A Multicenter Study in Northern Italy to Evaluate the Impact of a Sepsis Bundle in Obstetric Settings: The SOS Study
Marta Colaneri, Simona Biscarini, Lara Tiranini, Rebecca Pesare, Pietro Valsecchi, Elena Seminari, Arsenio Spinillo, Alessandra Bandera, Enrico Mario Ferrazzi, Andrea Gori, Laura Carenzi, Luigi Pusterla, Federico D’Amico, Alessandro Raimondi, Massimo Puoti, Elisa Vallicella

TL;DR
A study in Italy evaluated a sepsis management bundle for pregnant women and found it reduced neonatal ICU admissions but had no significant effect on maternal outcomes.
Contribution
The study introduces a regional sepsis management bundle tailored for obstetric patients and evaluates its real-world impact.
Findings
Neonatal ICU admissions decreased significantly after bundle implementation.
There was no significant change in maternal ICU admissions or hospital stay length.
Infectious disease specialist consultations increased postbundle.
Abstract
In 2018, Lombardy's Fight Against Sepsis in Obstetrics group developed a regional sepsis management bundle for obstetric patients. This study aimed to evaluate the impact of this bundle on maternal and neonatal clinical outcomes and on process measures. This multicenter, observational, retrospective study included data from pregnant and puerperal adult patients diagnosed with sepsis according to the Surviving Sepsis Campaign guidelines in 2 periods: May 2015 to May 2018 (prebundle) and July 2018 to January 2023 (postbundle). Eighty women were included: 24 (30.0%) in the prebundle period and 56 (70.0%) in the postbundle period. The primary source of infection was urinary (40.0%), with Escherichia coli being the most common pathogen isolated from blood cultures. Regarding clinical outcomes, no deaths occurred in pre- and postbundle periods. For mothers, there was no significant…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
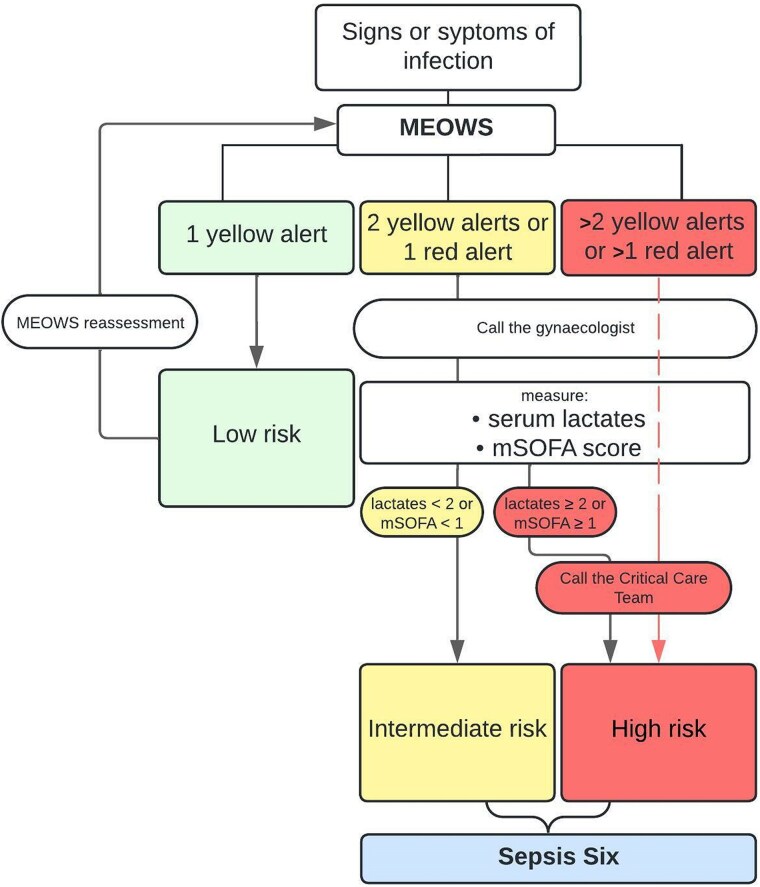 Figure 1
Figure 1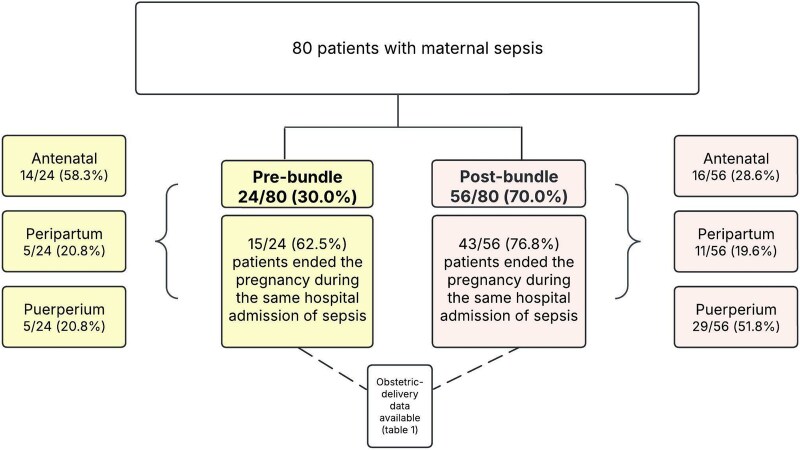 Figure 2
Figure 2| No. (%) or Median (IQR) | |||||
|---|---|---|---|---|---|
| No. | Overall (n = 80) | Prebundle (n = 24) | Postbundle (n = 56) |
| |
| Age, y | 80 | 31.0 (26.0–36.3) | 33.5 (25.8–37.3) | 31 (26.0–36.0) | .578 |
| Ethnicity | 79 | .301 | |||
| Caucasian | 53 (66.3) | 15 (62.5) | 38 (67.9) | ||
| Hispanic | 6 (7.5) | 1 (4.2) | 5 (8.9) | ||
| Indian | 3 (3.8) | 1 (4.2) | 2 (3.6) | ||
| Asiatic | 2 (2.5) | 2 (8.3) | 0 (0) | ||
| African | 6 (7.5) | 1 (4.2) | 5 (8.9) | ||
| Arabic | 7 (8.8) | 2 (8.3) | 5 (8.9) | ||
| Other | 2 (2.5) | 0 (0) | 2 (3.6) | ||
| History | 80 | ||||
| Penicillin allergy | 7 (8.8) | 3 (13) | 4 (7.1) | .450 | |
| Cardiovascular disease | 3 (3.8) | 1 (4.2) | 2 (3.6) | >.981 | |
| Thyroid abnormalities | 13 (16.3) | 6 (25.0) | 7 (12.5) | .200 | |
| Hematologic malignancy | 4 (5.0) | 0 (0) | 4 (7.1) | .304 | |
| Respiratory disease | 2 (2.5) | 0 (0) | 2 (3.6) | >.900 | |
| Kidney disease | 1 (1.3) | 0 (0) | 1 (1.8) | >.900 | |
| Rheumatic disease | 2 (2.5) | 1 (4.2) | 1 (1.8) | .577 | |
| Previous septic event | 3 (3.8) | 2 (8.3) | 1 (1.8) | .232 | |
| Uterine fibroids | 5 (6.6) | 1 (4.2) | 4 (7.7) | >.900 | |
| Previous abdominal surgery | 9 (11.3) | 2 (8.3) | 7 (12.5) | .734 | |
| Obstetric history | |||||
| No. of prior pregnancies | 80 | .400 | |||
| 0 | 42 (53.8) | 10 (41.7) | 32 (57.1) | ||
| ≥3 | 7 (8.7) | 3 (12.5) | 4 (7.1) | ||
| Previous cesarean section | 79 | 16 (20.0) | 4 (16.7) | 12 (21.4) | >.900 |
| Multiple pregnancy | 80 | 8 (10.0) | 1 (4.2) | 7 (12.5) | .401 |
| Pregnancy complication | |||||
| HELLP syndrome | 80 | 3 (3.8) | 1 (4.2) | 2 (3.6) | >.900 |
| Gestational diabetes | 80 | 5 (6.3) | 1 (4.2) | 4 (7.1) | >.900 |
| Gestational hypertension | 80 | 8 (10.0) | 1 (4.2) | 7 (12.5) | .458 |
| Cholestasis | 80 | 3 (3.8) | 0 (0) | 3 (5.4) | .587 |
| PPROM | 80 | 16 (20.0) | 5 (20.8) | 11 (19.6) | >.900 |
| Preterm labor | 79 | 9 (11.4) | 4 (16.7) | 5 (9.1) | .411 |
| Patients at high risk | 80 | 52 (65) | 15 (63) | 37 (66) | .759 |
| Obstetric-delivery data | 58 | 15 | 43 | ||
| Gestational age delivery, wk | 57 | 36.0 (25.0–39.0) | 26.0 (17.0–33.0) | 37.0 (27.0–39.8) | .006 |
| Induction of labor | 58 | 20 (34.5) | 4 (26.7) | 16 (37.2) | .500 |
| Cesarean section | 58 | 35 (60.3) | 10 (66.7) | 25 (58.1) | .577 |
| Antibiotic prophylaxis | 46 | 14 (30.4) | 6 (50.0) | 8 (23.5) | .140 |
| Delivery complications | |||||
| Postpartum hemorrhage | 55 | 15 (27.3) | 2 (14.3) | 13 (31.7) | .301 |
| Manual removal of retained placenta | 53 | 14 (26.4) | 4 (30.8) | 10 (25.0) | .678 |
| Disseminated intravascular coagulation | 55 | 2 (3.6) | 1 (7.1) | 1 (2.4) | .400 |
| No. (%) or Median (IQR) | |||||
|---|---|---|---|---|---|
| No. | Overall (n = 80) | Prebundle (n = 24) | Postbundle (n = 56) |
| |
| Time of sepsis identification | 80 | .021 | |||
| Antenatal: from conception to labor onset | 30 (37.5) | 14 (58.3) | 16 (28.6) | ||
| Peripartum: from labor onset to delivery of placenta | 16 (20.0) | 5 (20.8) | 11 (19.6) | ||
| Puerperium: from delivery of placenta to 42 d after | 34 (42.5) | 5 (20.8) | 29 (51.8) | ||
| Source of sepsis | |||||
| Genital tract | 80 | 12 (15.0) | 5 (20.8) | 7 (12.5) | .500 |
| Urinary tract | 80 | 32 (40.0) | 9 (37.5) | 23 (41.1) | .765 |
| Chorioamnionitis | 80 | 23 (28.8) | 8 (33.3) | 15 (26.8) | .588 |
| Pneumonia | 80 | 7 (8.8) | 3 (12.5) | 4 (7.1) | .357 |
| Appendicitis | 80 | 1 (1.3) | 0 (0) | 1 (1.8) | >.900 |
| Surgical site | 80 | 6 (7.5) | 1 (4.2) | 5 (8.9) | .701 |
| Skin soft tissue | 80 | 1 (1.3) | 0 (0) | 1 (1.8) | >.900 |
| Mastitis | 80 | 1 (1.3) | 0 (0) | 1 (1.8) | >.900 |
| Unknown | 80 | 8 (10.0) | 0 (0) | 8 (14.3) | .100 |
| MEOWS: color-coded score risk | 42 | .310 | |||
| High | 26 (61.9) | … | 26 (61.9) | ||
| Intermediate | 12 (28.6) | … | 12 (28.6) | ||
| Low | 4 (9.5) | … | 4 (9.5) | ||
| mSOFA score | 73 | .800 | |||
| <1 | 22 (30.1) | 7 (31.8) | 15 (29.4) | ||
| ≥1 | 51 (69.9) | 15 (68.2) | 36 (70.6) | ||
| Laboratory test results | |||||
| Lactates | 38 | 1.5 (0.8–2.7) | 0.9 (0.7–1.5) | 1.6 (0.8–2.7) | .199 |
| White blood cells count, × 103/μL | 79 | 13.4 (8.0–18.3) | 10.2 (3.5–15.4) | 14.9 (9.1–19.5) | .050 |
| C-reactive protein, mg/dL | 79 | 14.7 (7.8–21.9) | 11.8 (8.1–19.0) | 15.4 (7.8–23.3) | .186 |
| Diagnostic imaging performed | 80 | ||||
| Chest x-ray | 42 (52.5) | 14 (58.3) | 28 (50.0) | .469 | |
| Abdominal ultrasound | 47 (58.8) | 12 (50.0) | 35 (62.5) | .269 | |
| Transvaginal ultrasound | 42 (52.5) | 12 (50.0) | 30 (53.6) | .799 | |
| CT scan | 20 (25.0) | 7 (29.2) | 13 (23.2) | .622 | |
| No. (%) | |||||
|---|---|---|---|---|---|
| No. | Overall (n = 80) | Prebundle (n = 24) | Postbundle (n = 56) |
| |
| Polymicrobial | 52 | 4 (7.7) | 0 (0) | 4 (10.3) | .677 |
| Isolated pathogens | 56 | 56 | 13 | 43 | .689 |
|
| 27 (48.2) | 8 (61.5) | 19 (44.2) | ||
|
| 11 (19.6) | 2 (15.4) | 9 (20.9) | ||
| Anaerobic bacteria | 6 (10.7) | 1 (7.7) | 5 (11.6) | ||
|
| 6 (10.7) | 1 (7.7) | 5 (11.6) | ||
|
| 3 (5.4) | 0 (0) | 3 (6.9) | ||
|
| 3 (5.4) | 1 (7.7) | 2 (4.7) | ||
| Class of administered antibiotics | |||||
| Penicillins | 80 | 51 (63.8) | 12 (50.0) | 39 (69.6) | .094 |
| Cephalosporins | 78 | 28 (35.9) | 10 (41.7) | 18 (33.3) | .455 |
| Carbapenems | 77 | 21 (27.3) | 5 (20.8) | 16 (30.2) | .366 |
| Fluoroquinolones | 77 | 7 (9.1) | 2 (8.3) | 5 (9.4) | >.900 |
| Aminoglycosides | 79 | 24 (30.4) | 4 (16.7) | 20 (36.4) | .081 |
| Glycopeptides and lipoglycopeptides | 79 | 17 (21.5) | 5 (20.8) | 12 (21.8) | >.900 |
| Macrolides, lincosamides | 80 | 10 (12.5) | 6 (25.0) | 4 (7.1) | .058 |
| Others | 79 | 17 (21.5) | 9 (37.5) | 8 (14.5) | .022 |
| No. | Overall (n = 80) | Prebundle (n = 24) | Postbundle (n = 56) |
| |
|---|---|---|---|---|---|
| Length of stay, d | 80 | 13.0 (9.0–18.3) | 10.5 (8.0–17.0) | 14.0 (10.0–20.3) | .211 |
| Maternal death | 0 | 0 (0) | 0 (0) | 0 (0) | … |
| ICU admission | 80 | 22 (27.5) | 9 (37.5) | 13 (23.2) | .200 |
| ICU length of stay, d | 22 | 3.5 (2.3–6.8) | 3.0 (2.0–6.0) | 5.0 (3.0–7.0) | .300 |
| Miscarriage | 58 | 15 (25.9) | 7 (46.7) | 8 (18.6) | .045 |
| Stillbirth | 58 | 0 (0) | 0 (0) | 0 (0) | … |
| NICU admission | 39 | 16 (41.0) | 6 (85.7) | 10 (31.3) | .013 |
| Weight at birth, g | 38 | 2948.5 | 1100.0 | 3100.0 | .300 |
| Early neonatal death, within 7 d | 39 | 3 (7.7) | 1 (14.2) | 2 (6.3) | .522 |
| No. (%) or Median (IQR) | |||||
|---|---|---|---|---|---|
| No. | Overall (n = 80) | Prebundle (n = 24) | Postbundle (n = 56) |
| |
| Lactates performed | 80 | 38 (48) | 9 (38) | 29 (52) | .200 |
| Blood cultures performed | 80 | 74 (92.5) | 22 (91.7) | 52 (92.9) | .222 |
| Positive blood culture results | 74 | 52 (70.3) | 13 (59.0) | 39 (75.0) | .222 |
| Time elapsed between suspicion of sepsis and blood culture, h | 50 | 2.7 (0.7–23.3) | 11.0 (0.0–28.0) | 2.0 (0.8–21.3) | .800 |
| Antibiotic treatment before sepsis suspicion | 79 | 41 (51.9) | 11 (47.8) | 30 (53.6) | .566 |
| Antibiotic started before cultures | 76 | 50 (65.8) | 13 (59.0) | 37 (68.6) | .379 |
| Antibiotic appropriateness | 52 | 39 (75) | 9 (69) | 30 (77) | .700 |
| Length of antibiotic treatment, d | 78 | 10.0 (7.0–15.8) | 8.0 (7.0–14.0) | 11.0 (7.3–16.0) | .297 |
| Infectious disease specialist consultation | 80 | 54 (67.5) | 12 (50.0) | 42 (75.0) | .029 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSepsis Diagnosis and Treatment · Neonatal and Maternal Infections · Emergency and Acute Care Studies
Sepsis accounts for 11% of maternal deaths globally [1]; despite its significant impact, its early identification and management remain challenging for different reasons [2]. First, an international consensus definition of sepsis in pregnancy and puerperium was established by the World Health Organization only in 2017 [3]; second, pregnant women's physiologic and immunologic adaptations can alter their ability to effectively combat infection, obscure certain signs of sepsis, and delay its recognition [4]. In addition, sepsis guidelines have always been modeled on the basis of randomized controlled trials that did not include pregnant patients, affecting the utility of the Quick Sequential Organ Failure Assessment, National Early Warning Score, or Systemic Inflammatory Response Syndrome score in this unique population [5].
As a result, an obstetric-specific sepsis scoring system, the Modified Early Obstetric Warning Score (MEOWS), has been proposed and further validated [6, 7]. However, its efficacy to reduce maternal deaths seems limited [8], and this may depend on its potentially enhanced performance when coupled with a proper guidance on action enclosed in bundles.
Over the last 2 decades, the Surviving Sepsis Campaign highlighted the importance of generating standardized guidelines for management of sepsis and septic shock in the general population. The implementation of sepsis bundles aimed to direct physicians toward the early diagnosis and treatment of this condition, leading to an improvement in the quality of management for cases of sepsis [9].
The evidence surrounding the efficacy of sepsis bundles remains inconclusive, with conflicting data emerging from recent studies. While the Sepsis Six, a set of 6 practical interventions, is widely recognized for its potential to significantly improve survival rates when implemented within the first hour of sepsis recognition [10], recent multicenter randomized trials have shown that early goal-directed therapy may not offer benefits over usual care [11–13]. Importantly, there is a significant gap in the literature regarding the application and effectiveness of sepsis bundles in the pregnant and puerperal populations, where sepsis presents unique challenges [14].
In May 2018, the Fight Against Sepsis in Obstetrics working group of the Lombardy Region in Northern Italy developed a bundle following regional risk management indications, which was aimed at proposing definitions and procedures for the identification and management of sepsis in the obstetric setting [15]. The objective of this study was to assess the effects of the regional sepsis bundle implementation in 7 hospitals in Lombardy.
METHODS
Study Design and Setting
The SOS study is a multicenter, observational, and retrospective cohort study conducted in 7 referral hospitals in the Lombardy Region, Northern Italy (IRCCS Fondazione Policlinico San Matteo of Pavia, Azienda Socio-Sanitaria Territoriale of Cremona, Ospedale Sant’Anna of Como, IRCCS Ospedale Ca’ Granda of Milan, ASST Grande Ospedale Metropolitano Niguarda of Milan, Ospedale Carlo Poma of Mantova, Vittore Buzzi Children Hospital of Milan).
The leading coordinating center was IRCCS Policlinico San Matteo Foundation, Pavia. Every center housed intensive care unit (ICU), infectious diseases (ID), and gynecology/obstetrics beds. Moreover, all the centers had a specific obstetrical emergency department, as well as pediatric and neonatology specialists.
Inclusion Criteria
Data were collected of all the pregnant and puerperal adult patients who were diagnosed with sepsis according to the Surviving Sepsis Campaign guidelines [9] between May 2015 and May 2018 (prebundle period) and between July 2018 and January 2023 (postbundle period). The only exclusion criterion was age <18 years. The reason for the 2-month gap was to allow time for the bundle to circulate and be used in daily practice by the considered hospitals in Lombardy.
First, medical records were retrieved of all pregnant and puerperal patients discharged with a sepsis-related ICD-9 code—namely, regarding “sepsis,” “septic shock,” and “infection.” Second, clinical data were analyzed by ID specialists, and the patients were included if they had (1) organ dysfunction, determined by an increase ≥2 points in the Sequential Organ Failure Assessment (SOFA) score, and (2) infection, the diagnosis of which relied on clinical suspicion from signs and symptoms of infection, radiologic and microbiologic data, and response to therapy. The medical records were then anonymized and abstracted on standardized data collection forms in the web platform REDCap. Demographic and clinical data were retrospectively extracted from paper and electronic records from the 7 involved hospitals. Notably, the centers were eligible for the study if caring for at least 1500 deliveries per year.
Patient Consent
This research project was carried out in accordance with a research plan and per the current version of the Declaration of Helsinki. The sponsor (IRCCS Policlinico San Matteo Foundation, Pavia) ensured that approval from a competent ethics committee was sought for the study. Informed consent for pseudonymized data processing for future research purposes was provided by all patients at the time of hospital admission, as routine procedure. Specific written informed consent was waived because of the retrospective nature of the analysis. The SOS study was approved by the IRCCS Policlinico San Matteo Foundation Institutional Review Board (20210080285; 25 August 2021).
Bundle Description
The “Operational Guidance Document for Early Identification and Management of Sepsis in Obstetrics” was developed by the working group Fight Against Sepsis in Obstetrics of the Lombardy Region, Northern Italy, following regional indications of risk management. A version translated in English is provided in the supplementary materials. The aim of the bundle was to propose definitions and procedures for the identification and management of sepsis in the obstetric population.
Although this is a comprehensive bundle that addresses various aspects of sepsis management, such as hemodynamic support, fluid resuscitation, and vasopressor use, our primary focus was related to ID-centered aspects, such as recognition and management of maternal sepsis with appropriate microbiological testing and antibiotic therapy. We briefly discuss these key points in turn.
Recognition of Maternal Sepsis
The bundle clearly states that all pregnant women arriving at the maternity triage service or already hospitalized should be monitored with the MEOWS, a specific early warning tool (Supplementary Figure 1, supplementary materials). MEOWS entails the assessment of vital signs such as respiratory rate, blood pressure, oxygen saturation, level of consciousness, and urinary output. Each parameter deviation from normal values is assigned a risk zone indicated by the colors white, yellow, and red. MEOWS enables early identification of patients with objective signs of potential ongoing infection but is insufficient for sepsis diagnosis. Maternal sepsis diagnosis requires the presence—during pregnancy or childbirth, postabortion, or postpartum—of a presumed or confirmed infection associated with damage to 1 or more organs, as evidenced by specific criteria, such as oxygen requirement to maintain SpO_2_ >95% or PaO_2_/FiO_2_ <400, platelet count <100 × 10^6^/L, bilirubin level >1.2 mg/dL, systolic blood pressure <90 mm Hg or mean arterial pressure <75 mm Hg, patient arousable to stimuli (verbal, painful, or unconscious), and creatinine level >1.2 mg/dL. The presence of 1 or more of these organ damage criteria corresponds to a modified SOFA (mSOFA) score ≥1.
Management of Maternal Sepsis
Depending on MEOWS, mSOFA, and lactate values obtained through arterial blood examination of patients, different “risk zones” are identified, as depicted in Figure 1, outlining the appropriate pathway to follow. In particular, implementation of the Sepsis Six panel is necessary in all cases of intermediate risk (infection signs/symptoms + 2 yellow or 1 red MEOWS alert) and high risk (infection signs/symptoms + >2 yellow or >1 red MEOWS alert or mSOFA ≥1).
Definition of risk zone based on the Modified Early Obstetric Warning Score (MEOWS) and the modified Sequential Organ Failure Assessment (mSOFA). The image is the modified English version of a flowchart included in the “Operational Guidance Document for Early Identification and Management of Sepsis in Obstetrics” (supplementary materials, attachment 1). The Sepsis Six consists of 3 diagnostic and 3 therapeutic steps—all to be delivered within 1 hour of the initial diagnosis of sepsis:1. Deliver high-flow oxygen.2. Take blood cultures and consider source control.3. Administer empiric intravenous antibiotics.4. Measure serial serum lactates and send full blood count.5. Start intravenous fluid resuscitation.6. Commence accurate urine output measurement [10].
The bundle provides detailed instructions for performing cultures before antibiotics, recommending at least 2 sets of blood cultures (BCs) and the search for infection foci. Regarding antibiotics, intravenous administration within the first hour is recommended in suspected or confirmed cases of sepsis, and the combination of penicillin/β-lactamase inhibitor is suggested as the first choice in the treatment, considering the most common septic sources in the obstetric context.
With the bundle, there were educational activities that consisted of formal training sessions, educational meetings, and visual aids such as posters in emergency departments and patient care areas. Additionally, a paper MEOWS parameter collection form was introduced in all patient charts to improve the early recognition of sepsis.
Patient Characteristics
The demographic data included age and ethnicity. Clinical data included comorbidities (history of cancer, chronic kidney disease, chronic liver disease, autoimmune disease, and hematologic disease). Obstetric data comprised gestational age, type of delivery, and delivery complications. Sepsis data included the timing of sepsis identification (antenatal, peripartum, or in the puerperium), MEOWS and mSOFA scores, and lactate values.
Although a definition of pregnant patients at high risk has always been difficult to assess [16], according to Zhang et al [17] we defined this subgroup of patients as those who had at least 1 of the following conditions: age ≥40 years, prepregnancy body mass index ≥30, history of drug or alcohol abuse, arterial hypertension, cardiovascular disease, history of arterial or venous thromboembolic events, pregestational diabetes, renal disease, rheumatic disease, thyroid abnormalities, hematologic disease, pulmonary disease, psychiatric disorders, cancer, gestational hypertension, intrahepatic cholestasis of pregnancy, previous cesarean sections, and history of thromboembolic events during pregnancy.
Microbiological and Treatment Data
Microbiological data included the type of microorganism causing the infection with specific susceptibility profiles, the site of infections, and cultures of specific samples (eg, fetus, amniotic liquid, and placenta). BCs were defined positive according to Weinstein et al [18]. A positive BC result was defined polymicrobial when more than 1 pathogen was isolated from the same blood sample or from 2 consecutive blood samples of the same patient within 24 hours.
Coagulase-negative staphylococci, aerobic and anaerobic diphtheroid, Micrococcus spp, Bacillus spp, and viridans streptococci were considered contaminants if only 1 bottle of BC was positive. In this case, the isolate was reported as a probable contaminant, and susceptibility testing was not performed.
Bacterial isolates were defined as multidrug-resistant organisms when nonsusceptible to at least 1 agent in ≥3 antimicrobial categories or when harboring specific antibiotic resistance mechanisms (eg, methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus faecium, and extended-spectrum β-lactamase– or carbapenemase-producing Enterobacterales) [19]. Treatment data included the type of antibiotic, timing of administration, and total duration of the therapy.
To assess the appropriateness of antibiotic therapy, we reviewed all infections and evaluated whether the administered empiric antibiotic regimen was aligned with the spectrum of activity required for the subsequently isolated pathogen.
Outcomes Data
The outcomes data were structured into patient-centered outcomes and process measures, reflecting clinical impacts and key intervention metrics [20]. Patient-centered data encompassed a comprehensive assessment of maternal and neonatal health. For the mothers, the incidence of maternal death, admission to ICU, and length of stay (LOS) were evaluated.
The following were assessed for neonates: miscarriage (fetal death before 24 weeks of gestation), stillbirth (fetal death at ≥24 weeks of gestation), weight at birth, admission to the neonatal ICU (NICU), and early neonatal death (defined as mortality within the first 7 days of life). Process measures comprised the rate of lactate measurements, the rate of positive BC results, the time elapsed between the suspicion of sepsis and BC collection, the administration of antibiotics before sepsis suspicion and before proper collection of BCs, the appropriateness of empirical antibiotic therapy, the length of antibiotic therapy, and the frequency of requests for ID specialist consultations.
Objectives
The primary objective of this study was to assess whether the bundle implementation influenced the median LOS of the patients. Specifically, it aimed to determine if there was a decrease in LOS during the postbundle period as compared with the prebundle period.
Secondary objectives of the study were as follows:
To evaluate if there was a reduction in sepsis-related ICU admissions of patients during the postbundle period as compared with the prebundle period.To assess whether there was a decrease in the number of neonatal deaths or admissions to the NICU during the postbundle period as compared with the prebundle period.To determine if there was an increased request of lactates in the suspected cases of maternal sepsis in the postbundle period as compared with the prebundle period.To determine if there was an increased rate of BCs requested in the postbundle period as compared with the prebundle period.To examine if the time interval between the suspicion of sepsis and BC collection improved after the bundle implementation.To determine if there was a reduction in the rate of antibiotics initiated before BC collection.To determine if there was an increase of the appropriateness of antibiotic therapy in the postbundle period as compared with the prebundle period.To determine if the length of antibiotic therapy was shorter in the postbundle period as compared with the prebundle period.To investigate whether there was a significant rise in the number of ID consultations postbundle.
Sample Size Calculation
From a clinical perspective, we were primarily interested in evaluating how the implementation of the bundle influenced patient clinical outcomes. Since maternal sepsis remains a rare event and severe outcomes such as mortality are fortunately even less frequent, the choice of LOS as the primary outcome of this study was driven by methodological considerations, particularly the need to ensure an adequate sample size. Therefore, although we recognize the inherent limitations of LOS as an outcome, as it may be affected by multiple factors beyond infection management, we believe that it provides valuable insight into the overall impact of the bundle on maternal care.
Assuming an initial mean hospital stay of 14 days (SD, 2), we anticipate a clinically meaningful reduction of 2 (2) days in the postbundle group. Based on these estimates, a minimum of 52 patients (26 in each group) is required to detect this difference with 80% power while maintaining a type I error rate of 1% (α = .01). This sample size was determined through power analysis, ensuring that our study is adequately powered to identify changes in patient outcomes attributable to the bundle intervention. The estimated patient count is consistent with the catchment population and expected incidence of sepsis in pregnancy in the participating hospitals.
Statistical Methods
Median and IQR were used to describe continuous variables. Categorical variables were represented with absolute frequencies and percentages.
Appropriate statistical tests were conducted to compare variables between the pre- and postbundle groups, selected per the nature of the variables. Fisher exact test or χ^2^ test was applied for categorical variables, as appropriate, after checking for violation of Pearson χ^2^ expected frequencies assumption. For continuous variables, the Wilcoxon rank sum test was employed to compare the distributions between the groups.
Statistical significance was fixed for P values <.05. Statistical analyses were conducted with R (version 4.2.1).
RESULTS
Overall, 80 women with sepsis during pregnancy or puerperium were included, with a median age of 31.0 years (IQR, 26.0–36.3). Among them, 24 (30.0%) were evaluated in the prebundle period and 56 (70.0%) in the postbundle period (Figure 2).
Flowchart of study population.
Regarding the history of these patients, few underlying comorbidities were reported, with thyroid abnormalities being the most frequent (13/80, 16.3%). Moreover, 9 (11.3%) patients previously underwent abdominal surgery. Seven (8.8%) patients had a penicillin allergy, while 3 (3.8%) already had a septic event.
Regarding previous pregnancies, 42 (52.5%) patients were primiparas while 16 (20.0%) had at least 1 previous cesarean section. More than half of patients (52/80, 65%) had a high-risk pregnancy: 15 of 24 (63%) in the prebundle period and 37 of 56 (66%) in the postbundle period (P = .759). Eight (10.0%) patients had sepsis during or following a multiple pregnancy, while the most frequent pregnancy complication was premature preterm rupture of membranes (16/80, 20.0%).
Delivery data were collected from 58 patients (15 prebundle and 43 postbundle) who ended their pregnancy during the same hospital admission of the septic event. Specifically, most patients underwent a cesarean section (n = 35, 60.3%) while 20 (34.5%) needed an induction of labor. In available medical records, 14 (30.4%) patients received an antibiotic prophylaxis in the peripartum period.
Gestational age at the time of delivery was lower in prebundle patients as compared with postbundle, with a median 26.0 weeks (IQR, 17.0–33.0) vs 37.0 (27.0–39.8; P = .006). Concerning the delivery complications, nearly a third of women (15/55, 27.3%) experienced a postpartum hemorrhage while 14 of 53 (26.4%) underwent manual removal of retained placenta. Demographic, clinical, and obstetric-delivery data of the study cohort are reported in Table 1.
Overall, sepsis occurred in 30 patients (37.5%) during the antenatal period, 16 (20.0%) during the peripartum period, and 34 (42.5%) during the puerperium. In the postbundle period, there was a significant increase in postpartum cases and a decrease in cases during pregnancy (P = .021). Data on sepsis are presented in Table 2.
The primary source of infection was urinary (n = 32, 40.0%), followed by chorioamnionitis (n = 23, 28.8%) and genital tract infections (n = 12, 15.0%). Regarding disease severity, 51 (69.9%) of 73 patients had a mSOFA ≥1, while among those in the postbundle period group, 38 of 42 (90.5%) had a high- or intermediate-risk score on MEOWS. In terms of imaging, slightly more than half of the patients (n = 42, 52.5%) underwent ultrasound or x-ray, while 20 (25.0%) required a computed tomography scan. Table 3 shows the microbiological data.
Among the 52 positive BC results, 56 pathogens were identified, with 4 of 52 (7.7%) showing a polymicrobial infection. The most frequently isolated bacteria were Enterobacterales, namely Escherichia coli (27/56 48.2%) and Klebsiella pneumoniae (11/56, 19.6%), followed by anaerobic bacteria (6/56, 10.7%) and gram-positive bacteria such as Streptococcus spp (6/56, 10.7%), Enterococcus spp (3/56, 5.4%), and Staphylococcus spp (3/56, 5.4%). Multidrug-resistant organisms accounted only 2 (3.6%) of the 56 isolated pathogens: 1 methicillin-resistant S aureus and 1 methicillin-resistant Staphylococcus epidermidis. No vancomycin-resistant E faecium or extended-spectrum β-lactamase/AmpC/carbapenemase–producing Enterobacterales was found.
Details on microbial isolates in urine, vaginal swab, placenta, and fetus/newborn cultures are reported in Supplementary Table 1 and the supplementary materials (attachment 2). Most patients (51/80, 63.8%) received penicillins (primarily piperacillin/tazobactam) as monotherapy or in combination as empiric antibiotic therapy.
Patient-Centered Outcomes
Regarding the primary objective of the study, the median LOS was 13.0 days (IQR, 9.0–18.3), with no differences between the periods. Notably, no maternal deaths or stillbirths occurred in either group. Of 80 patients, 22 (27.5%) required ICU admission, with 9 patients (37.5%) in the prebundle period and 13 (23.2%) in the postbundle period. Although there was a reduction in the number of ICU admissions in the postbundle period, this difference was not statistically significant (P = .200). Of 58 pregnancies, 15 (25.9%) ended in miscarriages: 7 of 15 (46.7%) in the prebundle period and 8 of 43 (18.6%) in the postbundle (P = .045). A significantly lower percentage of newborns required NICU admission after the introduction of the bundle, with 6 of 7 (85.7%) and 10 of 32 (31.3%) in the pre- and postbundle periods, respectively (P = .013). Early neonatal death (within 7 days) occurred in 3 newborns (7.7%) for the overall cohort.
Process Measures
Regarding the secondary objectives and the process measures, the lactate measurement was assessed in 80 patients overall, with an increase in the postbundle period (52%) as compared with the prebundle period (38%), but this difference was not statistically significant (P = .200). Similarly, the rate of BCs requested increased in the postbundle period (75%) vs the prebundle period (59%, P = .222). Following the same trend, the median time between suspected sepsis and BC collection improved from 11.0 hours (IQR, 0.0–28.0) prebundle to 2.0 hours (0.8–21.3) postbundle, but no significant difference was observed (P = .800). Importantly, more than half of the patients (51.9%) were already undergoing antibiotic treatment before sepsis suspicion, and 65.8% had received antibiotics before BC collection, with no significant difference between the pre- and postbundle periods.
Empirical antibiotic therapy was appropriate in 75% of cases overall, increasing from 69% in the prebundle group to 77% in the postbundle group, although this change was not statistically significant. Moreover, the median duration of treatment was similar in the 2 groups, with 8.0 days (IQR, 7.0–14.0) prebundle and 11.0 days (7.3–16.0) postbundle (P = .297).
Finally, there was a significant increase in ID specialist consultations in the postbundle period (75.0%) as compared with the prebundle period (50.0%, P = .029). Table 4 reports details about treatment and outcome data, and Table 5 reports details about the process measure outcomes.
DISCUSSION
During the study period, a total of 80 patients developed maternal sepsis, with 50 cases occurring in the peripartum and puerperium periods. The primary infection source was urinary, predominantly caused by E coli, and penicillins were the most frequently prescribed antibiotics. These findings align with existing data from high-income countries, where E coli is a leading pathogen in maternal sepsis, with urinary and genital tract infections being most common [21, 22]. Similarly, World Health Organization data from the GLOSS group confirm these findings, suggesting that cephalosporins and amoxicillin are commonly prescribed in similar populations [23]. In light of these consistent findings, our study contributes to a growing understanding of pathogen patterns and treatment practices in maternal sepsis, highlighting a critical area for focused intervention.
The bundle did not significantly reduce maternal LOS or ICU admissions. However, there was a reduction in NICU admissions observed, although the contribution of the bundle implementation to this change remains uncertain. Given the different median gestational age between pre- and postimplementation groups (26 vs 37 weeks), it is possible that preterm monitoring requirements contributed to fetal outcome differences. These differences between the populations may be due to chance but also could be seen as an effect of the bundle itself in that it may have standardized early recognition of sepsis across gestational ages, potentially shifting clinical focus beyond high-risk preterm cases. We believe that this potential change in focus may represent an important but often overlooked advantage of bundles—namely, improving overall sepsis awareness and response rather than merely targeting high-risk groups [24].
Moreover, the significant increase in sepsis diagnoses during the postpartum period and the corresponding reduction in cases during pregnancy in the postbundle group, along with differences in sample sizes and population characteristics, complicate the attribution of observed improvements solely to the bundle. The postbundle cohort was larger and coincided with heightened clinical awareness, which may have influenced outcomes beyond the bundle's direct impact. This also suggests that while standardized protocols are beneficial, their success is contingent upon institutional engagement, clinician adherence, and preexisting clinical culture [25].
To assess the impact of the sepsis bundle, key process-specific metrics were analyzed. Despite a nonsignificant improvement in several process measures, the observed trend suggests a positive evolution of diagnostic and management strategies. Notably, ID consultations significantly increased in the postbundle period, reflecting the explicit recommendation in the bundle to involve ID specialists early. In fact, prompt ID involvement has been already recognized as a key factor in improving sepsis outcomes in other populations [26].
Antibiotic appropriateness remained unchanged between the pre- and postbundle groups despite the bundle's focus on antimicrobial stewardship. This aligns with other studies highlighting challenges in achieving consistent antibiotic adherence in sepsis management [27]. Continued efforts, including real-time feedback and clinician education, remain crucial for improving antimicrobial stewardship [28]. The persistent issue of inappropriate microbiological sampling timing, with more than half of the patients receiving antibiotics before BC collection, underscores the need for further optimization of bundle adherence. This gap, despite bundle implementation, reflects ongoing difficulties in prioritizing BCs before antibiotic initiation, as noted in the literature [29].
This study has several important limitations. The retrospective design limits control over confounding variables, and data collection from 7 hospitals introduces variability in documentation practices. The prebundle sample size (n = 24) was slightly below the target of 26 but remained close to the original estimate, and a post hoc power analysis confirmed sufficient statistical power. Additionally, differences in population characteristics between periods suggest that improved neonatal outcomes cannot be attributed solely to bundle implementation but may reflect evolving clinical practices.
Despite these limitations, this study provides valuable insights. It is among the first to examine the effects of the Surviving Sepsis Campaign guidelines on maternal and neonatal outcomes, addressing a gap in existing literature. Implementing a structured bundle across multiple hospitals allowed for a comprehensive evaluation of sepsis management in pregnancy and puerperium. Moreover, a key aspect of the bundle's implementation was the adoption of multiple educational strategies to enhance guideline adherence, including the awareness of the potential benefit of increasing the ID specialists' involvement.
In conclusion, this study underscores the need for localized, condition-specific guidelines that adapt Surviving Sepsis Campaign principles to obstetric populations, ensuring better adherence and improved maternal and neonatal outcomes. Future efforts should focus on enhancing guideline adherence through targeted education, real-time feedback mechanisms and tailored antimicrobial stewardship strategies.
Supplementary Material
ofaf337_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Say L, Chou D, Gemmill A, et al Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health 2014; 2:e 323–33.25103301 10.1016/S 2214-109X(14)70227-X · doi ↗ · pubmed ↗
- 2Turner MJ . Maternal sepsis is an evolving challenge. Int J Gynaecol Obstet 2019; 146:39–42.31037723 10.1002/ijgo.12833 · doi ↗ · pubmed ↗
- 3World Health Organization . Statement on maternal sepsis. 2017. Available at: https://www.who.int/publications/i/item/WHO-RHR-17.02 Accessed 24 Jun 2025.
- 4Bridwell RE, Carius BM, Long B, Oliver JJ, Schmitz G. Sepsis in pregnancy: recognition and resuscitation. West J Emerg Med 2019; 20:822–32.31539341 10.5811/westjem.2019.6.43369 PMC 6754194 · doi ↗ · pubmed ↗
- 5Rhodes A, Evans LE, Alhazzani W, et al Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med 2017; 43:304–77.28101605 10.1007/s 00134-017-4683-6 · doi ↗ · pubmed ↗
- 6Singh S, Mc Glennan A, England A, Simons R. A validation study of the CEMACH recommended modified early obstetric warning system (MEOWS)*. Anaesthesia 2012; 67:12–8.22066604 10.1111/j.1365-2044.2011.06896.x · doi ↗ · pubmed ↗
- 7Shields LE, Wiesner S, Klein C, Pelletreau B, Hedriana HL. Use of maternal early warning trigger tool reduces maternal morbidity. Am J Obstet Gynecol 2016; 214:527.e 1–6.10.1016/j.ajog.2016.01.15426924745 · doi ↗ · pubmed ↗
- 8Umar A, Ameh CA, Muriithi F, Mathai M. Early warning systems in obstetrics: a systematic literature review. P Lo S One 2019; 14:e 0217864.31150513 10.1371/journal.pone.0217864 PMC 6544303 · doi ↗ · pubmed ↗