Patient-reported symptoms in the detection of head and neck cancer recurrence: a systematic review
Kate Hulse, Rhona Hurley, Anja Lowit, Roma Maguire, Claire Paterson, Catriona M. Douglas

TL;DR
This study reviews how well patients can detect head and neck cancer recurrence through reported symptoms, finding that symptoms are not very sensitive but highly specific.
Contribution
The paper provides a systematic review of patient-reported symptoms for detecting HNC recurrence, highlighting their limitations and potential for improvement.
Findings
The median sensitivity of patient-reported symptoms to detect recurrence is 47.3%.
Patient-reported symptoms have a high specificity (79.3%) and negative-predictive value (98.0%).
New symptoms are often reported during routine follow-up rather than urgent appointments.
Abstract
Patient-initiated follow-up (PIFU) after treatment for head and neck cancer (HNC) relies on the signs and symptoms of recurrence being detectable by patients. We examine the evidence for patient-reported symptoms as an indicator of recurrence. A search was conducted via OvidMEDLINE and Embase (2010 to January 2024) plus sources of grey literature for studies which describe patient-reported symptoms and recurrent disease. Findings are reported as per PRISMA guidelines. Twenty studies were included which were highly heterogenous. The median sensitivity of patient-reported symptoms to detect recurrence is 47.3%. Median specificity, positive-predictive value (PPV) and negative-predictive value (NPV) were 79.3%, 9.3% and 98.0% respectively. New symptoms were generally reported at routine follow-up rather than expedited appointments. The high specificity and NPV of patient-reported…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
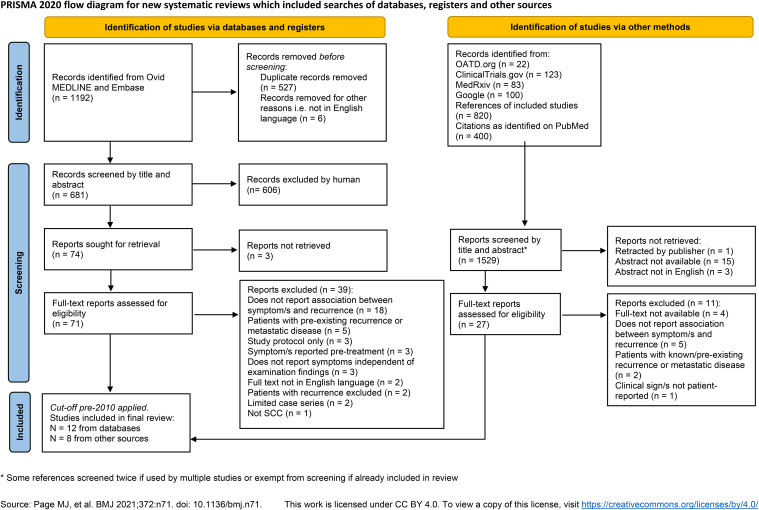 Figure 1
Figure 1| Author | Country | Year of publication | N | Period of treatment | Tumour primary site and stage | Primary treatment | Nature of patient-reported symptom/s | Key finding/s related to symptomatic recurrence or second primary |
|---|---|---|---|---|---|---|---|---|
| Belcastro | USA | 2021 | 89 | 2010-2019 | Oropharyngeal SCC (50.6% HPV-positive). | Surgical treatment +/- adjuvant CRT (rates NS) | New throat pain or otalgia | 32 (36%) patients had a recurrence/SP. |
| Blatt | Germany | 2022 | 760 | 2000-2015 | All oral SCC. Stage NS, 198 (29%) T3/4. | Primary surgery | Self-reported symptoms, not pre-defined | 216 (28.4%) patients had a recurrence, of which 18 (8%) were detected via self-reported symptoms. |
| Brands | Netherlands | 2022 | 307 | 2006-2012 | All oropharynx, 155 (50.5%) HPV PCR or P16-positive. 250 (81%) stage III/IV. | RT alone 187 (61%), CRT 81 (26%), surgery + RT/CRT 30 (9.8%) | Routine or interval visit and whether patient-initiated plus “potential signs and symptoms of new disease” | 81 (26.4%) locoregional recurrence or SP of which 69 (85.2%) were symptomatic. 100% of SP tumours were symptomatic. |
| Daga | India | 2021 | 700, of which 189 FU | FU 2020 | Whole cohort (including new cancer cases) 554 (80%) oral cavity. 623 (89.9%) stage III/IV. | NS | Symptoms inc. pain, ulceration, swelling and weight loss | 81 (43%) of FU patients were symptomatic of which 12 (14.8%) had recurrence. Rate of recurrence in asymptomatic patients not given. |
| Ellis | UK | 2021 | 5123 | FU 2017-2018 | 1845 (36%) oropharynx, 1151 (22.5%) glottic and 527 (10.3%) oral cavity most common subsites. Stage NS, 1781 (34.8%) T3/4. | 2123 (41.4%) surgery to primary site, 2756 (53. 8%) RT +/- CT. 1661 (32.4%) neck dissection and/or 3132 (61.1%) RT to at least one neck. | New symptoms since previous consultation, not pre-defined | 122 patients had recurrence or SP, and an additional 50 patients had residual disease (within 6 months). Of all confirmed malignancy, 86 (50%) were asymptomatic. |
| Ilmarinen | Finland | 2018 | 153 (366 FU visits) | FU 2014 | All oropharynx, 110 (72%) p16-positive. 132 (86.3%) stage III/IV. | 93 (61%) CRT, 38 (25%) surgery + RT/CRT | New symptoms that raise suspicion of cancer recurrence or patient-requested visit | 4 (3%) patients developed recurrence, all of which were symptomatic. |
| Lin | Taiwan | 2015 | 136 | TNO (post-treatment) 2010-2014 | HNSCC plus oesophageal synchronous primaries 33.8%, hypopharynx 29.4%); remainder oropharynx, larynx and oral. 77.2% stage III/IV disease. | Majority surgery + adjuvant CRT (36.8%), primary CRT (30.9%) or surgery single modality (20.6%) | All had swallowing disorder e.g. weight loss, dysphagia, odynophagia, choking, hoarseness, prolonged tube feeding, lumping throat | 45 (33.1%) patients had a recurrence/SP, all patients in cohort had swallowing disorder. |
| Malik | India | 2020 | 400 | 2018-2019 | All oral cancer <2 years since treatment. | Surgery plus 348 (87%) received adjuvant RT/CRT | Symptoms suggestive of recurrence inc. problem in speaking, new growth/ulcer in the mouth, pain in head/neck region, new neck swelling | Recurrence confirmed in 20 (5%) patients, of which the pre-clinic telephone questionnaire identified 18 (90%) however the specificity was worse than for clinical examination (75.5% versus 92.9%). |
| Masroor | USA | 2019 | 233 (3358 FU visits) | 2011-2014 | HPV-positive oropharyngeal SCC. 18 (7.7%) stage III disease, no stage IV. | Primary CRT (68.2%), surgery + adjuvant RT/CRT (20.6%), single modality RT or surgery | Recurrences ‘symptom-directed’ where patient symptoms prompted work-up, not pre-defined | 23 recurrences, of which 11 (47.8%) - in 10 patients - were symptomatic and only 1 detected by physician examination. Remaining diagnosed on post-treatment PET-CT. |
| Miyamaru | Japan | 2023 | 440 | 2009-2018 | Oral cavity (35%), hypopharynx (29%) and larynx (28%) most common subsites. 56% stage III/IV disease. | Surgical resection +/- adjuvant RT/CRT | Patients asked about “unusual symptoms” at regular follow-up, not pre-defined | 133 (30.2%) patients had 160 recurrences. 7/35 (20%) local recurrences, 17/68 (25%) regional recurrences and 5/57 (9%) of distant metastases were detected by symptom-based examination; compared with 46%, 16% and 0% with clinical examination. |
| Pagh | Denmark | 2013 | 619 | FU 2012 | Oropharynx 199 (32%), larynx 144 (23%) and oral cavity 137 (22%) most common subsites. Stage NS. | Primary RT/CRT 419 (67.7%), surgery alone 107 (17.3%), surgery + RT 83 (13.4%) | Validated patient-reported symptom questionnaire from ESTRO, planned versus patient-requested FU | Recurrence or SP diagnosed in 29 (4.7%) patients of which 22 (75.9%) had symptoms. 19/22 (86.4%) symptomatic patients presented at routine FU. |
| Pakkanen | Finland | 2021 | 303 | 2003-2015 | All T1 glottic cancer | 163 (53.8%) surgery and 140 (46.2%) RT | Not pre-defined | 38 (12.5%) patients had recurrence, of which 17 (44.7%) had new symptoms. |
| Srivastava | India | 2015 | 86 | 2008-2012 | Patients who still had pain at 6 weeks post-RT. 31 (36%) oropharynx, 19 (22.1%) larynx and 18 (20.9%) oral cavity most common subsites. 68 (79%) stage III/IV. | All RT/CRT | Persistent pain 6 weeks and 3 months after completion of RT | 60% of patients with neuropathic-type pain at 6 weeks had a later recurrence. |
| Stimpson | Australia | 2014 | 260 (321 FU visits) | FU 2013 | NS | NS | “Presence or absence of new symptoms” not pre-defined | New symptoms reported at 59 appointments and 27 were expedited. 9 (3.5%) recurrences in total, 8 symptomatic and 1 asymptomatic. |
| Su | USA | 2018 | 33 | 2005-2016 | All oropharynx HPV-positive. 10 T3/4. | NS | Not further specified | 16 patients had a recurrence, 13 of whom were asymptomatic at time of recurrence detection. 12 recurrences were detected via PET-CT and none with physical examination. |
| Tufano-Sugarman | USA | 2023 | 19 | 2011-2019 | Mostly oral cavity primary (84.2%), remainder nasopharyngeal or sinus. | 18 (95%) received CRT | All patients with suspected osteoradionecrosis | 7 (36.8%) patients investigated for suspected ORN had cancer recurrence or persistent disease. |
| Van de Weerd | Netherlands | 2024 | 413 | 2006-2012 | All larynx - 264 (64%) glottic, 138 (33%) supraglottic. 132 (32%) stage III/IV. | 255 (61.7%) RT/CRT, 106 (26%) surgery only, 52 (12.6%) surgery and RT/CRT | Hoarseness, change of voice, dyspnoea, dysphagia, globus sensation, pain at primary site, otalgia, bleeding or bloody sputum, neck lump | 126 (30.5%) patients had recurrence, of which 98 (82%) reported symptoms at time of detection. 6 (5%) unknown symptom status. |
| Van Nuffel | Belgium | 2023 | 132 | 2005-2017 | Oropharynx (70.5%), hypopharynx (29.5). 86.4% stage III/IV disease. | Primary CRT (53%), primary RT only (26.5%), single modality surgery +/- adjuvant RT/CRT | “Clinical symptoms at the time of diagnosis” of recurrence | 61 (46.2%) patients had recurrence and 24 (17.8%) developed a SP tumour. 44 (72.1%) were clinically apparent or symptomatic; 11/39 (28%) patients with clinically occult recurrence had new symptoms suggestive of recurrence. |
| Wakasugi | Japan | 2022 | 150 | 2010-2019 | Oropharynx 39 (26%), hypopharynx 52 (34.7%) and oral cavity 26 (17.35) most common subsites. All stage III/IV. | Surgery plus CRT or CRT alone | “Symptoms at the time of detection of recurrence” | 63 (42%) patients had recurrence and 22 (14.7%) SP tumour of which 38 (60.3%) and 8 (36.4%) were symptomatic respectively. |
| Zhang | UK | 2022 | 1066 | FU 2020 | Oropharynx 426 (39.7%) and larynx 302 (28.2%) most common subsite. Includes small proportion of thyroid and skin. | NS | 6m remote telephone triage and assessment of new symptoms | 34 (3.2%) developed a recurrence during the study period. |
| Author (year) | N | Study design | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|
| Belcastro (2021) ( | 89 | Retrospective | 71.8 | - | - | - |
| Blatt (2022) ( | 760 | Retrospective | 9.1 | – | – | – |
| Brands (2022) ( | 307 | Retrospective | 85.2 | - | - | - |
| Ellis (2021) ( | 5123 | Retro/prospective | 50.0 | 77.2 | 7.1 | 97.8 |
| Ilmarinen (2019) ( | 153 | Retrospective | 100 | 87.9 | 18.2 | 100 |
| Malik (2020) ( | 136 | Prospective | 90.0 | 75.5 | 16.2 | 99.3 |
| Masroor (2019) ( | 233 | Retrospective | 47.8 | - | - | - |
| Miyamaru (2023) ( | 440 | Retrospective | 18.1 | – | – | – |
| Pagh (2013)( | 619 | Prospective | 75.9 | - | - | - |
| Pakkanen (2021) ( | 303 | Retrospective | 44.7 | – | – | – |
| Srivastava (2015) ( | 86 | Retrospective | 94.7 | 56.7 | 38.3 | 97.4 |
| Stimpson (2014) ( | 260 | Prospective | 88.9 | 83.7 | 13.6 | 99.6 |
| Su (2018) ( | 33 | Retrospective | 11.5 | - | - | - |
| Van de Weerd (2024) ( | 413 | Retrospective | 86.0 | – | – | – |
| Van Nuffel (2023) ( | 132* | Retrospective | 72.1 | - | - | - |
| Wakasugi (2022) ( | 150 | Retrospective | 54.1 | – | – | – |
| Zhang (2022) ( | 1066 | Prospective | 35.3 | 89.1 | 5.4 | 97.7 |
- —Chief Scientist Office, Scottish Government Health and Social Care Directorate 10.13039/100014589
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Cancer Studies · Cancer Diagnosis and Treatment · Oral health in cancer treatment
Introduction
1
Head and neck cancer (HNC) is the 8^th^ most common cancer in the UK (1). Following treatment, over a third of patients experience recurrence depending on the tumour stage and primary site. Treatment options for recurrent disease include salvage surgery, re-irradiation, palliative chemotherapy and/or immunotherapy. A recent meta-analysis reported 5-year overall survival following salvage surgery between 26-67% (2). Salvage treatments generally carry significant morbidity but are more likely to be successful if recurrence is detected at an earlier stage (3) and therefore the emphasis remains on early identification.
The rationale for follow-up after HNC treatment is the detection of recurrent disease and the management of post-treatment toxicity. Current UK recommendations are for patients to be seen at least every 2 months for the first 2 years, followed by every 3–6 months for a minimum of 5 years in total. It is recommended that patients should have clinical examination at every follow-up including, when appropriate, nasopharyngolaryngoscopy (4). Patient-initiated follow-up (PIFU) is not currently routine practice, and many patients prefer a scheduled follow-up approach for reassurance and reliable access to information (5). PIFU has been mooted in HNC since there is limited evidence that regular follow-up impacts survival outcomes and outpatient capacity can struggle to meet the demand of recommended appointment frequency. A recent systematic review of PIFU following treatment for other cancer types found similar rates of recurrence, survival, quality of life, fear of recurrence and patient satisfaction in breast and colorectal cancer compared to conventional follow-up. However, it is noted that all breast cancer PIFU programmes included regular mammograms and colorectal PIFU programmes included either regular testing for faecal occult blood or CT scans (6).
For PIFU to replace the function of routine surveillance in HNC, it should be a reliable tool to identify recurrence; this has not yet been demonstrated but is the subject of on-going research (7). In this systematic review, we aim to examine the value of patient-reported symptoms in the detection of recurrence and second primary (SP) in HNC and therefore the potential role of symptoms in PIFU.
Methods
2
Eligibility criteria
2.1
Inclusion
2.1.1
Studies describing patient-reported signs or symptoms after curative treatment for Head and Neck squamous-cell carcinoma (HNSCC),Some or all the patients in the cohort received primary cancer treatment after January 2010,Studies report rates of recurrence and/or SP detection in relation to patient symptoms,Full text available in English.
Exclusion
2.1.2
Study subjects have known recurrent or metastatic HNSCC, non-SCC histology, cutaneous, upper oesophageal cancer or thyroid cancer,Patients receiving palliative or non-curative treatment,Case reports,No original data presented e.g. review articles.
Information sources
2.2
The search was conducted on OvidMEDLINE (1974 to January 26 2024) and Embase (1946 to January 26 2024). Sources of grey literature were searched via four channels: the online repository Open Access Thesis and Dissertations (oatd.org), ClinicalTrials.gov, MedRxiv, and a Google search where the first 100 hits were screened for relevance. The references and citations of included studies were also subject to screening followed by full-text review if deemed relevant.
Search strategy
2.3
This review was registered on PROSPERO (CRD42024510566) and reported according to PRISMA guidelines (8). OvidMEDLINE and Embase were searched separately using the following terms: (head and neck cancer) AND (patient reported or patient-reported or symptom) AND (recurrent or recurrence or second primary).* “Head and neck cancer” as subject/keyword and “recurrence” were used to search the oatd.org database with a filter for English-language. The search terms are described in detail and for other sources in Appendix 1.
Selection process
2.4
Duplicates were manually removed by screening of the title, first author name and year of publication. Abstracts were screened for inclusion or exclusion by two authors (KH and RH) according to the criteria above and full-text review was performed with over-sight by CD who made a final decision on inclusion in cases of disagreement.
A cut-off of treatment prior to 2010 was applied since the wide-spread adoption of intensity-modulated radiotherapy (IMRT) around this time reduced treatment-related long-term sequelae (9). Similarly, the role of human-papilloma virus (HPV) in oropharyngeal cancer was recognised and changed the understanding of risk and recurrence related to these cancers (10).
Data collection
2.5
Data was extracted by KH. Data items retrieved were the first author, country of study, year of publication, number of patients included in study, period of patient treatment, demographic and clinical characteristics of patients, the patient-reported outcome measure used, and key findings related to recurrence of disease or SP.
Effect measures
2.6
Data was collected on the number of true positives (patients with reported symptoms and confirmed recurrence), true negatives (asymptomatic patients without recurrence), false positives (symptomatic without recurrence) and false negatives (asymptomatic with recurrence). Where sufficient data was reported a calculation of sensitivity, specificity, positive-predictive value (PPV) and negative predictive value (NPV) was performed. Confidence intervals of 95% were calculated using RStudio 2024.12.0.
Synthesis methods
2.7
Variables as described above were tabulated. A narrative synthesis of results was performed. Studies were almost exclusively observational in nature with heterogenous study populations and study design therefore meta-analysis could not be meaningfully performed.
Quality assessment and risk of bias
2.8
Most of the studies were a cohort study involving longitudinal observation of a group of patients following treatment and assessment of their outcomes. There are no recommended risk-of-bias tools specific to this study design. The following sources of potential bias were assessed, derived from the Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies (11): 1) representativeness of the population, 2) method of assessing symptoms, 3) adequacy of follow-up and 4) identification of and control for potential confounding factors.
Results
3
Study selection
3.1
The search of OvidMEDLINE and Embase yielded a total of 1192 results. After de-duplication there were 887 records remaining. Six articles were removed as the publication was not available in English language and a further 213 were removed as the full text was not available e.g. conference abstract only. The remaining 668 records were reviewed by KH and RH for eligibility. Twenty-two theses were also screened for inclusion and one dissertation was sought for full-text review. ClinicalTrials.gov search yielded 123 records which were screened for relevance, but none sought for full-text review. MedRxiv found 83 records, 1 sought for full-text review. A Google search did not yield any previously unfound records. The cut-off for treatment time prior to 2010 was applied to the final set of records since it is not possible to search or filter for this in the conventional way. The process of study selection is shown in the PRISMA flow-diagram (Figure 1).
*PRISMA flow diagram shows the data sources, excluded records and reasons for exclusion. Some references screened twice if used by multiple studies or exempt from screening if already included in review. Source: Page MJ, et al. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. This work is licensed under CC BY 4.0. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.
Study characteristics
3.2
A total of 20 studies are included in this review, published between 2013-2024. Key features and results of individual studies can be found in Table 1 (12–31). The study populations represent a heterogeneous group of patients with different primary disease site and stages and varying treatment modalities. There are 17 cohort studies, of which 4 are retrospective. In these studies, the rate of symptomatic and asymptomatic recurrences or SP are generally reported however few state the rate of patient-reported symptoms in the whole cohort. There were 3 case series, of which 2 assessed a patient group which were all symptomatic.
Quality and risk of bias
3.3
The focus of the studies varied greatly, and in some cases, represent a narrow subset of the HNC patient population. For example, Pakkanen et al. only include T1 laryngeal cancer and Wakasugi et al. only include patients with locally advanced (T3/4) disease. The studies by Lin and Tufano-Sugarman, whose patients all had swallowing problems and symptoms in-keeping with osteoradionecrosis respectively, are not typical of the HNC post-treatment population. One study of patients with oropharyngeal tumours included only those who received surgical treatment, whereas the usual treatment modality for many of these patients would be primary chemoradiotherapy and therefore this is also an atypical cohort.
In most studies, the nature of patient-reported symptoms was either entirely undefined or loosely described, such as symptoms “suggestive of recurrence”. One paper used a validated questionnaire to capture patient-reported symptoms (22). We cannot be confident of the completeness of symptom data when collected retrospectively from patients’ notes although this is most pertinent for the absence of symptom data as symptoms are unlikely to have been recorded as present in error.
Seventeen studies followed patients up for an adequate length of time for recurrence to become apparent after the onset of recorded symptoms. The study by Daga et al. presented a retrospective audit of patients with HNC presenting to the hospital during a period of COVID lockdown in India for 2 months. Stimpson and colleagues invited patients attending follow-up to complete a questionnaire which included questions about the presence or absence of new symptoms. This was compared with findings at the clinic appointment, such as suspicious of recurrence. Therefore these two studies only represented a snapshot which could potentially miss recurrence associated with the reported symptoms. Since most studies were retrospective, there was not an issue with loss to follow-up or patient attrition and generally reporting bias was not a concern as all cases or consecutive cases within the period were reported.
Since most of the cohort studies were not primarily designed to evaluate symptomatic recurrence, few identified and attempted to account for associated confounding factors which could have influenced the rate of symptomatic recurrence, such as stage or treatment modality. Ten studies identified and controlled for one or more other factors which might influence the prevalence of post-treatment symptoms.
Results of synthesis
3.4
The diagnostic power of patient-reported symptoms to detect recurrence as reported in the 17 cohort studies are shown in Table 2. The median sensitivity is 47.3% [CI 44.3, 50.2], so fewer than half of patients with a recurrence will have recognisable symptoms. The reported sensitivity ranged widely from 9.1% to 100%. There was no obvious association between the predominant cancer subsites represented in the study and the sensitivity of patient-reported symptoms. Indeed, the worst reported sensitivity was in a cohort of patients all with oral cancer (13), but another study of entirely oral cancer patients by Malik et al. reported 90.0% sensitivity (19). The second worst reported sensitivity was in a study of patients with HPV-positive oropharyngeal cancer by Su et al, however the highest reported sensitivity was in the study by Ilmarinen which was also all patients with oropharyngeal cancer, of which 72% were HPV-positive. A much greater proportion of patients in the latter study were advanced stage, but again this is not a consistent pattern across the studies.
Sufficient data was reported in 6 cohort studies to calculate specificity, PPV and NPV of which the median is 79.3% [CI 78.3, 80.2], 9.3% [CI 7.9, 10.8] and 98.0% [CI 97.6, 98.3] respectively. This does not include case-controlled studies where either all patients were symptomatic, or all had recurrent disease. Data was able to be retrieved from studies representing all cancer subsites but only the studies by Ilmarinen and Malik included a single subsite. The specificity ranges from 56.7 - 89.1%, meaning that most patients who are asymptomatic will not have a recurrence (true negative), however symptoms are not a highly specific indicator of disease. Both PPV and NPV are determined by the prevalence of disease in the population. Five out of the six studies reported a very low recurrence rate (≤5%) and therefore NPV is expected to be high since it is inversely related to prevalence.
The most frequent patient-reported signs and symptoms varied slightly between studies but were predictable ‘red flags’ such as throat pain, hoarseness and difficulty swallowing. There is limited evidence for the relationship between the timing of patients’ symptoms and recurrence e.g. whether new onset is more pertinent. Of note, several studies report the number of patients expediting their appointments due to symptoms but there appears to be a significant cohort of patients across the studies who experienced symptoms but were seen at routine follow-up intervals.
Discussion
4
Results in context
4.1
Morbidity following treatment for HNC is common and, in the included studies, the recording of symptom rate in individuals without recurrence is poor. A European study of all cancer types (mostly breast cancer) following radiotherapy found a symptom rate of 55% and a quarter of these symptomatic patients had a recurrence (32). In comparison, the PPV of symptoms in HNC is consistently poor. This may be because the overall rate of symptoms in HNC is higher and therefore it is less discriminating for disease. A PIFU service for HNC may therefore be less efficient at detecting recurrent disease than in other cancers and have less impact in reducing follow-up demand. It also bears repeating that in PIFU programmes for other cancer types, additional testing including imaging is performed routinely (6). Since UK guidance is currently only to perform additional post-treatment imaging if clinically indicated, any such PIFU programme in HNC would need to determine on what basis imaging is requested. If it is based on symptoms then this could drive a significant increase in the demand for radiological tests.
Multiple studies found that patients with symptoms, which should have raised concern for recurrence, did not have expedited clinical review. This could be because patients did not inform their clinical team of new symptoms. If so, this is somewhat at odds with the findings from Lorenc et al. of high levels of confidence amongst HNC survivors in contacting the clinic upon identifying symptoms (33). This perhaps reflects the self-selection of patients with high levels of understanding and engagement who participated in the interview study. Patients who were interviewed also had higher rates of post-graduate education than the pool of HNC survivors they were drawn from (37.9% versus 29.5%) possibly meaning they were generally better informed. The issue of patient awareness highlights the need for patient education about red flag symptoms and self-examination. INTEGRATE audited patient education about red flag symptoms, as part of UK guidance for HNC follow-up consultations, and found documentation of verbal information-giving in 20.2% of appointments and written in 0.2% (16). This indicates significant room for improvement but could also reflect incomplete documentation.
Limitations of evidence
4.2
Very few studies pre-defined the symptoms which patients were asked about during follow-up. Despite this, expected symptoms of HNC recurrence such as pain and dysphagia arose repeatedly. Presumably these symptoms were elicited or volunteered by patients and recorded because they are known to be associated with HNC presentations. However, it is unclear whether this represents a complete picture of patients’ symptoms for example dry mouth, sore mouth and dental issues are very common patient-reported concerns, but these were not well represented. Most studies in this review were retrospective in nature. It is probable that there is missing data where symptoms deemed to be less important have not been recorded. This along with the lack of pre-defined symptoms means that it is not possible to draw any strong conclusions.
The patient populations in the included studies are very heterogenous; reflected in the wide range of sensitivity (9.1-100%) for patient reported symptoms. The overall prevalence of symptoms in patients after treatment for HNC is poorly described and therefore it is not possible to determine the extent to which patient-reported measures could have a meaningful role in identifying the presence of recurrence. The rate of recurrence reported in the included studies is hugely variable but particularly low for the studies which reported sufficient data to calculate PPV and NPV. Given these values are both dependent on the population prevalence, these results should be interpreted with caution.
Limitations of the review
4.3
Despite the terms employed in the literature search being broad, many papers were found via references and citations rather than the initial search. Regardless, the authors are confident that this approach including grey literature sources has yielded a complete picture of the available evidence on this subject. As mentioned earlier there are no valid risk-of-bias tools for observational cohort studies of this nature however we have based reporting on an existing tool and have captured the common concerns about these studies.
This review includes a heterogenous group of patients in terms of primary site, stage, treatment modality and tumour HPV-status. Tests of sensitivity and specificity are specific to the population and the population prevalence of the outcome of interest, both of which are highly variable in these studies. The tests of diagnostic power should therefore be interpreted with a significant degree of caution. This is reflected in the wide range of sensitivity and specificity values amongst the studies. This warrants further investigation with data segregated by disease subsite and with prospective collection of symptom data.
Implications of the results
4.4
This review suggests that symptoms in isolation are not a reliable method of detection of HNC recurrence. As patients are very unlikely to have a recurrence in the absence of symptoms, we should consider whether follow-up based primarily around recurrence detection is in patients’ best interest. Patients can have life-long morbidity after HNC diagnosis and treatment (34). For some patients, psychological morbidity including fear of cancer recurrence and body image disturbance are more pronounced than physical concerns. These aspects might be better managed in a different setting by alternative healthcare professionals e.g. Cancer Nurse Specialists (CNS) and clinical psychologists. There is a concern that PIFU models of surveillance after treatment could delay the identification of some recurrence presentations. We may question whether reliance on PIFU is justified when the outcomes of salvage treatments are generally more favourable in early stage, small volume disease.
Some studies reported that patients were experiencing symptoms at their consultation, but they were seen at a routine visit, i.e. they had not expedited their follow-up appointment. We must ensure patients are equipped with the knowledge and skills required to maximise symptom detection by educating them about red flag symptoms, empowering them to highlight to clinicians when they might be experiencing them and provide a route for urgent review.
To more accurately address the question of whether patient-reported signs and symptoms could be used to detect recurrence, patients should be asked to report all symptoms in a reliable and repeatable manner. Use of validated patient-reported outcome measures would be ideal but there should also be consensus on the measures used to compare outcomes across treatment centres. Digital tools such as smartphone applications may be useful to encourage patients to record and report signs and symptoms on a regular basis to identify symptom trends. International collaberators have already embarked on creating such as system in HNC (35). In the future, artificial intelligence tools may be trained to handle large datasets and identify common patterns which may predict recurrence however for this to be possible, accurate and more granular prospective data must be available.
Conclusion
5
The specificity of patient-reported symptoms is good meaning if patients do not report new or worsening symptoms, clinical teams can be reassured that the chance of recurrent disease is low. However, sensitivity is very poor in some studies therefore patient-reported signs and symptoms in isolation are not a reliable means of recurrence or SP detection. This question needs further investigation using prospective, pre-defined symptom data to build a complete picture of the prevalence of symptoms in the HNC follow-up population. Patient education, collection of data via digital symptom-tracking and the use of validated PROMs may optimise the diagnostic yield of patient-reported signs and symptoms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cancer Research UK. Head and neck cancer incidence statistics . Available online at: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/head-and-neck-cancers (Accessed 9/7/2024).
- 2Bulbul MG Genovese TJ Hagan K Rege S Qureshi A Varvares MA. Salvage surgery for recurrent squamous cell carcinoma of the head and neck: Systematic review and meta-analysis. Head Neck. (2022) 44:275–85. doi: 10.1002/hed.26898 34729845 · doi ↗ · pubmed ↗
- 3Goodwin WJ Jr. Salvage surgery for patients with recurrent squamous cell carcinoma of the upper aerodigestive tract: when do the ends justify the means? Laryngoscope . (2000) 110:1–18. doi: 10.1097/00005537-200003001-00001 10714711 · doi ↗ · pubmed ↗
- 4Homer JJ Winter SC. Head and neck cancer: United Kingdom national multidisciplinary guidelines, sixth edition. J Laryngol Otol. (2024) 138:S 31. doi: 10.1017/S 0022215123001615 38682705 · doi ↗ · pubmed ↗
- 5Mc Laren O Perkins C Zhu Y Smith M Williams R. Patient perspectives on surveillance after head and neck cancer treatment: A systematic review. Clin Otolaryngol. (2021) 46:1345–53. doi: 10.1111/coa.13846 34363645 · doi ↗ · pubmed ↗
- 6Dretzke J Chaudri T Balaji R Mehanna H Nankivell P Moore DJ. PETNECK 2 Research Team. A systematic review of the effectiveness of patient-initiated follow-up after cancer. Cancer Med. (2023) 12:19057–71. doi: 10.1002/cam 4.v 12.18 PMC 1055786737602830 · doi ↗ · pubmed ↗
- 7Nankivell P Gaunt P Gaunt C Sissons J Liaskou E Jefferson Y. PETNECK 2 Research Team. PET-CT-guided, symptom-based, patient-initiated surveillance versus clinical follow-up in head neck cancer patients (PETNECK 2): study protocol for a multicentre feasibility study and non-inferiority, randomised, phase III trial. BMC Cancer. (2024) 24:823. doi: 10.1186/s 12885-024-12470-9 38987693 PMC 11234619 · doi ↗ · pubmed ↗
- 8Page MJ Mc Kenzie JE Bossuyt PM Boutron I Hoffmann TC Mulrow CD. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n 71. doi: 10.1136/bmj.n 71 33782057 PMC 8005924 · doi ↗ · pubmed ↗