratinized tissue (KT) from 1.51 mm to 4.18 mm after 36 months, a result significantly greater than in the control group 20. Similarly, Stähli et al. 24 reported an increase in the width of the keratinized tissue (KT) from 1.14 mm to 3.07 mm after 5 years in the group treated with EMD, demonstrating the long-term stability of the treatment 24. However, Zuhr et al. 22 observed that the group treated with TUN + CTG (without EMD) had a significantly greater gingival thickness (GT) (1.41 mm) compared to the group treated with CAF + EMD (0.78 mm), suggesting that CTG may be superior to EMD in terms of increasing gingival thickness 22.
Some studies have shown neutral or limited results. Stähli et al. 21 did not observe significant differences in the width of the keratinized tissue (KT) between the groups treated with and without EMD after six months 22. Rieder et al. also reported that the control group (without EMD) had superior results in the thickness of the keratinized tissue (KTT) compared to the group treated with EMD 25. Górski et al. 18 did not observe significant differences in gingival thickness (GT) or keratinized tissue width (KTW) between the groups with and without EMD, despite the aesthetic improvement 18.
EMD and inflammatory markers
Dias et al. 23 reported that VEGF levels were significantly higher in the test group after 14 days, suggesting increased angiogenesis and healing 23. IL-1β and IL-6 levels were significantly elevated in both groups after 7 days, with IL-1β remaining elevated in the test group after 14 days 23. Stähli et al. 21 did not observe significant differences in the levels of inflammatory markers (IL-1β, IL-8, IL-10, MMP-8, and TGF-β1) between the two groups at any time 21. Gerova-Vatsova et al. 27 observed that EMD helps to improve and accelerate the healing of soft tissues and the resolution of inflammation 27. Villa et al. 28 highlighted that TGF-α plays a crucial role in the proliferative phase of wound healing, angiogenic processes, and granulation tissue formation 28.
Aesthetic perception and patient satisfaction
Esthetic perception and patient satisfaction are critical aspects, and EMD stands out in these criteria. Górski et al. 18 reported less postoperative pain and better esthetic evaluation (RES) in the EMD group, highlighting the alignment of the mucogingival junction and tissue texture 18. França-Grohmann et al. observed greater patient satisfaction (evaluated by VAS) and better professional evaluation (QCE) in the EMD group, even without statistical differences in root coverage 19. Aydinyurt et al. 26 highlighted the improvement in tissue texture and mucogingival alignment in the EMD group, key factors for treatment acceptance 26. Mercado et al. and Stähli et al. reinforced that patient treated with EMD reported greater satisfaction, referring to an improvement in associated symptoms such as pain, supporting the idea that the use of EMD generates significant biological benefits and clinical outcomes 20^,^24.
LIMITATIONS
The heterogeneity of the included studies, particularly in surgical techniques and graft harvesting methods, may have affected result comparability. Methodological quality also varies, with some studies showing a risk of bias due to lack of blinding or inadequate randomization. The limited number of clinical trials and variability in follow-up periods make conclusions uncertain. However, Mercado et al. 20. and Zuhr et al. 22 provide long-term follow-up. Mercado’s study showed good stability in challenging Miller Class III and IV recessions (RT2/RT3 of Cairo), while Zuhr’s study, using Emdogain without grafting, showed inferior outcomes. Graft association has been shown to enhance stability and tissue gain over time 6. More long-term randomized clinical trials with standardized methods are needed to clarify the role of enamel matrix derivative in clinical outcomes.
CONCLUSIONS
The results related to root coverage vary depending on the surgical technique and the type of recession treated. In complex cases such as Cairo RT2 or RT3, it may offer benefits; however, in less complex recessions, the results seem to be more inconsistent. Its capacity to increase gingival thickness may vary depending on the surgical technique and the type of recession. In terms of aesthetics, it appears to be consistently associated with better aesthetic outcomes and greater patient satisfaction, regardless of statistical differences in clinical parameters.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cortellini P Bissada NF Mucogingival conditions in the natural dentition Narrative review, case definitions, and diagnostic considerations J Periodontol 2018891 S 204S 21310.1002/JPER.16-067129926948 · doi ↗ · pubmed ↗
- 2Mascardo KC Tomack J Chen CY Mancini L Kim DM Friedland B Barootchi S Tavelli L Risk indicators for gingival recession in the esthetic zone A cross-sectional clinical, tomographic, and ultrasonographic study J Periodontol 202495543244310.1002/JPER.23-035738196327 · doi ↗ · pubmed ↗
- 3Imber JC Kasaj A Treatment of Gingival Recession When and How?Int Dent J 202171317818710.1111/idj.1261734024328 PMC 9275303 · doi ↗ · pubmed ↗
- 4Souccar NM Oueis R Mussleman JP Jr Geurs NC Abou-Arraj RV The Impact of Orthodontic Retainers on Gingival Recession A Best-Evidence Review Compend Contin Educ Dent 2022433 E 1E 435377673 · pubmed ↗
- 5De Lauretis A ØvrebøØ Romandini M Lyngstadaas SP Rossi F Haugen HJ From Basic Science to Clinical Practice A Review of Current Periodontal/Mucogingival Regenerative Biomaterials Adv Sci (Weinh)20241117 e 230884810.1002/advs.20230884838380549 PMC 11077667 · doi ↗ · pubmed ↗
- 6Pini Prato GP Franceschi D Cortellini P Chambrone L Long-term evaluation (20 years) of the outcomes of subepithelial connective tissue graft plus coronally advanced flap in the treatment of maxillary single recession-type defects J Periodontol 201889111290129910.1002/JPER.17-061929873085 · doi ↗ · pubmed ↗
- 7Majzoub Z Landi L Grusovin MG Cordioli G Histology of connective tissue graft A case report J Periodontol 200172111607161510.1902/jop.2001.72.11.160711759874 · doi ↗ · pubmed ↗
- 8Hammarström L Enamel matrix, cementum development and regeneration J Clin Periodontol 1997249 Pt 265866810.1111/j.1600-051x.1997.tb 00247.x 9310870 · doi ↗ · pubmed ↗